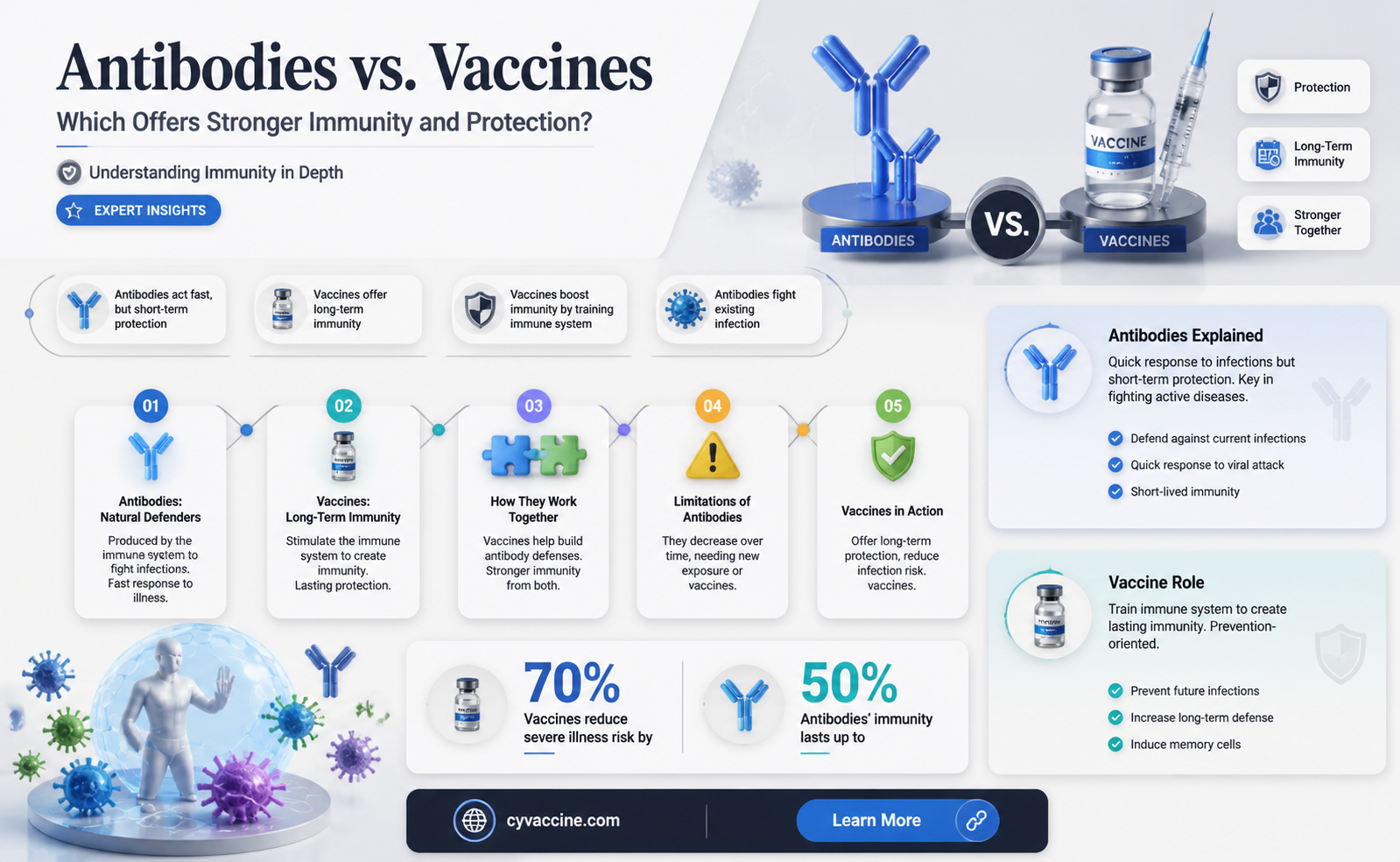
The question of whether antibodies are stronger than vaccines is a nuanced one, as both play distinct yet complementary roles in the immune system. Antibodies, which are proteins produced by the body in response to an infection or vaccination, provide immediate and targeted defense against specific pathogens. However, their effectiveness is often temporary and depends on the individual’s immune response. Vaccines, on the other hand, stimulate the immune system to generate a memory response, preparing it to produce antibodies more efficiently if exposed to the pathogen in the future. While antibodies offer rapid protection, vaccines provide long-term immunity and broader defense, making them a more robust and sustainable solution for preventing diseases. Thus, rather than comparing their strength, it’s more accurate to view them as synergistic tools in the fight against infectious diseases.
Explore related products






What You'll Learn
- Antibody vs. Vaccine Duration: How long does protection last for each method
- Efficacy Comparison: Which provides better defense against pathogens
- Side Effects: Are antibodies safer than vaccine reactions
- Cost and Accessibility: Which is more affordable and widely available
- Natural vs. Induced Immunity: Which offers superior immune response
![]()
Antibody vs. Vaccine Duration: How long does protection last for each method?
Antibodies, whether naturally produced after an infection or administered through monoclonal antibody treatments, offer immediate but temporary protection against pathogens. For instance, after recovering from COVID-19, natural antibodies typically peak within 1–2 months and may wane significantly after 6–12 months, leaving individuals vulnerable to reinfection. Monoclonal antibody treatments, such as those used for COVID-19, provide a rapid immune boost but last only a few weeks to months, depending on the dosage (e.g., a single 900 mg infusion of bamlanivimab offers protection for approximately 3 months). This short-term defense is useful for high-risk individuals but requires repeated administration for sustained protection.
Vaccines, on the other hand, are designed to confer long-term immunity by training the immune system to recognize and combat pathogens. For example, the mRNA COVID-19 vaccines (Pfizer and Moderna) provide robust protection for at least 6 months after the second dose, with studies showing efficacy rates above 90% during this period. Booster shots, typically administered 6–12 months later, extend this protection further. Similarly, childhood vaccines like the MMR (measles, mumps, rubella) offer lifelong immunity after a two-dose series, while others, such as the Tdap (tetanus, diphtheria, pertussis), require boosters every 10 years. This prolonged duration makes vaccines a cornerstone of public health, reducing disease transmission and preventing outbreaks.
Comparing the two, antibodies provide a quick fix but are fleeting, while vaccines build a durable immune memory. For instance, a person who receives monoclonal antibodies for Ebola gains immediate protection but must rely on vaccines like Ervebo for long-term defense, which has shown efficacy for at least 2 years in clinical trials. This distinction highlights the complementary roles of antibodies and vaccines: antibodies are ideal for urgent, short-term needs, while vaccines are the gold standard for sustained population-level immunity.
Practical considerations further emphasize the differences. Antibody treatments are often reserved for specific populations, such as immunocompromised individuals who may not mount a strong vaccine response. Vaccines, however, are widely accessible and cost-effective, with global vaccination campaigns reaching billions of people annually. For optimal protection, combining both approaches—such as using monoclonal antibodies during an outbreak while promoting widespread vaccination—can maximize immunity and reduce disease burden. Understanding these durations and mechanisms empowers individuals and healthcare providers to make informed decisions tailored to their needs.
United Airlines Employee Vaccination Rates: A Comprehensive Overview
You may want to see also
Explore related products






![]()
Efficacy Comparison: Which provides better defense against pathogens?
Antibodies and vaccines both play critical roles in defending the body against pathogens, but their mechanisms and efficacy differ significantly. Antibodies, also known as immunoglobulins, are proteins produced by the immune system in response to a specific antigen, such as a virus or bacterium. They act as a rapid defense, neutralizing pathogens before they can cause harm. Vaccines, on the other hand, are biological preparations that stimulate the immune system to recognize and combat pathogens, often by introducing a weakened or inactivated form of the pathogen. This comparison highlights the distinct advantages and limitations of each approach in providing protection.
Consider the immediate response to a pathogen. When exposed to a virus like influenza, individuals with pre-existing antibodies—either from a previous infection or a monoclonal antibody treatment—may experience milder symptoms or no illness at all. For instance, monoclonal antibody treatments for COVID-19, such as those containing casirivimab and imdevimab, have been shown to reduce hospitalization rates by up to 70% when administered within 10 days of symptom onset. However, this protection is short-lived, typically lasting only a few weeks to months. Vaccines, in contrast, provide a more durable defense by training the immune system to produce its own antibodies and memory cells. A single dose of the Pfizer-BioNTech COVID-19 vaccine, for example, offers approximately 52% efficacy against symptomatic infection after two weeks, rising to 95% after the second dose.
The longevity of protection is a key differentiator. Antibodies from natural infection or passive immunization wane over time, leaving individuals vulnerable to reinfection. For example, studies show that COVID-19 antibodies from natural infection can decline significantly within 6–12 months. Vaccines, however, often confer long-term immunity by creating immunological memory. The measles vaccine, for instance, provides lifelong protection in 95% of recipients after two doses. Booster shots can further extend this immunity, as seen with the tetanus vaccine, which requires boosters every 10 years to maintain optimal protection.
Practical considerations also influence the choice between antibodies and vaccines. Antibody treatments are typically reserved for high-risk individuals or those with compromised immune systems, as they are costly and require intravenous or subcutaneous administration. Vaccines, in contrast, are more accessible and cost-effective for population-wide protection. For example, the annual influenza vaccine is recommended for everyone aged 6 months and older, with specific formulations tailored for children, adults, and seniors. This broad applicability makes vaccines a cornerstone of public health strategies.
In conclusion, while antibodies offer immediate and potent protection against pathogens, vaccines provide a more sustainable and scalable defense. Antibodies are invaluable in acute situations, such as treating severe infections or preventing disease in immunocompromised individuals. Vaccines, however, remain the gold standard for long-term immunity and disease prevention at the population level. Understanding these differences allows for informed decisions in both personal health management and public health policy.
Understanding Why Some Children Cannot Receive Vaccinations: Key Factors Explained
You may want to see also
Explore related products






![]()
Side Effects: Are antibodies safer than vaccine reactions?
Antibodies, whether naturally acquired or administered through treatments like monoclonal antibody therapies, are often perceived as a gentler alternative to vaccines due to their targeted action against specific pathogens. However, the safety profile of antibodies versus vaccine reactions is not as straightforward as it seems. While vaccines can trigger side effects such as fever, fatigue, or injection site pain, these are typically mild and short-lived, serving as signs of the immune system’s activation. Antibody treatments, on the other hand, may carry risks like allergic reactions, anaphylaxis, or even immune system dysregulation, particularly in high-dose regimens. For instance, COVID-19 monoclonal antibody infusions have been associated with rare but severe side effects, including rapid heartbeat and shortness of breath, requiring immediate medical attention.
Consider the practical implications for different age groups. Vaccines are rigorously tested across populations, including children and the elderly, with well-documented safety profiles. For example, the flu vaccine is recommended annually for individuals over six months old, with side effects limited to soreness or low-grade fever in most cases. Antibody treatments, however, are often reserved for specific high-risk groups, such as immunocompromised patients or those with severe infections, and may not be suitable for widespread use due to their potential risks. A 70-year-old with a weakened immune system might benefit from monoclonal antibodies during a COVID-19 infection but could face a higher risk of adverse reactions compared to a healthy 30-year-old receiving a vaccine.
From a comparative standpoint, vaccines offer long-term immunity by training the immune system to recognize and combat pathogens, whereas antibodies provide immediate but temporary protection. This distinction influences their side effect profiles. Vaccines may cause discomfort during the immune response training phase, but their benefits far outweigh these transient effects. Antibodies, while effective in urgent situations, lack the preventive aspect of vaccines and may require repeated doses, increasing the cumulative risk of side effects. For instance, a single dose of the Pfizer-BioNTech COVID-19 vaccine (30 µg) has a well-tolerated side effect profile, whereas multiple doses of monoclonal antibodies (e.g., 2,400 mg of bamlanivimab) could amplify risks like infusion reactions.
To navigate this dilemma, individuals should weigh the urgency of their situation against the potential risks. If exposed to a pathogen and at high risk of severe illness, antibody treatment might be the safer immediate option despite its side effects. However, for long-term protection and minimal risk, vaccines remain the preferred choice. Practical tips include monitoring for severe reactions post-antibody treatment (e.g., difficulty breathing or swelling) and staying hydrated after vaccination to alleviate mild symptoms. Ultimately, while antibodies can be lifesaving in critical scenarios, vaccines offer a safer, more sustainable approach to disease prevention.
Vaccine Courts: Billions Paid Out - Fact or Fiction?
You may want to see also
Explore related products






![]()
Cost and Accessibility: Which is more affordable and widely available?
Antibodies, whether naturally produced or administered via monoclonal antibody treatments, come with a steep price tag. For instance, a single dose of monoclonal antibody treatment for COVID-19 can cost upwards of $2,000 per patient, and multiple doses may be required for sustained protection. In contrast, vaccines are significantly more affordable, with many COVID-19 vaccines priced between $10 to $40 per dose, often subsidized by governments or covered by insurance. This stark difference in cost highlights a critical barrier to accessibility for antibody treatments, especially in low-resource settings.
Consider the logistics of distribution: vaccines are typically administered in standardized doses, often requiring only one or two shots for full immunity. For example, the Pfizer-BioNTech COVID-19 vaccine is given in two 0.3 mL doses, spaced 3–4 weeks apart, for individuals aged 12 and older. Antibody treatments, however, often require intravenous infusion, which demands trained healthcare personnel and specialized facilities. This complexity not only increases costs but also limits availability, particularly in rural or underdeveloped areas where such infrastructure is scarce.
From a public health perspective, vaccines are a more scalable solution. They can be mass-produced, stored (many at standard refrigeration temperatures), and distributed efficiently, reaching millions of people through existing immunization programs. Antibody treatments, on the other hand, are often reserved for high-risk individuals or those already infected, making them less practical for widespread preventive use. For example, while a vaccine campaign can target entire populations, monoclonal antibody treatments are typically prioritized for elderly patients or those with comorbidities, leaving others without access.
A persuasive argument for vaccines lies in their long-term cost-effectiveness. Vaccines not only prevent infection but also reduce the burden on healthcare systems by minimizing severe cases and hospitalizations. For instance, a study by the CDC estimated that COVID-19 vaccination prevented over 140,000 deaths and 4 million infections in the U.S. by June 2021, saving billions in healthcare costs. Antibody treatments, while lifesaving in certain cases, address the symptom rather than the root cause, making them a less sustainable solution for population-wide protection.
In conclusion, while antibody treatments play a crucial role in managing specific cases, vaccines emerge as the more affordable and accessible option for broad immunity. Practical tips for maximizing vaccine accessibility include advocating for global distribution initiatives, such as COVAX, and supporting local vaccination drives. For those considering antibody treatments, consult healthcare providers to weigh the benefits against the logistical and financial challenges, ensuring informed decision-making in both individual and public health contexts.
Government vs. Private Vaccination: Key Differences and What They Mean for You
You may want to see also
Explore related products






![]()
Natural vs. Induced Immunity: Which offers superior immune response?
The human immune system is a marvel of biological engineering, capable of distinguishing between the body's own cells and foreign invaders. When it comes to immunity, the debate between natural and induced (vaccine-derived) immunity often centers on which provides a more robust and lasting defense. Natural immunity, acquired through infection, involves the body's full-scale response to a pathogen, often leading to the production of a wide array of antibodies and memory cells. In contrast, induced immunity, achieved through vaccination, typically targets specific antigens, stimulating a focused immune response without the risks associated with the disease itself.
Consider the case of COVID-19. Studies have shown that individuals who recover from SARS-CoV-2 infection develop a diverse set of antibodies, including neutralizing antibodies that prevent the virus from entering cells. However, this natural immunity comes at a cost: the risk of severe illness, long-term health complications, and even death. Vaccines, on the other hand, provide a safer alternative by introducing a harmless component of the virus (e.g., mRNA or a viral vector) to trigger an immune response. For instance, the Pfizer-BioNTech COVID-19 vaccine delivers a dose of 30 micrograms of mRNA encoding the virus’s spike protein, prompting the production of targeted antibodies and memory cells without exposing the individual to the virus itself.
From an analytical perspective, the durability of immunity is a critical factor. Natural immunity often wanes over time, as observed with seasonal coronaviruses, where reinfections are common after 1–3 years. Vaccines, however, can be engineered to enhance longevity. Booster shots, such as the 50-microgram Pfizer-BioNTech COVID-19 booster, reinforce memory cell populations, extending protection. Additionally, vaccines can be updated to target emerging variants, a flexibility natural immunity lacks. For example, the bivalent COVID-19 boosters introduced in 2022 address both the original strain and Omicron subvariants, offering broader protection than natural immunity alone.
Practically speaking, the choice between natural and induced immunity is not one of equivalence but of risk management. For healthy individuals under 65, natural immunity might provide adequate protection against mild reinfection, but the potential for severe outcomes remains a gamble. Vaccination, particularly for vulnerable populations (e.g., the elderly or immunocompromised), is a safer and more controlled approach. For instance, the CDC recommends COVID-19 vaccination for everyone aged 6 months and older, with additional doses for those over 65 or with weakened immune systems. This tailored approach maximizes benefits while minimizing risks.
In conclusion, while natural immunity can be potent, its acquisition is fraught with danger and uncertainty. Induced immunity, through vaccination, offers a safer, more predictable, and adaptable solution. By understanding the mechanisms and limitations of both, individuals and healthcare providers can make informed decisions to optimize immune protection. Whether through a 30-microgram mRNA dose or a strategic booster regimen, the goal remains the same: to build a resilient defense against pathogens without compromising health.
Understanding the Meningococcal B Vaccine: Benefits, Risks, and Importance
You may want to see also
Frequently asked questions
Antibodies and vaccines serve different purposes. Antibodies provide immediate protection by neutralizing pathogens, while vaccines stimulate the immune system to produce antibodies and memory cells for long-term immunity. Neither is inherently "stronger"—they complement each other.
No, antibodies cannot replace vaccines. Antibodies from sources like monoclonal antibody treatments or natural infection provide temporary protection, whereas vaccines offer durable immunity by training the immune system to respond effectively in the future.
Vaccines provide longer-lasting immunity. They create immunological memory, allowing the body to quickly produce antibodies if exposed to the pathogen again. Antibodies from infection or treatment typically wane over time.
No, relying on natural antibodies from infection is riskier than getting vaccinated. Infections can cause severe illness or complications, while vaccines safely prepare the immune system without the dangers of the disease itself. Vaccination is the safer and more effective choice.