Antibodies and vaccines, while both crucial in the fight against diseases, serve distinct roles in the immune system. Antibodies are proteins produced by the body’s immune cells, specifically B cells, in response to the presence of foreign invaders like viruses or bacteria. They act as targeted defenders, neutralizing or marking pathogens for destruction. Vaccines, on the other hand, are biological preparations that stimulate the immune system to recognize and combat specific pathogens without causing the disease itself. They work by introducing a harmless form of the pathogen or its components, prompting the body to produce antibodies and memory cells, which provide long-term protection against future infections. While antibodies are the immune system’s immediate response, vaccines are a preventive measure designed to train the body to generate these antibodies efficiently. Understanding the difference between the two is essential for appreciating how they collectively contribute to immunity and public health.
| Characteristics | Values |
|---|---|
| Definition | Antibodies are proteins produced by the immune system to neutralize pathogens. Vaccines are biological preparations that stimulate the immune system to produce antibodies. |
| Origin | Antibodies are naturally produced by B cells in response to an infection or vaccination. Vaccines are artificially created using weakened/killed pathogens, viral vectors, mRNA, or proteins. |
| Function | Antibodies directly neutralize or tag pathogens for destruction. Vaccines induce the immune system to produce antibodies and memory cells for future protection. |
| Duration | Antibodies can last weeks to years, depending on the type and exposure. Vaccine-induced immunity can last years to a lifetime, depending on the vaccine. |
| Administration | Antibodies are naturally produced or administered as therapy (e.g., monoclonal antibodies). Vaccines are administered via injection, nasal spray, or oral route. |
| Purpose | Antibodies treat or prevent active infections. Vaccines prevent infections by preparing the immune system. |
| Specificity | Antibodies target specific antigens on pathogens. Vaccines target specific pathogens or their components. |
| Immune Response | Antibodies are part of the adaptive immune response. Vaccines stimulate both innate and adaptive immune responses. |
| Examples | IgG, IgM, IgA (antibodies). COVID-19 vaccines (Pfizer, Moderna), flu vaccines (vaccines). |
| Side Effects | Antibody therapy may cause allergic reactions. Vaccines may cause mild side effects (e.g., soreness, fever). |
| Development Time | Antibodies are produced within days to weeks after exposure. Vaccines take weeks to months to induce full immunity. |
| Passive vs. Active | Antibodies can be passively transferred (e.g., monoclonal antibodies). Vaccines provide active immunity through immune system stimulation. |
Explore related products





What You'll Learn
![]()
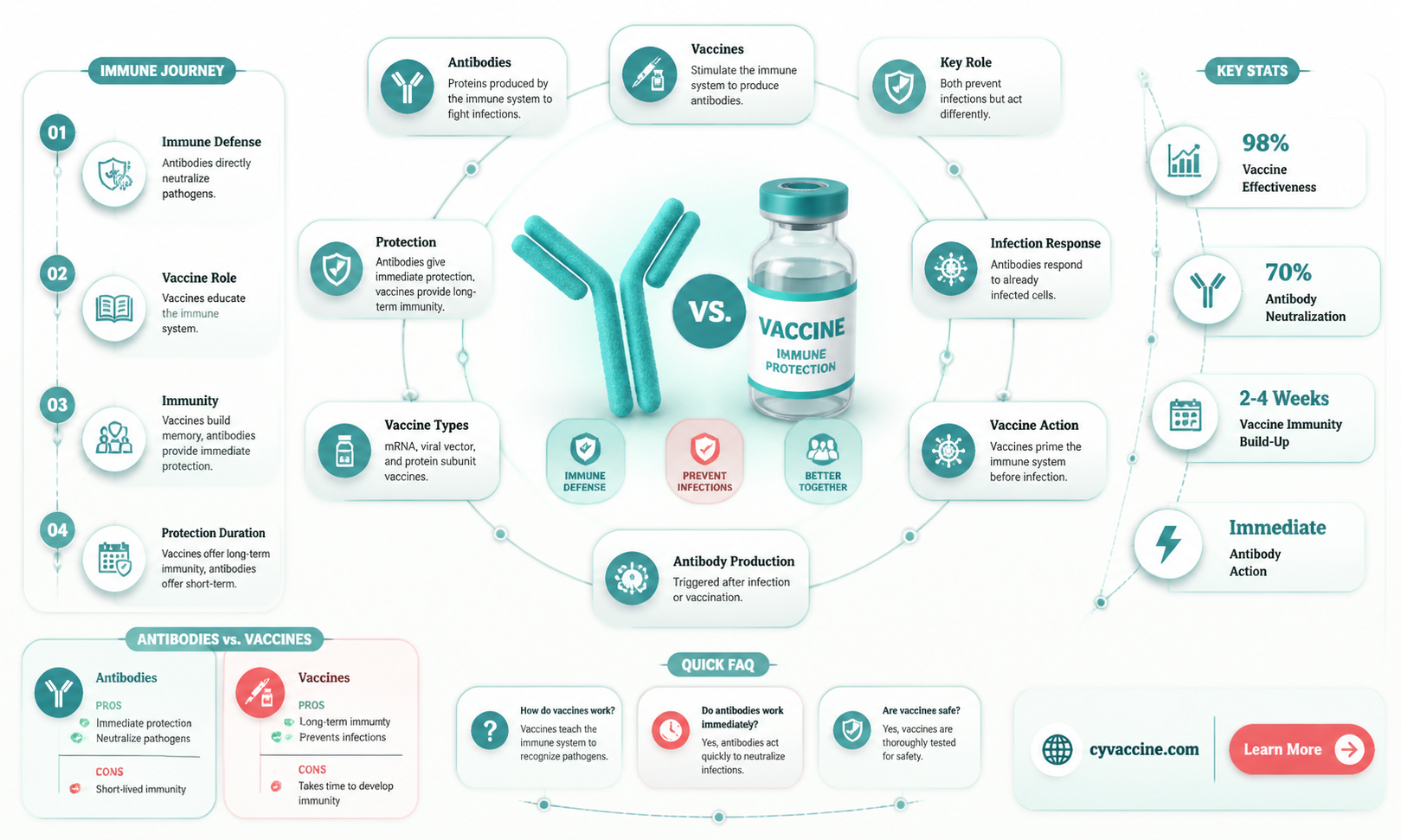
Antibody Function vs. Vaccine Purpose
Antibodies and vaccines, though interconnected, serve distinct roles in the immune system. Antibodies, also known as immunoglobulins, are Y-shaped proteins produced by B cells in response to foreign invaders like viruses or bacteria. Their primary function is to neutralize pathogens by binding to specific antigens, marking them for destruction by other immune cells or directly blocking their ability to infect cells. For instance, after a COVID-19 infection, the body produces antibodies targeting the virus’s spike protein, preventing it from entering human cells. Vaccines, on the other hand, are biological preparations that introduce a harmless form of a pathogen (or its components) to the immune system, training it to recognize and combat future threats. While antibodies act as the immune system’s immediate defense force, vaccines are the strategic training program that prepares the body for potential attacks.
Consider the process of vaccination as a rehearsal for the immune system. When a vaccine, such as the mRNA COVID-19 vaccine, is administered, it delivers genetic instructions for cells to produce a harmless piece of the virus’s spike protein. The immune system identifies this protein as foreign, prompting B cells to produce antibodies and memory cells. These memory cells remain dormant but ready to mount a rapid response if the actual virus is encountered. Antibodies generated post-vaccination can persist for months or years, depending on the vaccine and individual immune response. For example, the measles vaccine confers lifelong immunity, while the flu vaccine requires annual administration due to the virus’s rapid mutation. Vaccines, therefore, are not a direct source of antibodies but a catalyst for their production and long-term immune preparedness.
A critical distinction lies in the timing and purpose of antibody function versus vaccine purpose. Antibodies are reactive, appearing only after exposure to a pathogen or vaccine. They provide immediate protection but wane over time, requiring booster doses for sustained immunity. Vaccines, however, are proactive, designed to prevent infections before they occur. For instance, the HPV vaccine is administered to adolescents (ages 9–14) in a two-dose schedule, offering protection against strains linked to cervical cancer. Here, the vaccine’s purpose is not to generate antibodies for immediate use but to establish a robust immune memory that can prevent future infections. This preventive approach underscores the vaccine’s role as a long-term investment in health, distinct from the short-term action of antibodies.
Practical considerations further highlight the differences. Antibody treatments, like monoclonal antibody infusions used for severe COVID-19 cases, provide instant immunity but are costly and require precise timing. Vaccines, while not offering immediate protection (typically taking 2–4 weeks to build immunity), are cost-effective and scalable, making them a cornerstone of public health. For example, the polio vaccine has nearly eradicated the disease globally through widespread immunization campaigns. Understanding these distinctions is crucial for informed decision-making, whether scheduling vaccinations for children or evaluating treatments during outbreaks. Antibodies and vaccines are not interchangeable but complementary tools in the fight against infectious diseases.
Oval Rabies Vaccination Tags: Materials and Composition Explained
You may want to see also
Explore related products





![]()
Natural vs. Vaccine-Induced Immunity
Antibodies and vaccines are not the same, though they are closely related in the context of immunity. Antibodies are proteins produced by the immune system to neutralize pathogens, while vaccines are biological preparations that stimulate the immune system to produce antibodies and memory cells for future protection. This distinction leads to a critical comparison: natural immunity, acquired through infection, versus vaccine-induced immunity, achieved through immunization.
Natural immunity develops when the body encounters a pathogen directly. During an infection, the immune system identifies the threat, mounts a response, and often retains memory cells to recognize the pathogen faster in future encounters. For example, surviving a measles infection typically confers lifelong immunity. However, this process comes with risks. Severe illness, long-term complications (e.g., myocarditis from COVID-19), or even death can occur before immunity is established. The immune response varies by individual, and the antibody levels produced may wane over time, leaving gaps in protection. For instance, natural immunity to pertussis (whooping cough) lasts 4–20 years, requiring repeated exposure to maintain defense—a dangerous proposition given the disease’s severity.
Vaccine-induced immunity bypasses the risks of natural infection by training the immune system safely. Vaccines introduce a weakened, inactivated, or fragment of the pathogen (e.g., mRNA in COVID-19 vaccines) to trigger a controlled immune response. This method produces antibodies and memory cells without exposing the individual to the disease’s dangers. For example, the MMR vaccine provides measles immunity in 97% of recipients after two doses, comparable to natural infection but without the risk of complications like encephalitis. Vaccines also standardize the immune response, ensuring consistent protection across populations. Booster doses, such as the Tdap vaccine for tetanus, diphtheria, and pertussis, are administered every 10 years to maintain antibody levels, offering predictable and manageable immunity.
Comparing the two, vaccine-induced immunity is often more reliable and safer. Natural immunity’s strength depends on the severity of the initial infection, which is unpredictable. In contrast, vaccines deliver a precise antigen dose, optimized for efficacy. For instance, the hepatitis B vaccine series (three doses over 6 months) provides over 90% protection, whereas natural immunity varies widely based on the infection’s course. Additionally, vaccines protect vulnerable populations indirectly through herd immunity, reducing disease circulation. Natural immunity does not offer this societal benefit, as it relies on individuals contracting and surviving the disease.
Practical considerations favor vaccine-induced immunity in most cases. Vaccines are particularly crucial for high-risk groups, such as the elderly, immunocompromised individuals, and children under 5, who may face severe outcomes from natural infections. For example, the flu vaccine, though imperfect, reduces hospitalizations in children by 40–60%. While natural immunity can be robust, its acquisition is fraught with danger and uncertainty. Vaccines provide a controlled, measurable, and safer path to immunity, making them the cornerstone of public health strategies against infectious diseases.
When Can You Book CVS Vaccine Appointments? Timing Tips Revealed
You may want to see also
Explore related products





![]()
Passive Antibodies vs. Active Vaccination
Antibodies and vaccines are not the same, though they both play critical roles in immune protection. Antibodies are proteins produced by the immune system to neutralize pathogens, while vaccines are biological preparations that stimulate the immune system to produce its own antibodies. This distinction becomes clearer when comparing passive antibodies and active vaccination, two fundamentally different approaches to immunity.
Passive antibody therapy involves the direct administration of pre-formed antibodies to provide immediate, short-term protection against a specific pathogen. For example, monoclonal antibody treatments like casirivimab and imdevimab have been used to treat COVID-19 in high-risk patients. These antibodies are typically given intravenously in doses ranging from 1,200 to 2,400 mg, depending on the patient’s weight and condition. The key advantage is speed: protection is instantaneous, making it ideal for emergencies or immunocompromised individuals who cannot mount an immune response. However, this protection wanes within weeks to months, as the body does not produce additional antibodies. Practical considerations include the need for refrigeration, potential allergic reactions, and the high cost of treatment.
In contrast, active vaccination stimulates the body’s own immune system to produce antibodies and memory cells, offering long-term protection. Vaccines like the mRNA COVID-19 vaccines (Pfizer-BioNTech and Moderna) require a series of doses (typically 30–100 µg per shot) spaced weeks apart to build robust immunity. The process is slower, as it relies on the immune system’s response, but the protection lasts for years or even decades. For instance, the measles vaccine provides lifelong immunity after two doses, administered at 12–15 months and 4–6 years of age. Active vaccination also confers herd immunity, reducing disease transmission in communities. However, it is less effective in individuals with weakened immune systems, highlighting the complementary roles of passive and active strategies.
The choice between passive antibodies and active vaccination depends on context. Passive therapy is a lifeline in acute situations, such as preventing rabies after a bite or treating severe infections in newborns. Active vaccination, however, is the cornerstone of public health, preventing diseases like polio and influenza on a population scale. For travelers to high-risk areas, a combination approach may be used: a vaccine series for long-term protection supplemented by passive antibodies for immediate coverage. Understanding these differences empowers individuals and healthcare providers to make informed decisions tailored to specific needs.
Pet Lyme Disease Vaccinations: How Often?
You may want to see also
Explore related products






![]()
Duration of Antibody Protection vs. Vaccines
Antibodies and vaccines are not the same, yet their interplay is crucial for understanding immunity duration. Antibodies, whether naturally produced after infection or administered via monoclonal antibody treatments, provide immediate but temporary protection, typically lasting weeks to months. Vaccines, on the other hand, stimulate the immune system to produce antibodies and memory cells, offering longer-lasting immunity, often years to a lifetime, depending on the vaccine. For instance, the flu vaccine requires annual administration due to viral mutations, while the measles vaccine confers lifelong protection in most cases.
Consider the COVID-19 pandemic, where this distinction became starkly evident. Monoclonal antibody treatments like Regeneron offered rapid protection for high-risk individuals but waned within 3–6 months. In contrast, mRNA vaccines (Pfizer, Moderna) induced robust antibody responses and memory B cells, with protection lasting over a year, though boosters became necessary due to variants and waning immunity. Dosage plays a role too: a standard COVID-19 vaccine dose (30 µg for Pfizer) provides solid initial protection, but a booster (same dosage) significantly extends immunity by reactivating memory cells.
The duration of antibody protection also varies by age and health status. In older adults or immunocompromised individuals, both natural and vaccine-induced antibodies may decline faster. For example, a 70-year-old might require a COVID-19 booster every 6 months, while a healthy 30-year-old could wait a year. Practical tip: monitor antibody levels via blood tests if you’re at risk, and consult a healthcare provider to tailor your vaccination schedule.
Comparatively, vaccines are designed to outlast natural antibody responses. The hepatitis B vaccine, for instance, provides protection for 20+ years after a 3-dose series, while natural infection antibodies might wane after 6 months. This highlights vaccines’ ability to mimic and enhance the immune system’s memory, ensuring prolonged defense against pathogens. However, no vaccine is perfect; some, like the tetanus shot, require periodic boosters every 10 years to maintain immunity.
In summary, while antibodies offer immediate protection, vaccines provide a sustained immune response through memory cells. Understanding this difference is key to optimizing immunity. For maximum protection, combine timely vaccinations with awareness of individual health factors, and stay updated on booster recommendations. After all, immunity isn’t just about antibodies—it’s about building a resilient immune memory.
Should Childhood Vaccinations Be Mandatory? A Parent's Responsibility Debate
You may want to see also
Explore related products






![]()
How Vaccines Stimulate Antibody Production
Vaccines are not antibodies, but they are the architects that orchestrate their creation. At their core, vaccines introduce a harmless piece of a pathogen—such as a protein or weakened virus—to the immune system. This triggers a cascade of events that culminates in antibody production. For instance, the mRNA vaccines for COVID-19 deliver genetic instructions to cells, prompting them to produce the SARS-CoV-2 spike protein. The immune system recognizes this protein as foreign, activating B cells to mature into plasma cells that secrete antibodies tailored to neutralize the threat.
Consider the process as a military training exercise. The vaccine acts as a drill sergeant, exposing the immune system to a simulated enemy (the antigen). B cells, the recruits, learn to identify and combat this invader. Once trained, memory B cells remain on standby, ready to rapidly produce antibodies if the real pathogen ever attacks. This is why a second vaccine dose, typically administered 3–4 weeks later, boosts antibody levels significantly—it reinforces the training, ensuring a swift and robust response.
The effectiveness of this process depends on several factors, including vaccine type, dosage, and individual immune health. For example, the influenza vaccine requires annual updates because the virus mutates frequently, necessitating new antigen targets. In contrast, the measles vaccine provides lifelong immunity with just two doses, usually given at 12–15 months and 4–6 years of age. Practical tips for maximizing antibody production include staying hydrated, maintaining a balanced diet rich in vitamins C and D, and avoiding excessive stress, as these factors support optimal immune function.
A critical distinction lies in the active versus passive nature of this process. Vaccines stimulate the body to produce its own antibodies, a proactive and long-lasting defense mechanism. In contrast, antibody therapies, like monoclonal antibodies, provide ready-made antibodies for immediate but temporary protection. While vaccines train the immune system for future battles, antibody treatments are akin to deploying a special forces unit to address an ongoing crisis. Understanding this difference highlights the unique role of vaccines in fostering self-sufficiency in immune defense.
Navigating Illinois Vaccine Exemption Form: My Step-by-Step Process
You may want to see also
Frequently asked questions
No, antibodies and vaccines are not the same. Antibodies are proteins produced by the immune system to fight off specific pathogens, while vaccines are substances administered to stimulate the immune system to produce antibodies and provide immunity against a disease.
Most vaccines do not directly provide antibodies. Instead, they introduce a weakened or inactivated form of a pathogen (or its components) to train the immune system to produce its own antibodies. However, some vaccines, like monoclonal antibody treatments, can directly provide antibodies for immediate protection.
No, the antibodies produced in response to vaccines do not always last forever. Their duration varies depending on the vaccine and the individual. Booster shots are often needed to maintain immunity by prompting the immune system to produce more antibodies.
Yes, antibodies can be produced naturally when the body is exposed to a pathogen. However, this method carries the risk of developing the disease. Vaccines provide a safer way to generate antibodies without the risk of severe illness.
No, different vaccines target specific pathogens and stimulate the production of antibodies tailored to those pathogens. For example, the flu vaccine produces antibodies against influenza viruses, while the COVID-19 vaccine produces antibodies against the SARS-CoV-2 virus.