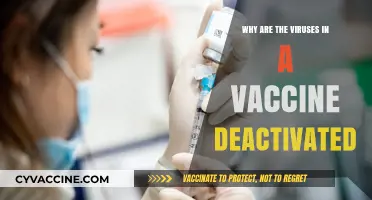
Some children are unable to receive vaccinations due to a variety of medical reasons, including severe allergies to vaccine components, compromised immune systems from conditions like HIV or cancer treatments, or specific genetic disorders. Additionally, infants under a certain age may not be eligible for certain vaccines because their immune systems are not yet developed enough to respond effectively. In rare cases, previous adverse reactions to vaccines can also prevent further immunization. These exemptions highlight the importance of herd immunity, where the majority of a population is vaccinated to protect those who cannot be, ensuring vulnerable individuals remain shielded from preventable diseases.
| Characteristics | Values |
|---|---|
| Medical Conditions | Severe allergic reaction (anaphylaxis) to a previous vaccine dose or vaccine component (e.g., gelatin, antibiotics) |
| Immunodeficiency disorders (e.g., HIV/AIDS, primary immunodeficiency) | |
| Active untreated tuberculosis | |
| Moderate or severe acute illness (with or without fever) | |
| Age Restrictions | Incomplete immune system development in infants (some vaccines not recommended before specific ages) |
| Specific vaccines not approved for certain age groups (e.g., HPV vaccine typically not given before age 9) | |
| Pregnancy | Live attenuated vaccines (e.g., MMR, varicella) generally avoided during pregnancy |
| Previous Adverse Reactions | History of severe adverse reaction to a specific vaccine or component |
| Treatment Interference | Immunosuppressive therapies (e.g., chemotherapy, high-dose steroids) |
| Recent blood transfusion or receipt of immune globulin | |
| Regional Vaccine Availability | Limited access to specific vaccines in certain regions or countries |
| Religious/Philosophical Exemptions | Parental refusal based on non-medical beliefs (varies by jurisdiction) |
| Temporary Contraindications | Mild acute illness (vaccination may be deferred until recovery) |
| Premature birth (some vaccines may be delayed based on gestational age) |
Explore related products






What You'll Learn
- Medical Conditions: Underlying health issues like immune disorders may prevent kids from receiving vaccines safely
- Allergic Reactions: Severe allergies to vaccine components can make vaccination risky for certain children
- Age Restrictions: Some vaccines are not approved for specific age groups, limiting availability for kids
- Temporary Illness: Acute illnesses may delay vaccination until the child fully recovers
- Parental Refusal: Personal beliefs or misinformation can lead parents to decline vaccines for their children
![]()
Medical Conditions: Underlying health issues like immune disorders may prevent kids from receiving vaccines safely
Children with certain medical conditions, particularly those affecting the immune system, often face unique challenges when it comes to vaccination. Immune disorders such as Severe Combined Immunodeficiency (SCID), Chronic Granulomatous Disease (CGD), or conditions requiring immunosuppressive therapies (e.g., post-organ transplant) can render live vaccines unsafe. For instance, the Measles, Mumps, and Rubella (MMR) vaccine, which uses weakened live viruses, poses a risk of causing the very disease it aims to prevent in immunocompromised individuals. This vulnerability necessitates careful evaluation by healthcare providers to balance protection against potential harm.
Consider the case of a child undergoing chemotherapy for leukemia. Their immune system, weakened by treatment, cannot safely process live vaccines like Varicella (chickenpox) or the nasal spray flu vaccine (FluMist). Instead, inactivated vaccines, such as the injectable flu shot or the hepatitis B vaccine, are recommended. Even then, timing is critical—vaccines may need to be delayed until immune function recovers, often 6–12 months post-treatment. Parents and caregivers must work closely with specialists to create a tailored vaccination plan, ensuring the child’s fragile immune system is not overwhelmed.
The decision to withhold or modify vaccines is not arbitrary; it’s rooted in evidence-based guidelines. For example, the Centers for Disease Control and Prevention (CDC) advises against live vaccines for children with HIV if their CD4 count is below a certain threshold. Similarly, children with autoimmune diseases like rheumatoid arthritis or lupus, who are on medications like corticosteroids or biologics, may require dose adjustments or alternative vaccine schedules. These precautions aim to minimize adverse reactions while maximizing immunity, often relying on antibody titers to confirm protection.
Practical tips for parents include maintaining open communication with healthcare providers, keeping detailed records of the child’s medical history, and staying informed about vaccine alternatives. For instance, if a child cannot receive the live rotavirus vaccine due to intestinal disorders like severe combined immunodeficiency, emphasis shifts to hygiene practices and environmental sanitation to prevent infection. Additionally, herd immunity becomes a critical protective factor, underscoring the importance of community vaccination rates in shielding vulnerable children.
In conclusion, while vaccines are a cornerstone of public health, they are not one-size-fits-all. For children with immune disorders, individualized approaches are essential. By understanding the interplay between medical conditions and vaccine safety, parents and healthcare providers can navigate this complex landscape, ensuring these children remain as protected as possible within the constraints of their health status.
Post-Vaccine Lymphedema Changes: Understanding Symptoms and Management Tips
You may want to see also
Explore related products






![]()
Allergic Reactions: Severe allergies to vaccine components can make vaccination risky for certain children
Severe allergic reactions to vaccine components, though rare, pose a significant risk for certain children, necessitating careful consideration before vaccination. These reactions, known as anaphylaxis, can occur within minutes to hours after immunization and may involve symptoms like hives, swelling, difficulty breathing, or a sudden drop in blood pressure. The components most commonly implicated include gelatin, egg protein, antibiotics, and preservatives like neomycin or formaldehyde. For instance, the measles-mumps-rubella (MMR) vaccine contains trace amounts of gelatin, while influenza vaccines may contain residual egg protein. Children with known severe allergies to these substances require individualized risk assessment, often involving allergists and immunologists, to determine if vaccination is safe or if alternatives exist.
Analyzing the risk-benefit balance is crucial when a child has a history of severe allergies. For example, the Centers for Disease Control and Prevention (CDC) advises that children with egg allergies can safely receive most vaccines, including MMR and influenza, as studies show the risk of anaphylaxis is extremely low—approximately 1.31 cases per 1 million doses. However, precautions such as administering the vaccine in a healthcare setting equipped to manage anaphylaxis and observing the child for 30 minutes post-vaccination are recommended. In contrast, children with a severe gelatin allergy may need to avoid specific vaccines altogether, as alternatives are not always available. This underscores the importance of thorough medical history review and allergen-specific guidance.
Practical steps can help mitigate risks for children with potential vaccine allergies. Parents should inform healthcare providers about any known allergies, including reactions to foods, medications, or previous vaccines. For children with egg allergies, requesting vaccines grown in non-egg-based cultures, such as the cell culture-based flu vaccine (Flucelvax), can reduce risk. Additionally, premedication with antihistamines is generally not recommended as a preventive measure, as it does not prevent anaphylaxis and may mask early symptoms. Instead, ensuring immediate access to epinephrine auto-injectors (e.g., EpiPen) during and after vaccination is critical for prompt treatment if a reaction occurs.
Comparatively, while severe allergic reactions are a valid reason to defer or avoid certain vaccines, they represent a small fraction of vaccination contraindications. Other conditions, such as immunodeficiency or moderate-to-severe illness, may also temporarily or permanently preclude vaccination. However, the specificity of allergic reactions—tied directly to identifiable vaccine components—allows for more targeted management. For instance, children allergic to neomycin can often receive vaccines without this preservative, whereas those with gelatin allergies may have fewer options. This highlights the need for personalized approaches in vaccine administration, balancing protection against vaccine-preventable diseases with individual safety.
In conclusion, severe allergies to vaccine components require careful navigation but do not universally preclude vaccination. By understanding the specific allergens involved, leveraging available alternatives, and implementing safety protocols, healthcare providers can minimize risks for vulnerable children. Parents play a pivotal role in this process by providing detailed allergy histories and advocating for their child’s needs. While challenges exist, the goal remains clear: to protect as many children as possible through vaccination while safeguarding those for whom it poses an unacceptable risk.
Achieving Herd Immunity: Understanding the Vaccination Percentage Required
You may want to see also
Explore related products






![]()
Age Restrictions: Some vaccines are not approved for specific age groups, limiting availability for kids
Vaccines are meticulously tested and approved for specific age groups, ensuring safety and efficacy. For instance, the COVID-19 mRNA vaccines (Pfizer-BioNTech and Moderna) were initially authorized for adults before clinical trials confirmed their safety and effectiveness in younger populations. Pfizer’s vaccine received FDA approval for children aged 5–11 with a lower dosage (10 micrograms per shot, compared to 30 micrograms for adults), but only after months of additional research. This phased approach underscores why some vaccines remain unavailable to kids: regulatory bodies require robust data to ensure age-appropriate formulations.
Consider the measles, mumps, and rubella (MMR) vaccine, typically administered after 12 months of age. Infants are not vaccinated earlier because maternal antibodies, transferred during pregnancy, can interfere with the vaccine’s effectiveness. Similarly, the HPV vaccine is approved for ages 9 and up, but its benefits are maximized when administered before potential exposure to the virus. These age restrictions are not arbitrary; they are rooted in immunological science and clinical trial outcomes. Parents must adhere to these guidelines, even if it means delaying protection.
From a practical standpoint, age restrictions require caregivers to stay informed about vaccine schedules. For example, the influenza vaccine is approved for children as young as 6 months, but its formulation varies annually based on circulating strains. Parents should consult healthcare providers to confirm eligibility and timing. Additionally, some vaccines, like the meningococcal conjugate vaccine, have tiered recommendations: first dose at 11–12 years, with a booster at 16. Misalignment with these schedules can leave children vulnerable during critical developmental stages.
Critics might argue that age restrictions delay herd immunity, but prioritizing safety is non-negotiable. Take the rotavirus vaccine, withdrawn in 1999 due to rare intestinal complications in infants before being reformulated and reintroduced in 2006. This cautionary tale highlights the importance of age-specific testing. While waiting for approval, parents can protect children through indirect measures, such as ensuring household members are vaccinated and maintaining hygiene practices. Age restrictions are not barriers but safeguards, ensuring vaccines deliver their intended benefits without harm.
NC Vaccine Registration: A Step-by-Step Guide to Signing Up
You may want to see also
Explore related products






![]()
Temporary Illness: Acute illnesses may delay vaccination until the child fully recovers
Acute illnesses, such as high fever, respiratory infections, or gastrointestinal disorders, can temporarily halt a child’s vaccination schedule. These conditions trigger the immune system to focus on fighting the immediate threat, reducing its capacity to respond effectively to vaccines. For instance, a child with a fever above 101°F (38.3°C) is often advised to postpone vaccination until they recover. This delay ensures the vaccine’s efficacy isn’t compromised and avoids misattributing vaccine side effects to the illness. Pediatricians typically recommend waiting 2–3 days after fever resolution before proceeding with immunization.
Consider a scenario where a 2-year-old with a viral infection is due for their MMR (measles, mumps, rubella) vaccine. Administering the vaccine during active illness could lead to suboptimal antibody production, leaving the child partially unprotected. In such cases, healthcare providers follow the CDC’s guidelines, which emphasize that mild illnesses (e.g., a runny nose without fever) are not contraindications but moderate to severe illnesses warrant postponement. Parents should communicate all symptoms to their pediatrician, who may adjust the timeline based on the child’s overall health.
Delaying vaccination due to acute illness requires careful planning to avoid falling behind schedule. For example, a 6-month-old with rotavirus infection might miss their DTaP (diphtheria, tetanus, pertussis) dose. Once recovered, the pediatrician can administer the missed vaccine without restarting the series, ensuring continuity. Parents should keep a record of the illness duration and consult their healthcare provider to reschedule promptly. This proactive approach minimizes gaps in immunity while respecting the child’s temporary health limitations.
Critics might argue that delaying vaccination increases vulnerability to vaccine-preventable diseases, but this concern is outweighed by the need for optimal immune response. A study in *Pediatrics* found that vaccinating during acute illness reduced antibody titers by up to 30% in some cases. By waiting until recovery, parents ensure their child receives the full protective benefit of the vaccine. This balance between timing and efficacy underscores the importance of adhering to medical advice during temporary illnesses.
In practice, parents can take steps to minimize delays. Keeping children up to date on vaccines before cold and flu seasons reduces overlap with acute illnesses. For unavoidable situations, maintaining open communication with healthcare providers ensures a tailored approach. While temporary delays are common, they are not permanent barriers—most children resume their vaccination schedule seamlessly once healthy. This flexibility within immunization protocols prioritizes both safety and long-term protection.
Understanding the Smallpox Vaccine: Its Type and Historical Significance
You may want to see also
Explore related products





![]()
Parental Refusal: Personal beliefs or misinformation can lead parents to decline vaccines for their children
Parental refusal of vaccines for children often stems from deeply held personal beliefs or exposure to misinformation, creating a complex barrier to public health efforts. For instance, some parents adhere to philosophical or religious convictions that conflict with vaccination, viewing it as an infringement on personal freedom or a violation of natural living. Others fall prey to debunked myths, such as the false link between vaccines and autism, which persists despite overwhelming scientific evidence to the contrary. These decisions, while rooted in individual perspectives, have broader implications, as they can lower herd immunity and leave vulnerable populations at risk.
Consider the MMR (measles, mumps, rubella) vaccine, typically administered in two doses at 12–15 months and 4–6 years. Misinformation campaigns often target this vaccine, leading some parents to delay or outright refuse it. The result? Measles outbreaks have resurged in communities with low vaccination rates, endangering infants too young to be vaccinated and immunocompromised individuals. For example, in 2019, the U.S. saw its highest number of measles cases in decades, largely in unvaccinated populations. This highlights how personal beliefs, when amplified by misinformation, can undermine decades of progress in disease prevention.
To address parental refusal, healthcare providers must engage in empathetic, evidence-based communication. Start by acknowledging concerns without dismissing them. For instance, if a parent worries about vaccine ingredients like thimerosal, explain its safety profile and the fact that it’s no longer used in childhood vaccines (except some flu shots, which have trace amounts). Use analogies to simplify complex concepts: compare herd immunity to a firebreak protecting a forest. Provide resources from trusted sources, such as the CDC or WHO, and emphasize the historical success of vaccines in eradicating diseases like smallpox.
A comparative approach can also be effective. Contrast the risks of vaccine-preventable diseases with the rare side effects of vaccines. For example, measles can lead to pneumonia, encephalitis, or death in 1–3 per 1,000 cases, while severe allergic reactions to the MMR vaccine occur in about 1 per million doses. Framing the conversation around protecting not just their child but also the community can resonate with parents’ innate desire to keep others safe. Additionally, share stories of families affected by vaccine-preventable diseases to humanize the impact of refusal.
Ultimately, addressing parental refusal requires a multifaceted strategy. Public health campaigns must combat misinformation by promoting accurate, accessible information. Schools and community leaders can play a role by fostering dialogue and building trust. Policymakers should consider strengthening vaccine mandates while allowing medical exemptions, balancing public health needs with individual rights. By understanding the roots of refusal and responding with compassion and clarity, we can bridge the gap between personal beliefs and collective well-being, ensuring more children receive life-saving vaccines.
Nevada Vaccine Eligibility: Who Qualifies for COVID-19 Shots Now?
You may want to see also
Frequently asked questions
Some children cannot receive vaccines due to medical reasons, such as severe allergies to vaccine components (e.g., eggs or gelatin), a weakened immune system from conditions like HIV or cancer treatments, or a history of severe reactions to previous doses.
Yes, some vaccines are not approved for children under a specific age because their immune systems may not respond effectively or safely. For example, the HPV vaccine is typically not given before age 9, and the COVID-19 vaccine was initially restricted to older age groups before being approved for younger children.
It depends on the condition and vaccine. Many children with chronic illnesses can and should be vaccinated, as they are often at higher risk for complications from vaccine-preventable diseases. However, those with specific immune disorders or severe illnesses may need to avoid live vaccines (e.g., MMR or varicella) unless cleared by their doctor. Always consult a healthcare provider for personalized advice.