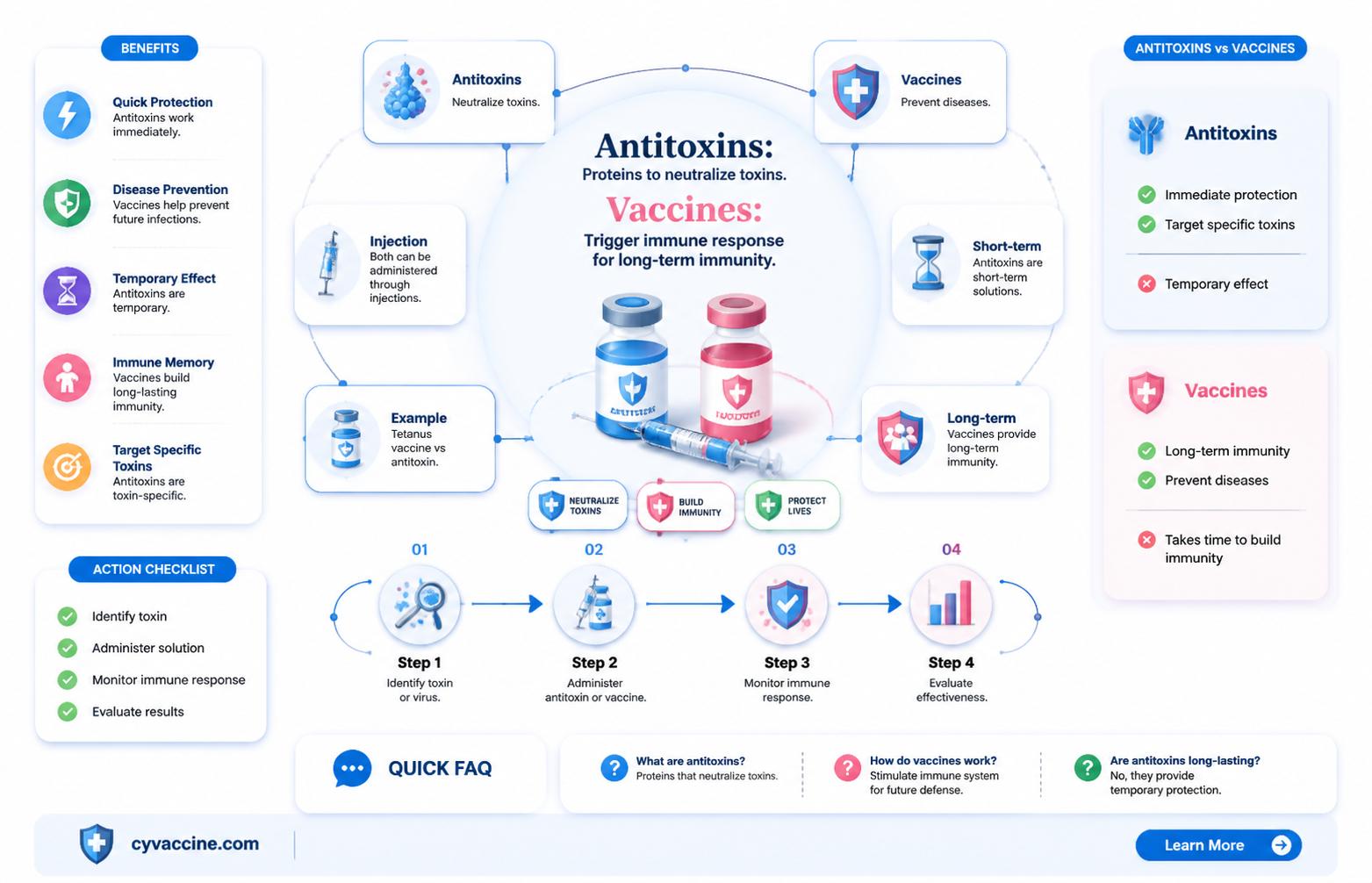
Antitoxins and vaccines are both crucial tools in the fight against infectious diseases, but they serve distinct purposes and function differently. Antitoxins are substances, typically antibodies, that neutralize toxins produced by bacteria or other pathogens, providing immediate but temporary protection or treatment after exposure. In contrast, vaccines stimulate the body’s immune system to produce its own antibodies and memory cells, offering long-term immunity by preventing or reducing the severity of infection. While both aim to combat disease, antitoxins act as a direct antidote to toxins, whereas vaccines focus on prevention by preparing the immune system for future encounters with pathogens. Understanding these differences is essential for appreciating their roles in public health and medical treatment.
| Characteristics | Values |
|---|---|
| Definition | Antitoxins are substances that neutralize toxins produced by bacteria or other pathogens. Vaccines are biological preparations that provide active, acquired immunity to particular diseases. |
| Mechanism of Action | Antitoxins directly neutralize toxins, often by binding to them. Vaccines stimulate the immune system to produce antibodies and memory cells for future protection. |
| Source | Antitoxins are typically derived from animals (e.g., horses) or produced synthetically. Vaccines are made from weakened/killed pathogens, their components, or genetic material. |
| Immunity Type | Antitoxins provide passive immunity, which is immediate but temporary. Vaccines provide active immunity, which is long-lasting and involves the body's own immune response. |
| Administration | Antitoxins are usually given after exposure to a toxin (post-exposure prophylaxis). Vaccines are administered before exposure to prevent disease. |
| Examples | Antitoxins: Diphtheria antitoxin, Botulinum antitoxin. Vaccines: MMR (Measles, Mumps, Rubella), COVID-19 vaccines. |
| Duration of Protection | Antitoxins offer protection for weeks to months. Vaccines provide protection for years or a lifetime, depending on the vaccine. |
| Side Effects | Antitoxins may cause allergic reactions (e.g., serum sickness). Vaccines may cause mild side effects like soreness, fever, or fatigue. |
| Purpose | Antitoxins treat or prevent toxin-mediated diseases. Vaccines prevent infectious diseases by inducing immunity. |
| Development | Antitoxins were developed in the late 19th century (e.g., diphtheria antitoxin). Vaccines have evolved over centuries, with modern advancements in mRNA and recombinant technologies. |
Explore related products






What You'll Learn
![]()
Antitoxin vs. Vaccine: Definition and Purpose
Antitoxins and vaccines, though both crucial in combating diseases, serve distinct purposes and operate through different mechanisms. Antitoxins are biological products derived from animals or humans that contain antibodies specifically designed to neutralize toxins produced by bacteria. For instance, diphtheria antitoxin is administered to counteract the potent exotoxin released by *Corynebacterium diphtheriae*, which can cause severe respiratory and cardiac complications. Vaccines, on the other hand, are prophylactic agents that stimulate the immune system to produce its own antibodies and memory cells, preparing the body to fight future infections. A classic example is the tetanus vaccine, which contains a toxoid (an inactivated form of the toxin) to induce immunity without causing disease.
Consider the scenario of a child exposed to tetanus through a deep wound. If the child has not been vaccinated, an immediate dose of tetanus antitoxin (3,000–6,000 units intramuscularly) is administered to neutralize the toxin already present. Simultaneously, a tetanus vaccine (0.5 mL intramuscularly) is given to ensure long-term immunity. This dual approach illustrates the complementary roles of antitoxins and vaccines: one provides immediate protection, while the other builds lasting defense. It’s critical to note that antitoxins offer passive immunity, meaning the borrowed antibodies do not confer permanent protection, whereas vaccines activate active immunity, training the body to respond autonomously.
From a practical standpoint, antitoxins are typically reserved for emergency situations or when immediate toxin neutralization is necessary. For example, botulism antitoxin is administered intravenously within hours of suspected exposure to prevent paralysis. Vaccines, however, are part of routine preventive care, often administered in multiple doses over years to ensure robust immunity. The DTaP vaccine (diphtheria, tetanus, and pertussis), for instance, is given to children at 2, 4, 6, and 15–18 months, followed by boosters at 4–6 years and 11–12 years. This schedule underscores the proactive nature of vaccines compared to the reactive use of antitoxins.
A key distinction lies in their side effects and risks. Antitoxins, being foreign proteins, can trigger serum sickness—a hypersensitivity reaction characterized by fever, rash, and joint pain—in up to 10% of recipients. To mitigate this, skin testing for sensitivity is sometimes performed before administration. Vaccines, while generally safe, may cause mild reactions like soreness at the injection site or low-grade fever. Rarely, severe allergic reactions (anaphylaxis) occur, typically within minutes of vaccination, emphasizing the importance of monitoring post-administration. Understanding these differences ensures appropriate use and patient education.
In summary, antitoxins and vaccines are not interchangeable but rather complementary tools in disease management. Antitoxins provide rapid, short-term relief by neutralizing toxins, while vaccines offer long-term protection by priming the immune system. For healthcare providers and patients alike, recognizing their unique roles ensures timely and effective intervention, whether in preventing tetanus after a rusty nail injury or treating diphtheria in an unvaccinated individual. Always consult guidelines for specific dosages and administration protocols, as these can vary based on age, weight, and clinical context.
Cancel Your NYS Vaccine Appointment: A Quick Step-by-Step Guide
You may want to see also
Explore related products






![]()
Mechanism of Action: How They Differ
Antitoxins and vaccines both serve as critical tools in the fight against infectious diseases, yet their mechanisms of action are fundamentally distinct. Antitoxins, typically derived from animal or human sources, are preformed antibodies that directly neutralize toxins produced by pathogens. For instance, diphtheria antitoxin is administered to bind and inactivate the potent exotoxin released by *Corynebacterium diphtheriae*, providing immediate protection. This passive immunity is short-lived, lasting only a few weeks, as the body does not produce its own antibodies in response to antitoxin treatment.
In contrast, vaccines operate by stimulating the immune system to generate its own protective response. They introduce a weakened or inactivated pathogen, or specific components of it, to trigger the production of memory cells and antibodies. For example, the tetanus vaccine contains a toxoid—a detoxified form of the tetanus toxin—that prompts the body to create antibodies capable of neutralizing the toxin if future exposure occurs. This active immunity is long-lasting, often providing protection for years or even decades, depending on the vaccine.
The timing and application of these interventions further highlight their differences. Antitoxins are primarily used as post-exposure prophylaxis or treatment, administered after an individual has been exposed to a toxin or is already symptomatic. For instance, a child with diphtheria might receive 20,000–100,000 units of antitoxin intravenously to counteract the toxin’s effects. Vaccines, however, are prophylactic, given to healthy individuals to prevent infection before exposure. The tetanus vaccine, for example, is typically administered in a series of doses starting in infancy, with booster shots recommended every 10 years for adults.
Practically, these differences dictate their use in specific scenarios. Antitoxins are reserved for urgent, life-threatening situations where immediate toxin neutralization is critical. Vaccines, on the other hand, are a cornerstone of public health, used to build herd immunity and prevent outbreaks. For travelers to regions with high tetanus risk, ensuring up-to-date vaccination is essential, while antitoxin treatment would only be considered if exposure is suspected or confirmed. Understanding these mechanisms ensures appropriate and effective use of each intervention.
When Should Kids Get the Varivax Vaccine? A Parent's Guide
You may want to see also
Explore related products






![]()
Immunity Duration: Short-Term vs. Long-Term
Antitoxins and vaccines both bolster immunity, but their mechanisms and duration of protection differ significantly. Antitoxins, such as those derived from horse serum for diphtheria, provide immediate, short-term immunity by neutralizing toxins already in the system. This passive immunity typically lasts weeks, not years, because the body does not produce its own antibodies. Vaccines, on the other hand, stimulate active immunity by training the immune system to recognize and combat pathogens. This process yields memory cells, offering protection that can span decades, as seen with measles or tetanus vaccines.
Consider the practical implications for travelers. A person visiting a region with high diphtheria risk might receive an antitoxin injection for immediate protection, but this safeguard wanes within 2–4 weeks. In contrast, a tetanus vaccine administered months or years prior provides enduring immunity, eliminating the need for urgent intervention. Dosage matters here: antitoxins often require higher, immediate doses (e.g., 10,000–50,000 units for diphtheria antitoxin), while vaccines use microgram quantities (e.g., 0.5 mL of the Tdap vaccine) to trigger long-term immunity.
For parents, understanding these differences is critical. A child exposed to pertussis (whooping cough) might receive an antitoxin for rapid symptom mitigation, but this does not prevent future infections. Vaccination with DTaP, however, builds lasting immunity, reducing hospitalization risk by 80% in the first year post-vaccination. Age-specific protocols further illustrate this divide: infants under 6 weeks cannot receive certain vaccines, making antitoxins their only short-term defense against diseases like botulism.
The takeaway is clear: antitoxins are not vaccines. They serve as emergency stopgaps, not long-term solutions. Vaccines, through their ability to engender memory responses, remain the cornerstone of preventive medicine. For optimal protection, combine short-term antitoxin use in acute exposures with consistent, age-appropriate vaccination schedules. Always consult healthcare providers to tailor strategies to individual needs, ensuring both immediate safety and enduring health.
US Global Vaccine Aid: Sharing Doses to Combat COVID-19 Worldwide
You may want to see also
Explore related products






![]()
Administration: Passive vs. Active Immunization
Antitoxins and vaccines both aim to protect against disease, but their mechanisms and administration methods differ significantly. While vaccines stimulate the body’s immune system to produce its own antibodies, antitoxins provide pre-formed antibodies directly. This distinction is crucial when considering passive vs. active immunization, two strategies with unique applications, benefits, and limitations.
Passive immunization involves the direct administration of pre-formed antibodies, typically through antitoxins or immunoglobulins. This method provides immediate but temporary protection, as the antibodies do not persist long-term. For example, tetanus antitoxin is given in cases of suspected tetanus exposure to neutralize the toxin rapidly. Dosage varies by severity but often ranges from 500 to 3,000 units for adults. Similarly, rabies immunoglobulin is administered alongside the rabies vaccine for post-exposure prophylaxis, delivering instant antibodies to combat the virus. Passive immunization is particularly useful in emergencies or for immunocompromised individuals who cannot mount an immune response. However, it carries risks such as allergic reactions and does not confer lasting immunity.
In contrast, active immunization uses vaccines to stimulate the body’s immune system to produce its own antibodies. This process takes time—typically weeks—but results in long-term or lifelong immunity. For instance, the diphtheria-tetanus-pertussis (DTaP) vaccine for children under 7 years old or the Tdap booster for adolescents and adults not only prevents tetanus but also induces memory cells for future protection. Active immunization is the cornerstone of public health, as seen in the eradication of smallpox and the control of polio. However, it is less effective in urgent situations where immediate protection is needed.
The choice between passive and active immunization depends on the context. For travelers exposed to rabies in remote areas, immediate passive immunization with rabies immunoglobulin is critical, followed by active immunization with the vaccine series. In contrast, routine childhood vaccinations like the MMR vaccine (measles, mumps, rubella) rely solely on active immunization, as the risk of exposure is ongoing, and long-term protection is essential. Practical tips include ensuring timely vaccine schedules, storing antitoxins properly (often refrigerated), and monitoring for adverse reactions post-administration.
In summary, while antitoxins and vaccines both combat disease, their administration reflects the fundamental difference between passive and active immunization. Passive immunization offers rapid, short-term protection through direct antibody delivery, ideal for emergencies. Active immunization, via vaccines, builds lasting immunity but requires time. Understanding these distinctions ensures appropriate use, maximizing protection while minimizing risks.
Trump's Role in COVID-19 Vaccine Development
You may want to see also
Explore related products





![]()
Historical Use: Antitoxins in Disease Prevention
Antitoxins, derived from the antibodies of immunized animals, played a pivotal role in disease prevention before the widespread use of vaccines. In the late 19th and early 20th centuries, they were the primary defense against bacterial toxins, particularly in diseases like diphtheria and tetanus. For instance, in 1894, Emil von Behring and Shibasaburo Kitasato developed the first antitoxin serum for diphtheria, which significantly reduced mortality rates among children. Administered as an injection, a typical dose ranged from 10,000 to 50,000 units, depending on the severity of the infection and the patient’s age. This breakthrough marked the beginning of passive immunization, a strategy that provided immediate, though temporary, protection against deadly toxins.
The production of antitoxins involved immunizing horses or sheep with controlled doses of bacterial toxins, allowing their immune systems to generate antibodies. These antibodies were then extracted from the animals’ blood, purified, and administered to humans. While effective, this method had limitations. Antitoxins offered only short-term immunity, lasting weeks to months, and repeated doses could lead to serum sickness, an allergic reaction caused by the foreign proteins. Despite these drawbacks, antitoxins were a lifeline during epidemics, particularly in resource-limited settings where vaccines were not yet available or affordable.
One of the most notable historical uses of antitoxins was during the diphtheria epidemic in the early 20th century. Before the introduction of the diphtheria vaccine in the 1920s, antitoxin serum was the only reliable treatment. Public health campaigns emphasized early diagnosis and prompt administration of antitoxins, often within hours of symptom onset. Parents were educated to recognize the disease’s hallmark signs—a thick gray membrane in the throat—and seek immediate medical attention. This proactive approach saved countless lives, particularly among children under five, who were most vulnerable to the disease.
Comparatively, antitoxins and vaccines serve distinct purposes. While antitoxins provide immediate protection by neutralizing existing toxins in the body, vaccines stimulate the immune system to produce its own antibodies, offering long-term immunity. Antitoxins were often used reactively, as a treatment for infected individuals, whereas vaccines are administered proactively to prevent infection altogether. For example, the tetanus antitoxin was used to treat exposed wounds, while the tetanus vaccine is given as part of routine immunizations to prevent the disease. This distinction highlights the complementary roles of antitoxins and vaccines in public health.
In conclusion, the historical use of antitoxins in disease prevention underscores their significance as a precursor to modern vaccines. They provided a critical bridge during a time when infectious diseases were rampant and medical solutions scarce. While their use has declined with the advent of vaccines, antitoxins remain relevant in specific contexts, such as treating botulism or managing severe infections in unvaccinated individuals. Understanding their role offers valuable insights into the evolution of immunology and the ongoing quest to protect human health.
Choosing the Optimal 4th Booster Vaccine: Expert Recommendations and Insights
You may want to see also
Frequently asked questions
No, antitoxins and vaccines are not the same. Antitoxins are substances that neutralize toxins produced by bacteria, while vaccines stimulate the immune system to produce its own antibodies against specific pathogens.
Antitoxins work by directly neutralizing toxins already present in the body, providing immediate but temporary protection. Vaccines, on the other hand, train the immune system to recognize and fight pathogens, offering long-term immunity.
Antitoxins do not prevent diseases; they treat the effects of toxins after infection. Vaccines, however, prevent diseases by preparing the immune system to combat pathogens before exposure.
Antitoxins are not an alternative to vaccines. They are used in specific cases to treat toxin-related illnesses, whereas vaccines are used for disease prevention.
No, antitoxins do not provide long-term immunity. They offer immediate but temporary relief from toxin effects, while vaccines confer lasting immunity by stimulating the immune system.