The development and availability of a vaccine typically follow a rigorous process that includes research, pre-clinical testing, clinical trials, regulatory approval, and mass production. While advancements in technology and global collaboration have accelerated timelines, creating a safe and effective vaccine usually takes several years. However, in urgent situations like the COVID-19 pandemic, unprecedented efforts and resources have been mobilized, allowing vaccines to be developed and approved in as little as 10 to 12 months. Factors such as funding, international cooperation, and existing scientific knowledge play critical roles in determining how soon a vaccine can be ready. Despite these advancements, ensuring safety, efficacy, and equitable distribution remain paramount challenges in the race to deliver vaccines to the public.
| Characteristics | Values |
|---|---|
| Typical Vaccine Development Time | 5–10 years |
| Accelerated Timeline (COVID-19) | 12–18 months (unprecedented speed due to global collaboration and funding) |
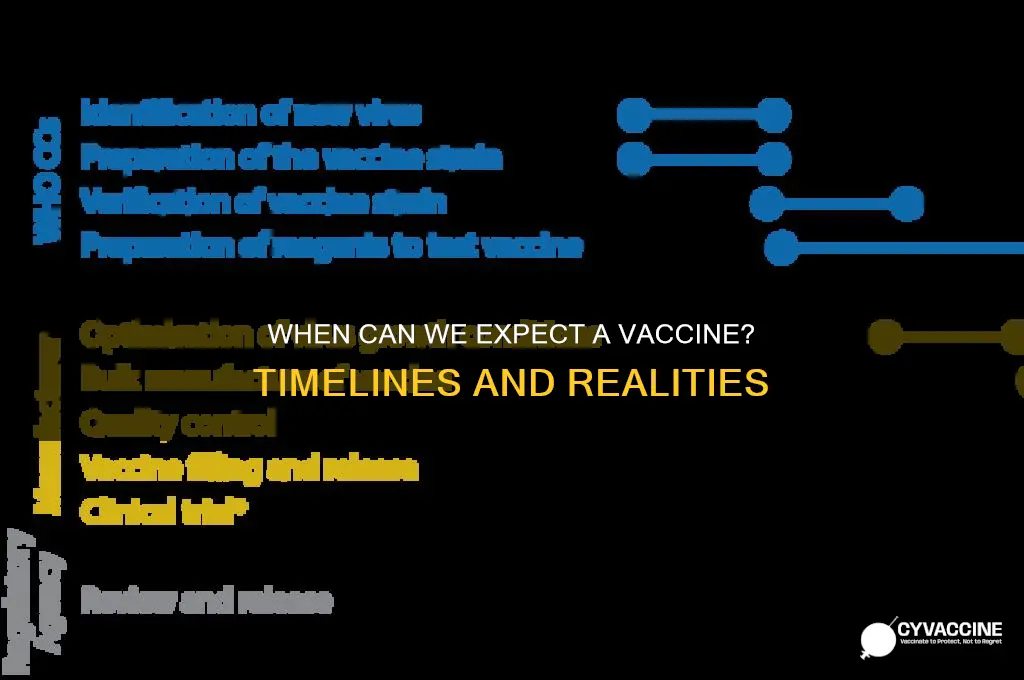
| Key Stages in Development | Preclinical testing, Phase 1–3 clinical trials, regulatory approval |
| Emergency Use Authorization (EUA) | Allows early distribution during public health emergencies |
| Manufacturing Scale-Up | Begins during clinical trials to reduce time post-approval |
| Global Collaboration | Over 200 vaccine candidates in development (as of 2023) |
| Technological Advances | mRNA and viral vector platforms enabled faster development |
| Funding and Resources | Billions invested by governments and private sectors |
| Regulatory Flexibility | Fast-tracked reviews without compromising safety standards |
| Distribution Challenges | Cold chain requirements, equitable global access |
| Public Hesitancy | Vaccine acceptance varies by region, impacting rollout speed |
| Booster Requirements | Ongoing research to determine need for additional doses |
| Variant Adaptation | Rapid updates to vaccines to target new variants (e.g., Omicron) |
| Long-Term Monitoring | Post-approval surveillance for safety and efficacy |
Explore related products






What You'll Learn
- Preclinical Testing Timeline: Animal studies and safety checks before human trials begin
- Clinical Trial Phases: Three phases to test safety, efficacy, and dosage in humans
- Manufacturing Scale-Up: Preparing facilities and resources for mass production of the vaccine
- Regulatory Approval Process: Expedited reviews by health agencies to ensure safety and efficacy
- Distribution Challenges: Logistics of transporting and administering vaccines globally
![]()
Preclinical Testing Timeline: Animal studies and safety checks before human trials begin
Before a vaccine candidate advances to human trials, it undergoes rigorous preclinical testing to ensure safety and efficacy. This phase, often lasting 1–2 years, involves animal studies and safety checks designed to predict how the vaccine will behave in humans. Typically, researchers start with small animals like mice or rats to assess immune responses and toxicity at varying dosages, often ranging from 0.1 to 10 micrograms per kilogram of body weight. These initial studies help determine the optimal dose and identify potential side effects, such as inflammation or allergic reactions, before moving to larger animals like monkeys or ferrets, which better mimic human physiology.
Animal studies are not just about observing immune responses; they also involve challenge trials, where vaccinated animals are deliberately exposed to the pathogen to test the vaccine’s protective efficacy. For example, in COVID-19 vaccine development, researchers infected vaccinated monkeys with the SARS-CoV-2 virus and monitored viral load in nasal swabs and lung tissue. If the vaccine reduces viral replication by 90% or more, it’s considered a promising candidate. However, these studies require careful design to ensure ethical treatment of animals and accurate translation to human outcomes.
Safety checks in preclinical testing go beyond efficacy. Researchers evaluate the vaccine’s stability, formulation, and potential for adverse effects like antibody-dependent enhancement (ADE), where the vaccine inadvertently worsens infection. For instance, dengue vaccine candidates have historically faced ADE challenges, underscoring the need for thorough investigation. Regulatory agencies like the FDA require detailed reports on manufacturing processes, including the purity of vaccine components and the consistency of production batches, to ensure quality control.
A critical but often overlooked aspect of preclinical testing is the choice of animal models. Not all species respond to vaccines the same way; for example, mice may not accurately reflect human immune responses to certain viruses. Scientists must select models that best represent human disease progression and immune mechanisms. This step can add months to the timeline but is essential for avoiding costly failures in later phases.
In conclusion, preclinical testing is a meticulous, multi-layered process that balances speed with caution. While advancements like high-throughput screening and computational modeling have accelerated this phase, it remains a bottleneck in vaccine development. Skipping or rushing these steps risks public safety and undermines trust in vaccines. For those tracking vaccine timelines, understanding this phase highlights why “soon” is relative—and why patience is as crucial as urgency.
Canadian Truckers' Vaccination Rates: Insights and Implications
You may want to see also
Explore related products


$126.09 $166.95

$11.93 $21.99



![]()
Clinical Trial Phases: Three phases to test safety, efficacy, and dosage in humans
Vaccine development is a meticulous process, and clinical trials are its backbone. These trials are divided into three distinct phases, each with a specific goal: ensuring the vaccine is safe, effective, and administered in the right dosage.
Phase 1: Safety First
This initial phase involves a small group of healthy volunteers, typically 20–100 individuals, to assess the vaccine’s safety profile. Participants are closely monitored for adverse reactions, such as fever, fatigue, or allergic responses. Dosage levels are carefully calibrated, often starting with micrograms (e.g., 10 µg) and escalating to determine the maximum tolerated dose without severe side effects. For example, in COVID-19 vaccine trials, early-phase participants received doses ranging from 25 µg to 250 µg to identify the optimal amount. Practical tip: Volunteers should maintain a symptom diary to report even minor changes, ensuring no detail is overlooked.
Phase 2: Efficacy and Immunogenicity
With safety established, Phase 2 expands to several hundred participants, often including diverse age groups (e.g., 18–55 years and 55+). This phase evaluates the vaccine’s ability to induce an immune response and its efficacy in preventing the target disease. Placebos are commonly used to compare outcomes. For instance, in a flu vaccine trial, participants might receive either the vaccine or a saline injection, with blood tests measuring antibody levels over weeks. Key takeaway: This phase helps refine dosage—a 50 µg dose might prove more effective than 25 µg—and identifies potential side effects in broader populations.
Phase 3: Large-Scale Validation
The final phase is the most extensive, involving thousands to tens of thousands of participants across multiple regions. Here, the vaccine’s efficacy is rigorously tested in real-world conditions. For example, a COVID-19 vaccine trial might enroll 30,000 participants, half receiving the vaccine and half a placebo, to determine its ability to prevent infection or severe illness. Dosage consistency is critical; a standardized 30 µg dose ensures results are comparable across the group. Caution: Rare side effects may only surface in this phase due to the larger sample size, emphasizing the need for continued monitoring.
Practical Considerations and Timeline
Each phase typically lasts 1–4 years, though accelerated timelines (e.g., 6–12 months for COVID-19 vaccines) are possible during public health emergencies. Participants should be aware of exclusion criteria, such as pre-existing conditions or age limits, which vary by trial. For instance, Phase 1 often restricts participants to ages 18–55, while Phase 3 may include older adults and those with comorbidities. Final thought: While these phases are sequential, overlapping trials and adaptive designs can expedite the process, bringing vaccines to market sooner without compromising safety or efficacy.
Understanding Adult Pneumonia Vaccines: Ingredients, Benefits, and Protection
You may want to see also
Explore related products

$26.99 $26.99


$28.99 $32.99



![]()
Manufacturing Scale-Up: Preparing facilities and resources for mass production of the vaccine
The race to produce a vaccine often hinges on manufacturing scale-up, a complex process that transforms lab-scale production into global distribution. While clinical trials determine safety and efficacy, parallel efforts must ensure facilities and resources are ready to meet unprecedented demand. This requires meticulous planning, significant investment, and innovative solutions to overcome logistical challenges.
Manufacturing scale-up begins with facility preparation. Existing vaccine production plants may need retooling to accommodate new processes and equipment. For instance, mRNA vaccines like Pfizer-BioNTech’s require specialized lipid nanoparticle production capabilities, demanding cleanrooms and precise temperature control (typically -70°C for storage). Building new facilities from scratch can take 2–5 years, but retrofitting existing ones can shorten timelines to 6–12 months. Governments and manufacturers often collaborate to expedite this process, as seen during the COVID-19 pandemic, where Operation Warp Speed in the U.S. provided funding and regulatory fast-tracking.
Resource allocation is equally critical. Raw materials, such as cell culture media, adjuvants, and glass vials, must be secured in vast quantities. A single dose of a vaccine may require just 0.3 mL of liquid, but producing billions of doses necessitates a stable supply chain. For example, the COVID-19 vaccine rollout faced shortages of lipid nanoparticles and specialized syringes. Manufacturers must also train personnel to operate new machinery and adhere to stringent quality control standards, such as Good Manufacturing Practices (GMP). Cross-contamination risks are high, so facilities often dedicate separate production lines for different vaccines.
A key challenge is balancing speed with safety. Scaling up too quickly can lead to production errors, as seen in early 2021 when a Baltimore plant accidentally mixed ingredients for Johnson & Johnson and AstraZeneca vaccines, ruining millions of doses. To mitigate risks, manufacturers conduct trial runs and implement real-time monitoring systems. Additionally, regulatory agencies like the FDA allow emergency use authorizations (EUAs) to accelerate approval while maintaining safety thresholds.
Finally, distribution logistics must align with manufacturing capabilities. Vaccines often require cold chain storage, with some needing ultra-cold temperatures. For instance, Pfizer’s vaccine must be stored at -70°C, while Moderna’s can withstand -20°C. This necessitates specialized transport and storage infrastructure, particularly in low-resource settings. Governments and NGOs collaborate to establish distribution networks, ensuring vaccines reach priority groups, such as healthcare workers and the elderly, first.
In summary, manufacturing scale-up is a multifaceted endeavor requiring facility upgrades, resource management, quality control, and logistical coordination. While it presents significant challenges, lessons from recent pandemics demonstrate that with strategic planning and collaboration, vaccine production can be scaled up rapidly without compromising safety. The goal is not just speed but sustainable, equitable distribution to protect global health.
North Dakota's Vaccination Progress: How Many Residents Are Fully Vaccinated?
You may want to see also
Explore related products






![]()
Regulatory Approval Process: Expedited reviews by health agencies to ensure safety and efficacy
The race to develop a vaccine often hinges on the regulatory approval process, a critical phase that balances speed with safety. Health agencies like the FDA, EMA, and WHO have implemented expedited review pathways to accelerate access to vaccines during public health emergencies. These pathways, such as the FDA’s Emergency Use Authorization (EUA) and the EMA’s Conditional Marketing Authorization, allow vaccines to be approved in months rather than years. However, expedited does not mean compromised; rigorous standards for safety and efficacy remain non-negotiable. For instance, Phase 3 clinical trials still require thousands of participants to demonstrate a vaccine’s effectiveness, typically achieving at least 50% efficacy to meet regulatory thresholds.
Consider the steps involved in an expedited review. First, manufacturers submit rolling data from clinical trials, allowing regulators to assess information as it becomes available rather than waiting for a complete package. Second, priority reviews shorten evaluation timelines from the standard 10–12 months to as little as 6 weeks. Third, post-approval monitoring, including Phase 4 studies and pharmacovigilance programs, ensures ongoing safety. For example, the Pfizer-BioNTech COVID-19 vaccine received EUA after demonstrating 95% efficacy in a 44,000-participant trial, with regulators reviewing data in real-time. This approach reduces administrative delays without bypassing critical safety checks.
A common misconception is that expedited approvals sacrifice thoroughness. In reality, regulators focus on the same endpoints—safety, immunogenicity, and efficacy—but streamline bureaucratic processes. For instance, the FDA’s EUA requires evidence that a vaccine’s benefits outweigh risks in a specific population, often starting with high-risk groups like healthcare workers or the elderly. Dosage regimens, such as a two-dose series administered 3–4 weeks apart, are carefully evaluated to maximize protection while minimizing side effects. This targeted approach ensures that even under accelerated timelines, vaccines meet established scientific criteria.
Expedited reviews also rely on international collaboration. Regulatory agencies share data and harmonize standards through coalitions like the International Coalition of Medicines Regulatory Authorities (ICMRA). This cooperation prevents duplication of efforts and accelerates global access. For example, the WHO’s Emergency Use Listing (EUL) allows vaccines approved by stringent regulatory authorities to be distributed in low-resource countries. Such partnerships highlight how expedited processes can be both efficient and equitable, ensuring that safety and efficacy are upheld across borders.
Practical tips for stakeholders navigating expedited approvals include early engagement with regulators to clarify expectations and leveraging existing platforms, such as mRNA technology, which can shorten development timelines. Manufacturers should also prepare for post-approval scrutiny by establishing robust surveillance systems. For the public, understanding that expedited does not mean rushed is key. Vaccines like Moderna’s COVID-19 shot, which progressed from lab to approval in under a year, exemplify how innovation and regulatory flexibility can coexist. Ultimately, expedited reviews are a testament to the adaptability of health agencies in crises, ensuring that vaccines are ready when the world needs them most.
Divine Perspective: Understanding God's View on Vaccines and Health
You may want to see also
Explore related products






![]()
Distribution Challenges: Logistics of transporting and administering vaccines globally
The COVID-19 pandemic underscored a critical truth: developing a vaccine is only half the battle. The Pfizer-BioNTech vaccine, for instance, requires ultra-cold storage at -70°C, a logistical nightmare for many countries lacking specialized infrastructure. This example highlights the first major hurdle in global vaccine distribution: temperature-sensitive logistics. Many vaccines, especially mRNA-based ones, degrade rapidly without precise temperature control, necessitating a "cold chain" from manufacturing plants to remote clinics. This isn’t just about refrigerators; it involves insulated packaging, real-time temperature monitoring, and backup power systems to prevent spoilage during transit.
Consider the scale: distributing billions of doses globally requires coordination across continents, each with unique challenges. In rural Africa, where only 28% of healthcare facilities have reliable electricity, maintaining a cold chain becomes nearly impossible. Contrast this with urban Europe, where advanced logistics networks can handle such demands but face bottlenecks in last-mile delivery. Prioritization becomes another critical issue. Who gets the vaccine first? High-income countries often secure doses through advance purchase agreements, leaving low-income nations reliant on initiatives like COVAX, which struggle to compete. This inequity delays global herd immunity and prolongs the pandemic.
Administering vaccines introduces another layer of complexity. The Pfizer vaccine requires two doses, 21 days apart, while AstraZeneca’s allows a 4–12-week interval. Such variations demand precise scheduling and patient tracking systems, particularly in regions with limited digital infrastructure. Training healthcare workers is equally vital. Administering mRNA vaccines, for example, involves drawing specific dose volumes (0.3 mL for Pfizer) and managing potential side effects like anaphylaxis. In areas with shortages of trained personnel, this becomes a significant barrier.
Finally, public trust and accessibility cannot be overlooked. Vaccine hesitancy, fueled by misinformation, reduces uptake even when doses are available. In Brazil, for instance, a 2021 survey found that 20% of the population was hesitant to receive a COVID-19 vaccine. Community engagement and localized communication strategies are essential to address these concerns. Mobile clinics, for example, have proven effective in reaching underserved populations, but they require funding and coordination. Without addressing these social and logistical factors, even the fastest-developed vaccine will fall short of its potential impact.
In summary, the speed of vaccine development is just one piece of the puzzle. Overcoming distribution challenges requires a multifaceted approach: investing in cold chain infrastructure, equitable allocation mechanisms, robust healthcare systems, and community-driven strategies. Only then can we ensure that vaccines reach those who need them most, regardless of geography or income.
Revolutionary Inventions Paving the Way for Animal Vaccines
You may want to see also
Frequently asked questions
Traditionally, vaccine development can take 10–15 years, including research, clinical trials, and regulatory approval. However, expedited processes, like those used for COVID-19 vaccines, can reduce this timeline to 1–2 years with significant resources and global collaboration.
COVID-19 vaccines were developed rapidly due to unprecedented global funding, pre-existing research on similar coronaviruses, streamlined clinical trials, and regulatory fast-tracking. Additionally, manufacturers began production before approval, reducing delays.
Yes, advancements in technology, such as mRNA platforms and improved data sharing, could further shorten timelines. However, speed depends on factors like the disease's complexity, funding, and regulatory requirements.
With lessons from COVID-19, a vaccine for a new pandemic could be ready within 6–12 months if the pathogen is well-understood, resources are available, and regulatory processes are expedited. Early detection and global coordination are critical.