Spacing out vaccines is a critical aspect of immunization schedules, designed to maximize their effectiveness while minimizing potential risks. Health organizations, such as the World Health Organization (WHO) and the Centers for Disease Control and Prevention (CDC), provide evidence-based guidelines to ensure vaccines are administered at optimal intervals. These schedules consider factors like the immune system’s response, the disease’s prevalence, and the vaccine’s formulation. Proper spacing allows the body to build sufficient immunity without overloading the immune system, ensuring protection against preventable diseases. Deviating from recommended schedules can leave individuals vulnerable to infections, underscoring the importance of adhering to established protocols.
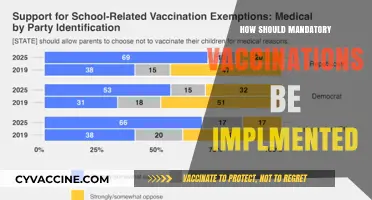
| Characteristics | Values |
|---|---|
| Minimum Interval Between Doses | Varies by vaccine type; e.g., mRNA COVID-19 vaccines (Pfizer, Moderna) typically require 3-4 weeks between doses, while adenovirus vector vaccines (J&J) are single-dose. |
| Immune Response Optimization | Spacing doses allows the immune system to build a stronger response; e.g., longer intervals (8-12 weeks) for some vaccines like COVID-19 may enhance efficacy. |
| Age Considerations | Infants and young children often follow specific schedules (e.g., 2, 4, 6 months) to align with immune system development. |
| Vaccine Type | Live attenuated vaccines (e.g., MMR) may require longer intervals (4-6 weeks) to avoid interference, while inactivated vaccines (e.g., flu) can be given closer together. |
| Catch-Up Vaccination | If doses are delayed, catch-up schedules may allow for shorter intervals to complete the series promptly. |
| Booster Doses | Boosters are typically given 6 months to 1 year after the primary series, depending on the vaccine and immunity wane. |
| Simultaneous Administration | Some vaccines can be given on the same day (e.g., flu and COVID-19), while others require spacing to monitor side effects. |
| Travel or Outbreak Situations | Accelerated schedules may be used in urgent cases, but efficacy and safety must be considered. |
| Individual Health Status | Immunocompromised individuals may require adjusted intervals or additional doses. |
| Global Recommendations | WHO and CDC guidelines provide standardized spacing recommendations, but local health authorities may adapt based on regional needs. |
Explore related products


$18.59 $19.95




What You'll Learn
- Optimal Vaccine Interval Timing: Recommended gaps between doses for maximum immune response and safety
- Age-Specific Spacing Guidelines: Tailored vaccine schedules for infants, adults, and elderly populations
- Simultaneous vs. Sequential Vaccines: Benefits and risks of administering multiple vaccines at once or separately
- Immune System Considerations: How health conditions or immunocompromised states affect vaccine spacing
- Catch-Up Vaccination Strategies: Effective spacing for missed doses to ensure full immunization coverage
![]()
Optimal Vaccine Interval Timing: Recommended gaps between doses for maximum immune response and safety
The timing between vaccine doses is a critical factor in ensuring both the safety and efficacy of immunization. For instance, the COVID-19 mRNA vaccines (Pfizer-BioNTech and Moderna) are administered with a recommended interval of 3 to 4 weeks between the first and second doses for individuals aged 12 and older. This interval is designed to maximize the immune response while minimizing the risk of side effects. Shorter intervals may lead to suboptimal immunity, as the immune system requires time to mount a robust response to the initial dose. Conversely, longer intervals can delay the achievement of full protection, leaving individuals vulnerable for extended periods.
From an analytical perspective, the optimal vaccine interval varies depending on the vaccine type, the pathogen it targets, and the recipient’s age and immune status. For example, the HPV vaccine (Gardasil 9) is typically given in two doses, 6 to 12 months apart for individuals aged 15 to 45, but three doses over 6 months for younger adolescents aged 9 to 14. This difference highlights how age-specific immune responses influence dosing schedules. Similarly, the shingles vaccine (Shingrix) requires two doses, spaced 2 to 6 months apart, to ensure adequate protection in older adults whose immune systems may be less responsive. Understanding these variations is essential for healthcare providers to tailor vaccination plans effectively.
Instructively, patients should adhere strictly to the recommended intervals provided by their healthcare provider or national health guidelines. Missing a dose or delaying it beyond the advised timeframe may necessitate restarting the vaccination series, particularly for vaccines like hepatitis B, where precise timing is crucial for seroconversion. Practical tips include setting reminders for follow-up doses, keeping a vaccination record, and consulting a healthcare professional if a dose is missed. For travelers requiring accelerated schedules, such as for yellow fever or typhoid vaccines, medical advice should be sought to balance protection with safety.
Persuasively, the science behind vaccine intervals underscores the importance of patience in achieving immunity. While it may be tempting to expedite the process, especially during disease outbreaks, adhering to recommended gaps ensures the body can develop memory cells and antibodies effectively. For example, the influenza vaccine is reformulated annually, and receiving it too early in the season may reduce its efficacy by the peak of flu activity. Conversely, delaying doses unnecessarily increases susceptibility to preventable diseases. Public health campaigns should emphasize that optimal timing is a cornerstone of vaccine success, not merely a bureaucratic guideline.
Comparatively, the concept of vaccine intervals can be likened to a recipe where precise measurements and timing determine the outcome. Just as baking requires specific intervals for ingredients to interact, vaccines need calculated gaps for the immune system to respond optimally. For instance, the measles-mumps-rubella (MMR) vaccine relies on a 4-week minimum interval between doses to prevent interference between immune responses. In contrast, the tetanus booster can be administered as soon as 2 weeks after a dirty wound exposure, demonstrating how urgency and safety dictate timing. This analogy highlights the balance between standardization and flexibility in vaccination protocols.
In conclusion, optimal vaccine interval timing is a nuanced aspect of immunization that balances immune response, safety, and practical considerations. By understanding the rationale behind recommended gaps—whether 3 weeks for COVID-19 vaccines or 6 months for HPV—individuals and healthcare providers can ensure maximum protection. Adherence to these schedules, coupled with awareness of age-specific and vaccine-specific variations, is vital for public health. As vaccination remains a cornerstone of disease prevention, respecting the science of timing is as crucial as the vaccines themselves.
Vaccines: Unraveling the Truth About Their Benefits and Safety
You may want to see also
Explore related products






![]()
Age-Specific Spacing Guidelines: Tailored vaccine schedules for infants, adults, and elderly populations
Infants require a carefully orchestrated vaccine schedule to build immunity without overwhelming their developing immune systems. The Centers for Disease Control and Prevention (CDC) recommends a series of vaccinations starting at birth, with the first dose of the hepatitis B vaccine administered within 24 hours of life. Subsequent vaccines, such as DTaP (diphtheria, tetanus, pertussis), Hib (Haemophilus influenzae type b), and PCV13 (pneumococcal conjugate vaccine), are typically given in a series of doses spaced 4 to 8 weeks apart. This interval allows the immune system to respond adequately to each vaccine while minimizing the risk of adverse reactions. For example, the first dose of the rotavirus vaccine is given at 2 months, followed by a second dose at 4 months, and a third dose at 6 months if necessary, depending on the brand. Parents should adhere strictly to this schedule, as deviations can compromise the effectiveness of the vaccines.
Adults, particularly those with no prior vaccination history or incomplete records, face a different set of spacing guidelines. Catch-up schedules often condense multiple vaccines into a shorter timeframe while ensuring safety and efficacy. For instance, the HPV (human papillomavirus) vaccine series for adults aged 27 to 45 is administered in three doses: the first dose, followed by the second dose 1–2 months later, and the third dose 6 months after the first. Similarly, the Tdap (tetanus, diphtheria, pertussis) booster is recommended every 10 years, but if an adult requires protection sooner, it can be given as early as 5 years after the last dose. Adults should also consider seasonal vaccines like the flu shot annually, spaced at least 2 weeks apart from other live vaccines to avoid interference.
Elderly populations, often with age-related immune decline, benefit from tailored vaccine spacing that maximizes protection. The shingles vaccine, for example, is recommended for adults over 50, with the two-dose Shingrix series given 2 to 6 months apart. Pneumococcal vaccines, such as PCV15 and PPSV23, are spaced 1 year apart for optimal immunity in this age group. Additionally, the high-dose flu vaccine is specifically formulated for adults 65 and older, administered annually but with a focus on timing—ideally in early fall to ensure peak immunity during flu season. Caregivers and healthcare providers should prioritize minimizing the number of clinic visits by combining vaccines when possible, such as administering the flu and pneumococcal vaccines during the same appointment.
Practical tips for all age groups include maintaining a detailed vaccination record, setting reminders for follow-up doses, and consulting healthcare providers to address specific health conditions or concerns. For infants, spacing vaccines correctly is crucial to avoid overloading their immune system, while adults and the elderly should focus on timely boosters and age-specific formulations. By adhering to these age-specific spacing guidelines, individuals can ensure they receive the maximum benefit from their vaccines, tailored to their unique physiological needs and immune responses.
Fully Vaccinated and Traveling: Do Quarantine Rules Still Apply?
You may want to see also
Explore related products






![]()
Simultaneous vs. Sequential Vaccines: Benefits and risks of administering multiple vaccines at once or separately
The decision to administer vaccines simultaneously or sequentially hinges on balancing immune response efficacy, logistical convenience, and potential side effects. Simultaneous administration, where multiple vaccines are given during the same visit, is a cornerstone of childhood immunization schedules. For instance, the CDC recommends that infants receive the DTaP (diphtheria, tetanus, pertussis), IPV (inactivated poliovirus), Hib (Haemophilus influenzae type b), and PCV13 (pneumococcal conjugate) vaccines at 2, 4, and 6 months of age, often in combination with others like rotavirus vaccine. This approach ensures timely protection against multiple diseases, reduces the number of clinic visits, and improves adherence to vaccination schedules, particularly in populations with limited healthcare access.
However, simultaneous vaccination raises concerns about immune interference and increased reactogenicity. Studies have shown that certain vaccine combinations, such as MMR (measles, mumps, rubella) and varicella, can elicit robust immune responses when given together, while others, like hepatitis B and DTaP, may require careful consideration due to potential interactions. For example, a 2012 study published in *Pediatrics* found that infants who received the inactivated influenza vaccine concurrently with PCV13 had slightly lower antibody responses to certain pneumococcal serotypes compared to those vaccinated sequentially. This highlights the need for evidence-based guidelines to optimize vaccine co-administration.
Sequential vaccination, spacing vaccines over multiple visits, offers the advantage of minimizing side effects and allowing for clearer attribution of adverse reactions to specific vaccines. This approach is often preferred for older adults or individuals with compromised immune systems, where the risk of overwhelming the immune system is higher. For example, the shingles vaccine (Shingrix) is typically administered in two doses, 2–6 months apart, to maximize efficacy while reducing the likelihood of severe local reactions, such as injection site pain or swelling. Sequential scheduling also provides flexibility for patients who experience significant side effects after the first dose, allowing for adjustments in timing or dosage.
Practical considerations play a critical role in choosing between simultaneous and sequential vaccination. For parents of young children, simultaneous administration simplifies the immunization process, reducing the stress of multiple clinic visits and ensuring timely completion of the vaccine series. Healthcare providers must weigh these benefits against the potential for increased fever, fussiness, or other mild reactions, which, while generally harmless, can be concerning for caregivers. Clear communication about expected side effects and the rationale behind vaccine spacing is essential to build trust and ensure compliance.
Ultimately, the choice between simultaneous and sequential vaccination should be guided by individual patient factors, vaccine-specific data, and public health priorities. Pediatric populations often benefit from simultaneous administration due to its efficiency and proven safety profile, while older adults or immunocompromised individuals may require a more tailored, sequential approach. As vaccine schedules continue to evolve, ongoing research and clinical guidelines will remain critical in optimizing immunization strategies to maximize protection while minimizing risks.
Understanding Booster Vaccine Names: A Comprehensive Guide for Informed Choices
You may want to see also
Explore related products






![]()
Immune System Considerations: How health conditions or immunocompromised states affect vaccine spacing
The immune system's ability to respond to vaccines is a delicate balance, and for individuals with compromised immunity, this balance becomes even more critical. Immunocompromised patients, such as those undergoing cancer treatment, living with HIV, or taking immunosuppressive medications, often require a tailored approach to vaccination. The spacing of vaccines in these cases is not just a matter of convenience but a strategic decision to ensure optimal immune response without overwhelming the body.
Understanding the Challenge: Immunocompromised individuals face a unique dilemma. Their bodies may struggle to mount a sufficient immune response to vaccines, leaving them vulnerable to preventable diseases. For instance, a study on solid organ transplant recipients found that the immune response to the influenza vaccine was significantly lower compared to healthy controls, emphasizing the need for careful vaccine management in this population. The challenge lies in stimulating the immune system enough to provide protection without causing adverse effects.
Strategic Spacing for Optimal Response: In these cases, healthcare providers often adopt a personalized vaccine schedule. For instance, the CDC recommends that for individuals with HIV, the measles, mumps, and rubella (MMR) vaccine should be administered at least 4 weeks apart from other live vaccines. This spacing allows the immune system to focus on one vaccine at a time, potentially improving the overall response. Similarly, for patients on chemotherapy, it is advised to complete the vaccine series before starting treatment or to wait until 3-6 months after chemotherapy, depending on the regimen, to ensure the body can generate an adequate immune reaction.
Practical Considerations: Age and the type of immunocompromise play a significant role in vaccine spacing decisions. For example, in children with leukemia, the timing of vaccinations is crucial. The American Cancer Society suggests that live vaccines should be administered during remission, and inactivated vaccines can be given during or after treatment, but with careful consideration of the child's immune status. Additionally, for older adults with age-related immune decline, the spacing between booster doses might be adjusted to ensure continued protection.
A Tailored Approach: The key takeaway is that vaccine spacing is not a one-size-fits-all strategy. For immunocompromised individuals, it is a precise science, requiring careful planning and monitoring. Healthcare professionals must consider the patient's medical history, current health status, and the specific vaccines required to create an effective schedule. This personalized approach ensures that vaccines are spaced optimally, providing the best chance of protection without compromising the individual's health. By understanding these immune system considerations, healthcare providers can make informed decisions, ultimately improving vaccine efficacy and patient outcomes.
Orlando Pharmacies Offering Yellow Fever Vaccines: Your Essential Guide
You may want to see also
Explore related products






![]()
Catch-Up Vaccination Strategies: Effective spacing for missed doses to ensure full immunization coverage
Missed vaccine doses can leave individuals vulnerable to preventable diseases, creating gaps in immunity that compromise both personal and public health. Catch-up vaccination strategies are crucial for bridging these gaps, but effective spacing is key to ensuring optimal immune response without overwhelming the body. The World Health Organization (WHO) and Centers for Disease Control and Prevention (CDC) provide guidelines for catch-up schedules, emphasizing flexibility while maintaining vaccine efficacy. For instance, inactivated vaccines like the DTaP (diphtheria, tetanus, pertussis) can often be administered at minimum intervals of 4 weeks, while live attenuated vaccines such as MMR (measles, mumps, rubella) typically require at least 4 weeks between doses but can be given simultaneously if more than 4 weeks have passed since the last dose.
Consider a child who missed their 12-month vaccinations, including MMR and varicella. A catch-up plan might involve administering MMR and varicella vaccines concurrently, as both are live attenuated but can be given together if the delay is significant. If additional doses are needed, spacing them 4–8 weeks apart ensures the immune system responds adequately. For adolescents or adults with incomplete series, the approach may differ. For example, the HPV vaccine (human papillomavirus) can be given in a 2-dose schedule for those initiating the series before age 15, with a 6–12 month interval, while those starting after age 15 require 3 doses spaced over 6 months. Tailoring the catch-up schedule to age, vaccine type, and previous doses is essential for maximizing protection.
One common challenge in catch-up vaccination is balancing urgency with safety. Overcrowding doses can lead to reduced efficacy or adverse reactions, while excessive delays prolong vulnerability. For combination vaccines like the pentavalent vaccine (diphtheria, tetanus, pertussis, hepatitis B, and *Haemophilus influenzae* type b), adhering to minimum intervals of 4 weeks between doses is critical. In resource-limited settings, healthcare providers often prioritize completing the series over strict adherence to intervals, as partial immunity is better than none. However, in well-resourced environments, precision in spacing ensures the highest possible immune response, particularly for vaccines requiring multiple doses to confer full protection, such as hepatitis B or pneumococcal vaccines.
Practical tips for implementing catch-up strategies include using immunization registries to track missed doses, setting reminders for follow-up appointments, and educating caregivers about the importance of timely completion. For example, a 7-year-old with incomplete DTaP and IPV (inactivated polio vaccine) series could receive the final doses at least 6 months after the previous dose, ensuring long-term immunity. In cases of significant delays, healthcare providers may opt for accelerated schedules, such as administering 3 doses of hepatitis B vaccine over 2 months (0, 1, 2 months) for rapid protection in high-risk individuals. Flexibility, combined with adherence to evidence-based intervals, ensures catch-up efforts are both safe and effective.
Ultimately, catch-up vaccination strategies require a personalized approach, considering the individual’s age, vaccine type, and immunization history. By adhering to minimum intervals while avoiding unnecessary delays, healthcare providers can close immunity gaps efficiently. For instance, a teenager with missed Tdap (tetanus, diphtheria, pertussis) and meningococcal doses can receive both vaccines during the same visit, provided they are due. This dual approach not only saves time but also reinforces the importance of comprehensive immunization. Effective catch-up spacing is not just about following rules—it’s about restoring protection and safeguarding health in a world where preventable diseases remain a threat.
Global Race for COVID-19 Vaccine: Who's Leading the Charge?
You may want to see also
Frequently asked questions
Vaccines for infants and young children are typically spaced according to the recommended immunization schedule provided by health authorities like the CDC or WHO. Most vaccines are given in a series, with doses spaced 4 to 8 weeks apart, depending on the vaccine. For example, the DTaP, IPV, and Hib vaccines often follow a 2, 4, and 6-month schedule. Always consult a healthcare provider for personalized guidance.
Multiple vaccines can and often are given at the same visit to ensure timely protection and reduce the number of clinic visits. Health authorities confirm that this practice is safe and effective. However, some vaccines, like those for COVID-19 and the flu, may be recommended at different times unless specifically advised otherwise by a healthcare provider.
The spacing of COVID-19 vaccine doses depends on the specific vaccine and local guidelines. For mRNA vaccines (Pfizer-BioNTech and Moderna), the initial doses are typically spaced 3 to 4 weeks apart, while booster doses are recommended 5 to 6 months later. For the Johnson & Johnson vaccine, a second dose is advised 2 months after the first. Always follow updated recommendations from health authorities.
Delaying vaccines beyond the recommended schedule is not advised, as it leaves individuals vulnerable to preventable diseases. The spacing in vaccine schedules is carefully studied to ensure safety and effectiveness while minimizing side effects. If you have concerns about side effects, discuss them with a healthcare provider rather than altering the schedule.
For adults, vaccine spacing depends on the specific vaccines needed. Some vaccines, like Tdap (tetanus, diphtheria, pertussis), can be given at any time if due. Others, such as HPV or hepatitis B vaccines, may require specific intervals (e.g., 1-2 months between doses). For catch-up immunizations, healthcare providers will create a schedule to ensure all necessary vaccines are administered as quickly and safely as possible.