The timeline for vaccine availability is a critical question in the face of emerging or ongoing public health crises, and it depends on several factors, including the nature of the pathogen, existing research, regulatory processes, and manufacturing capabilities. Typically, vaccine development can take several years, but in urgent situations, such as the COVID-19 pandemic, accelerated efforts and global collaboration have significantly shortened this timeframe. From the identification of the virus to the distribution of vaccines, the process involves preclinical testing, multiple phases of clinical trials, regulatory approval, and mass production. While some vaccines, like those for COVID-19, have been developed and deployed within a year, others may take longer due to scientific challenges or the need for extensive safety and efficacy data. Public health officials often emphasize the importance of balancing speed with safety to ensure that any available vaccine is both effective and trustworthy.
| Characteristics | Values |
|---|---|
| Current Timeline (as of 2023) | Vaccines for COVID-19 are already widely available globally. |
| Development Time for New Vaccines | Typically 5-10 years, but expedited to 1-2 years during the COVID-19 pandemic. |
| Emergency Use Authorization (EUA) | Allows rapid deployment during public health emergencies. |
| Manufacturing Scale-Up | 6-12 months after clinical trials, depending on infrastructure. |
| Distribution Challenges | Logistics, cold chain requirements, and equitable access impact timelines. |
| Booster Updates | 3-6 months to develop and deploy updated vaccines for new variants. |
| Regulatory Approval | 1-3 months for full approval after EUA, depending on data submission. |
| Global Collaboration | Accelerates development and distribution through initiatives like COVAX. |
| Public Hesitancy Impact | Delays uptake but does not affect vaccine availability timelines. |
| Future Pandemic Preparedness | Platforms like mRNA technology could reduce development time to 3-6 months. |
Explore related products






What You'll Learn
![]()
Clinical trial phases and timelines
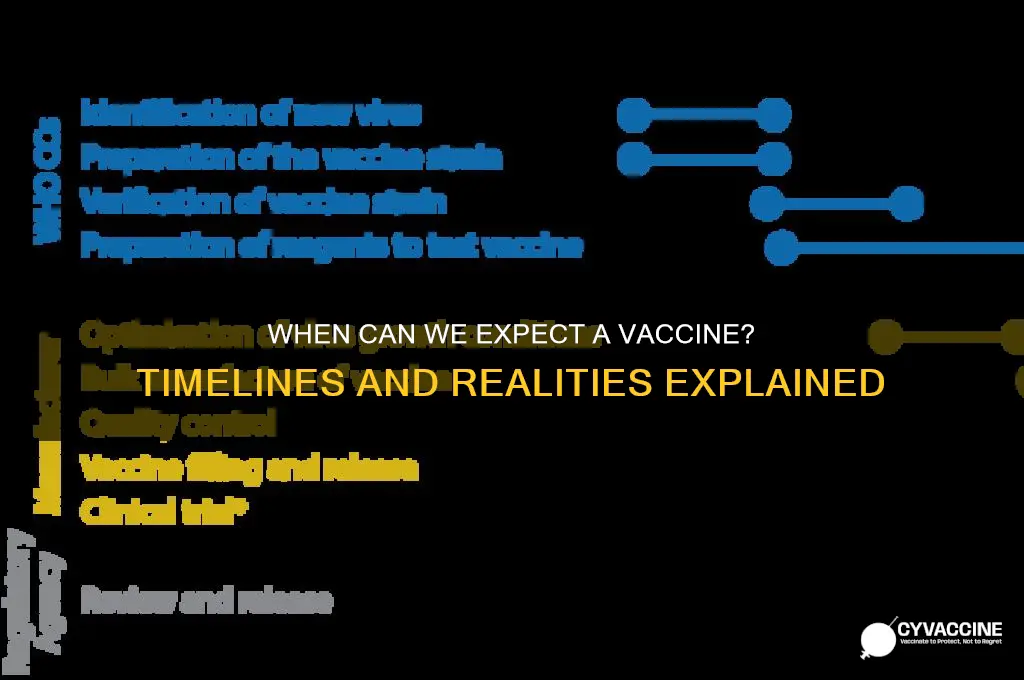
Vaccine development is a complex, multi-stage process that ensures safety and efficacy before public distribution. Understanding the clinical trial phases and their timelines is crucial for grasping how soon a vaccine could become available. Each phase serves a distinct purpose, from initial safety checks to large-scale efficacy trials, and each step is subject to rigorous regulatory oversight.
Phase 1: Safety First
In this exploratory stage, the vaccine is administered to a small group of healthy volunteers, typically 20–100 individuals. The primary goal is to assess safety, monitor side effects, and determine the appropriate dosage. For instance, a COVID-19 vaccine trial might start with doses ranging from 10 to 100 micrograms to identify the optimal amount that balances immune response and tolerability. This phase usually takes 2–3 months but can extend if unexpected adverse reactions occur. Participants are closely monitored through blood tests and physical exams to ensure the vaccine doesn’t cause harm.
Phase 2: Efficacy and Immunogenicity
Once safety is established, Phase 2 expands to include several hundred subjects, often targeting specific demographics like older adults or those with underlying conditions. This phase evaluates the vaccine’s ability to generate an immune response (immunogenicity) and refines dosage levels. For example, a flu vaccine trial might test whether a 15-microgram dose produces sufficient antibodies in individuals over 65. This stage typically lasts 6–8 months, as researchers analyze data to ensure the vaccine not only works but also performs consistently across diverse populations.
Phase 3: Large-Scale Testing
Here, the vaccine is administered to thousands of participants in a randomized, placebo-controlled trial. The goal is to confirm efficacy in preventing disease and to identify rare side effects that might not have appeared in smaller groups. For a vaccine like HPV, Phase 3 trials might involve 15,000 adolescents and young adults, tracking outcomes over 1–2 years. This phase is the most time-consuming, often lasting 1–4 years, depending on disease prevalence and trial design. Accelerated timelines, as seen during the COVID-19 pandemic, can compress this phase to 6–9 months through expedited enrollment and interim analyses.
Expedited Pathways and Practical Considerations
In emergencies, regulatory agencies like the FDA can employ expedited pathways, such as Emergency Use Authorization (EUA), to accelerate vaccine availability. However, even with these measures, Phase 3 data must still demonstrate clear benefits outweighing risks. Practical tips for trial participants include keeping a symptom diary, adhering to follow-up schedules, and reporting any unusual reactions promptly. For the public, understanding these timelines helps manage expectations—a vaccine that skips steps risks compromising safety, while one that follows the full process ensures trust and long-term efficacy.
Utah's COVID-19 Vaccine Rollout: Tracking Administered Doses and Progress
You may want to see also
Explore related products






![]()
Manufacturing and scaling production capacity
The race to produce a vaccine often hinges on manufacturing and scaling production capacity, a complex process that can make or break timelines. Once a vaccine candidate proves safe and effective in clinical trials, the real challenge begins: producing billions of doses quickly and consistently. This requires a delicate balance of technology, infrastructure, and global collaboration.
Consider the logistical hurdles. A single dose of a vaccine might require as little as 0.5 mL of liquid, but for a global population, this translates to massive volumes. For instance, vaccinating 70% of the world’s 8 billion people would require 5.6 billion doses, or 2.8 billion liters of vaccine. Traditional manufacturing facilities, designed for annual flu vaccines or routine immunizations, cannot meet this demand overnight. Scaling up involves expanding existing facilities, repurposing factories, and even building new ones—a process that typically takes years, not months.
To accelerate production, manufacturers often employ innovative strategies. One approach is technology transfer, where the vaccine’s developer shares its formula and production methods with other companies worldwide. For example, during the COVID-19 pandemic, Moderna partnered with Lonza Group to increase production, while AstraZeneca collaborated with the Serum Institute of India. Another strategy is platform-based manufacturing, using systems like mRNA or viral vectors that allow for rapid adaptation to new pathogens. These platforms reduce the time needed to retool facilities, as the same production lines can be used for different vaccines with minor adjustments.
However, scaling production isn’t just about quantity—it’s also about quality. Each dose must meet stringent regulatory standards for safety and efficacy. This requires rigorous testing at every stage, from raw materials to final packaging. For instance, mRNA vaccines must be stored at ultra-cold temperatures (-70°C), demanding specialized equipment and cold chain logistics. Even a small deviation in temperature or formulation can render doses unusable, highlighting the need for precision at scale.
Despite these challenges, recent advancements offer hope. Governments and private sectors are investing in flexible manufacturing hubs that can quickly pivot to produce vaccines for emerging threats. Initiatives like the Coalition for Epidemic Preparedness Innovations (CEPI) are funding research into rapid-response platforms. Additionally, pre-approval of manufacturing sites and bulk production of vaccine components (e.g., adjuvants or lipid nanoparticles) can shave months off timelines. While manufacturing and scaling remain bottlenecks, strategic planning and innovation are steadily reducing the time it takes to deliver vaccines to those who need them most.
Effective Ways to Reduce Swelling After Getting Vaccinated
You may want to see also
Explore related products






![]()
Regulatory approval and emergency use
Regulatory approval is the final hurdle before a vaccine can reach the public, but it’s not a one-size-fits-all process. In the U.S., the FDA typically requires Phase 3 clinical trial data demonstrating safety and efficacy, a process that historically takes years. However, during public health emergencies, the FDA can issue Emergency Use Authorization (EUA), a faster pathway that allows temporary use of a vaccine based on less extensive data. For example, the COVID-19 vaccines from Pfizer and Moderna received EUA in December 2020 after just eight months of development, a record-breaking timeline. This expedited process balances urgency with safety, requiring manufacturers to meet specific criteria, such as at least two months of safety data following vaccination.
The EUA process, while faster, is not a shortcut. It demands rigorous evidence, including clear benefits outweighing risks and well-defined conditions for use. For instance, COVID-19 vaccines under EUA were initially approved for individuals aged 16 and older, with Pfizer later expanding to ages 12–15 after additional trials. Dosage instructions are also critical: Pfizer’s vaccine requires two 30-microgram doses spaced 21 days apart, while Moderna’s uses two 100-microgram doses spaced 28 days apart. These specifics ensure consistency and safety, even under emergency conditions.
Globally, regulatory approval varies widely, creating disparities in vaccine availability. The WHO’s Emergency Use Listing (EUL) accelerates access in low-income countries by assessing vaccines for international use. For example, AstraZeneca’s vaccine received EUL in February 2021, enabling its distribution through COVAX. However, some countries, like India, have their own expedited pathways, such as the Restricted Emergency Use Approval, which allowed Bharat Biotech’s Covaxin to be deployed despite limited Phase 3 data. These differences highlight the tension between speed and standardization in global health crises.
Practical tips for navigating regulatory approval include early engagement with regulators, transparent data sharing, and clear communication of risks and benefits. Manufacturers must also prepare for post-authorization studies to monitor long-term safety and efficacy. For the public, understanding EUA limitations is key: vaccines under EUA are not fully approved, and informed consent is required. For example, recipients should be aware of potential side effects, such as fatigue or fever, and follow dosage instructions precisely to ensure protection.
In conclusion, regulatory approval and emergency use pathways are critical determinants of vaccine availability timelines. While EUA offers a faster route, it maintains safety standards through specific criteria and conditions. Global variations in approval processes underscore the need for collaboration and harmonization. For both manufacturers and the public, clarity, transparency, and adherence to guidelines are essential to ensure vaccines are both available and trustworthy.
Jacksonville, Florida: Locating Your Vaccination Records – A Comprehensive Guide
You may want to see also
Explore related products






![]()
Distribution and supply chain challenges
The COVID-19 pandemic underscored the complexity of vaccine distribution, revealing that developing a vaccine is only half the battle. Once available, the logistical hurdles of transporting, storing, and administering doses to billions became the next critical challenge. For instance, the Pfizer-BioNTech vaccine requires ultra-cold storage at -70°C, a condition that many low-income countries struggle to meet due to inadequate infrastructure. This temperature sensitivity isn’t just a technical detail—it directly impacts how quickly vaccines can reach remote or underserved populations.
Consider the supply chain as a relay race, where each handoff must be seamless. From manufacturing plants to airports, warehouses, and finally clinics, every step requires precise coordination. Delays at any stage—whether due to customs clearance, refrigeration failures, or transportation bottlenecks—can render doses ineffective. For example, a single shipment of 10,000 doses delayed by 24 hours could mean thousands of missed vaccinations, especially in regions with limited storage capacity. This fragility highlights the need for robust contingency plans, such as investing in portable cold storage units or training local staff to handle temperature-sensitive cargo.
Another layer of complexity arises from the inequitable distribution of resources. Wealthier nations often secure vaccine doses in advance, leaving low-income countries to wait months or even years. COVAX, a global initiative aimed at equitable distribution, faced significant challenges in 2021 due to supply shortages and export restrictions. To address this, governments and manufacturers must prioritize transparency and collaboration. For instance, sharing production schedules and waiving intellectual property rights could accelerate global access. Practical steps include establishing regional manufacturing hubs in Africa and Asia to reduce reliance on distant suppliers.
Finally, the "last mile" of distribution—getting vaccines into arms—requires tailored strategies. In rural areas, mobile clinics and drone deliveries have proven effective, while urban centers benefit from mass vaccination sites. Age-specific considerations, such as prioritizing elderly populations or ensuring child-friendly formulations, further complicate logistics. For example, a 0.5 mL dose for children under 12 requires different packaging and administration protocols than a 0.3 mL booster for adults. Clear communication and training for healthcare workers are essential to avoid errors. By addressing these challenges systematically, the timeline for vaccine availability can be shortened, saving lives and restoring normalcy faster.
Australia's Vaccination Progress: Tracking the Number of Vaccinated Individuals
You may want to see also
Explore related products






![]()
Public acceptance and vaccination rates
The speed at which a vaccine becomes available is only half the battle; its success hinges on public acceptance and vaccination rates. Historical data shows that even the most effective vaccines fail to curb disease if uptake is low. For instance, the measles vaccine, with a 97% efficacy rate, still sees outbreaks in communities where vaccination rates dip below 95%. This threshold, known as herd immunity, is critical for protecting vulnerable populations who cannot receive vaccines due to medical reasons. Without widespread acceptance, even a rapidly developed vaccine may fall short of its potential.
To boost vaccination rates, public health campaigns must address hesitancy head-on. A 2020 study found that 20% of respondents were unsure about receiving a COVID-19 vaccine, citing concerns over safety and side effects. Tailored messaging can mitigate this: emphasizing the rigorous testing phases (Phase I to III trials involving thousands of participants) and transparent communication about common side effects (e.g., soreness at the injection site, mild fever) can build trust. Additionally, leveraging trusted community leaders—such as healthcare workers or religious figures—to endorse vaccination can be more effective than broad, impersonal campaigns.
Practical barriers also play a significant role in vaccination rates. For example, requiring two doses of a vaccine, spaced 3–4 weeks apart, can deter individuals with limited access to healthcare or transportation. Simplifying the process—such as offering mobile clinics in underserved areas or extending clinic hours—can improve uptake. Similarly, clear instructions on scheduling second doses, perhaps via text reminders, can reduce missed appointments. For children, bundling vaccines with routine check-ups (e.g., combining the flu shot with a 5-year-old’s well-child visit) streamlines the process for parents.
Comparing vaccination campaigns reveals that incentives can tip the balance. In 2021, Ohio’s Vax-a-Million lottery, offering $1 million prizes to vaccinated residents, saw a 43% increase in vaccinations among eligible age groups. While not all regions can replicate such large-scale incentives, smaller rewards—like gift cards, discounts, or paid time off for vaccination—have proven effective. Employers and schools can play a pivotal role here, offering perks to vaccinated individuals while ensuring policies are inclusive and non-coercive.
Ultimately, the interplay between vaccine availability and public acceptance requires a multi-faceted approach. While scientific advancements may deliver a vaccine in record time, its impact depends on how well it is received. By addressing hesitancy, removing logistical barriers, and employing strategic incentives, public health officials can ensure that vaccination rates meet the demands of herd immunity. The goal isn’t just to make vaccines available—it’s to make them accessible, trusted, and embraced by the communities they aim to protect.
Atlantic City Convention Center: COVID-19 Vaccine Options and Availability
You may want to see also
Frequently asked questions
Developing a new vaccine typically takes 10–15 years, but in emergencies like a pandemic, this timeline can be accelerated to 12–18 months with global collaboration and expedited regulatory processes.
Distribution speed depends on manufacturing capacity, supply chain logistics, prioritization of high-risk groups, and public acceptance of the vaccine.
Yes, in urgent situations like a global health crisis, vaccines can be developed and distributed in under a year, as seen with COVID-19 vaccines, thanks to unprecedented global cooperation and funding.
After approval, distribution begins immediately, but availability varies by region and population group, with high-risk individuals and healthcare workers typically receiving it first.