The development of a vaccine for the coronavirus, specifically SARS-CoV-2, has been a global priority since the outbreak of the COVID-19 pandemic. Typically, vaccine development can take several years, involving rigorous research, clinical trials, and regulatory approvals. However, the unprecedented urgency of the pandemic accelerated this process, with scientists, governments, and pharmaceutical companies collaborating to expedite timelines. By early 2021, multiple vaccines, such as those developed by Pfizer-BioNTech, Moderna, and AstraZeneca, were authorized for emergency use in various countries, marking a remarkable achievement in medical history. Despite this progress, the timeline for widespread availability and distribution varied globally, influenced by factors like production capacity, logistics, and equitable access. Ongoing research continues to address emerging variants and improve vaccine efficacy, ensuring long-term protection against the virus.
| Characteristics | Values |
|---|---|
| Current Status (as of October 2023) | Multiple vaccines approved and widely distributed globally. |
| Vaccine Types | mRNA (Pfizer-BioNTech, Moderna), Viral Vector (AstraZeneca, J&J), Protein-based (Novavax), Inactivated (Sinovac, Sinopharm). |
| Efficacy | 60-95% depending on the vaccine type and variant. |
| Booster Recommendations | Boosters advised for enhanced protection, especially against variants. |
| Development Timeline | ~1 year (unprecedented speed due to global collaboration and funding). |
| Global Distribution | Over 13 billion doses administered worldwide (as of October 2023). |
| Ongoing Research | Focus on variant-specific vaccines and next-generation technologies. |
| Challenges | Vaccine hesitancy, equitable distribution, and variant adaptability. |
| Long-Term Immunity | Studies ongoing; boosters likely needed for sustained protection. |
| Side Effects | Generally mild (e.g., soreness, fatigue); rare severe cases (e.g., myocarditis). |
Explore related products

$29.95 $25.48

$2.74 $24.95




What You'll Learn
- Current Vaccine Development Stages: Overview of ongoing clinical trials and phases for COVID-19 vaccines globally
- Challenges in Vaccine Production: Supply chain, manufacturing, and distribution hurdles affecting vaccine availability timelines
- Regulatory Approval Process: Steps and timelines for emergency use authorization and full approval by health agencies
- Efficacy and Safety Testing: Ensuring vaccines meet required standards for effectiveness and minimal side effects
- Global Distribution Equity: Addressing disparities in vaccine access between developed and developing countries
![]()
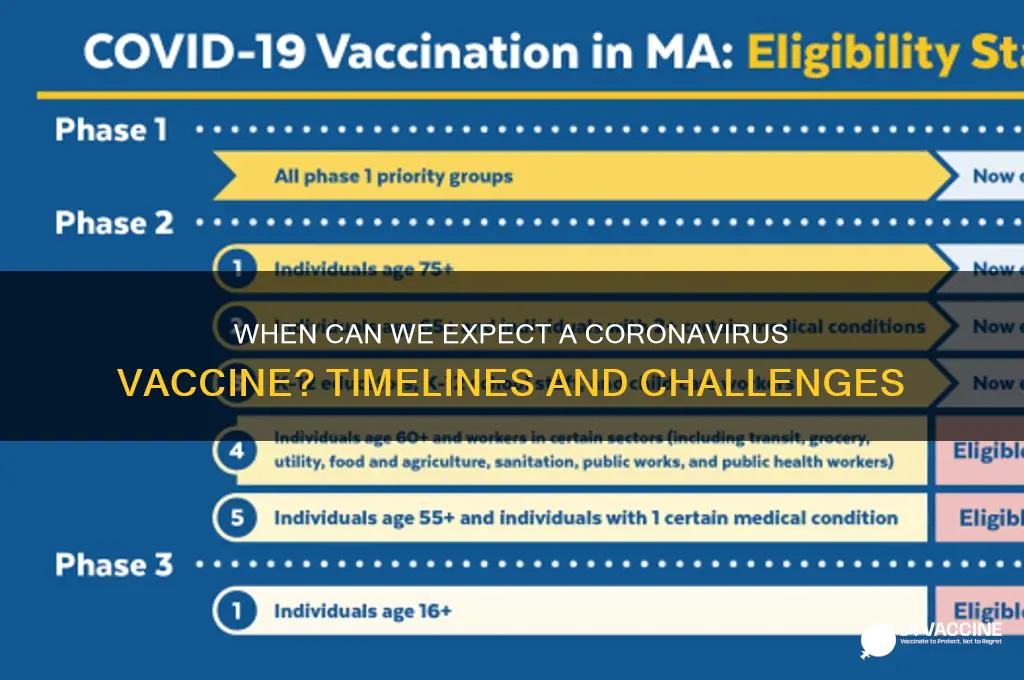
Current Vaccine Development Stages: Overview of ongoing clinical trials and phases for COVID-19 vaccines globally
The race to develop a COVID-19 vaccine has been unprecedented, with over 200 candidates in various stages of development globally. As of the latest updates, several vaccines have progressed through clinical trials, offering a glimmer of hope in the fight against the pandemic. Understanding the current vaccine development stages is crucial for grasping how soon a vaccine might become widely available.
Phase 1 Trials: Safety and Dosage
In this initial stage, vaccines are tested on a small group of healthy volunteers (typically 20–100 individuals) to assess safety, dosage levels, and immune response. For instance, Moderna’s mRNA-1273 vaccine began Phase 1 trials in March 2020, testing doses of 25, 100, and 250 micrograms. Similarly, AstraZeneca’s AZD1222 vaccine, developed with the University of Oxford, initiated Phase 1 trials with a focus on safety and immunogenicity in adults aged 18–55. These trials are critical for identifying potential side effects and determining the optimal dose for further testing.
Phase 2 Trials: Expanded Testing and Immunogenicity
Once a vaccine is deemed safe, Phase 2 trials expand to include several hundred participants, often targeting specific age groups or populations at higher risk. Pfizer and BioNTech’s BNT162b2 vaccine, for example, enrolled participants aged 18–85 in Phase 2/3 trials to evaluate efficacy across diverse demographics. This phase also refines the vaccine’s ability to induce an immune response. Johnson & Johnson’s Janssen vaccine tested a single-dose regimen in Phase 2, a unique approach compared to the two-dose strategies of Pfizer and Moderna.
Phase 3 Trials: Efficacy and Large-Scale Testing
Phase 3 trials are the most critical, involving tens of thousands of participants to determine the vaccine’s efficacy in preventing COVID-19. These trials often include placebo groups and are conducted across multiple countries to ensure diverse representation. For instance, Pfizer and BioNTech’s Phase 3 trial enrolled 43,000 participants globally, reporting a 95% efficacy rate in preventing symptomatic COVID-19. Similarly, AstraZeneca’s trial involved 30,000 participants in the U.S., U.K., Brazil, and South Africa, demonstrating 70–90% efficacy depending on dosage.
Emergency Use Authorization and Rollout
Following successful Phase 3 trials, vaccines can seek emergency use authorization (EUA) from regulatory bodies like the FDA or EMA. Pfizer’s vaccine received EUA in December 2020, followed by Moderna’s shortly after. AstraZeneca’s vaccine has been authorized in the U.K. and several other countries but faced scrutiny over dosing regimens and rare side effects. Practical tips for the public include staying informed about vaccine availability in their region, understanding dosage schedules (e.g., Pfizer’s 21-day interval, Moderna’s 28-day interval), and being aware of potential side effects like fatigue or fever.
Global Collaboration and Challenges
The rapid progress in vaccine development is a testament to global collaboration, with governments, pharmaceutical companies, and research institutions working together. However, challenges remain, including ensuring equitable distribution, addressing vaccine hesitancy, and monitoring for long-term safety. Initiatives like COVAX aim to provide vaccines to low-income countries, but supply chain logistics and storage requirements (e.g., Pfizer’s ultra-cold storage needs) pose significant hurdles.
In summary, while several COVID-19 vaccines have advanced through clinical trials and are being distributed globally, ongoing monitoring and equitable access remain critical. Understanding the development stages helps demystify the timeline and underscores the importance of continued vigilance in the fight against the pandemic.
US Vaccination Progress: State-by-State Breakdown of Inoculated Residents
You may want to see also
Explore related products






![]()
Challenges in Vaccine Production: Supply chain, manufacturing, and distribution hurdles affecting vaccine availability timelines
The race to produce a coronavirus vaccine has been unprecedented, but the journey from lab to arm is fraught with challenges. One of the most critical bottlenecks lies in the supply chain, where raw materials like bioreactor bags, cell culture media, and specialized glass vials are in short supply. For instance, a single dose of the Pfizer-BioNTech vaccine requires up to 280 components sourced from 19 countries. When just one supplier faces delays, the entire production line grinds to a halt. This fragility was exposed in early 2021 when a shortage of lipid nanoparticles—a key ingredient in mRNA vaccines—threatened to slow global distribution. Manufacturers are now scrambling to diversify suppliers and build redundancy, but this takes time and investment, delaying timelines further.
Manufacturing itself is another hurdle, particularly for novel vaccine platforms like mRNA. Producing mRNA vaccines involves complex processes, such as synthesizing genetic material and encapsulating it in lipid nanoparticles, which require highly specialized equipment and expertise. For example, the Pfizer-BioNTech vaccine must be stored at -70°C, demanding ultra-cold freezers that are scarce in many regions. Scaling up production to meet global demand has proven difficult, with facilities often operating at or near capacity. Even a minor deviation in temperature or humidity during production can render batches unusable, leading to costly setbacks. Training personnel to handle these advanced techniques adds another layer of complexity, further extending timelines.
Distribution presents its own set of challenges, especially in low- and middle-income countries. The Pfizer vaccine’s stringent storage requirements make it impractical for many regions lacking advanced infrastructure. In contrast, the AstraZeneca vaccine, which can be stored at refrigerator temperatures, is more accessible but has faced production delays due to supply chain issues and regulatory hurdles. Additionally, the "last mile" of delivery—getting vaccines from distribution centers to remote areas—requires robust cold chains, reliable transportation, and trained healthcare workers. For example, in rural India, where electricity is unreliable, solar-powered refrigerators have been deployed, but such solutions are expensive and not universally available.
Finally, equitable distribution remains a moral and logistical challenge. Wealthy nations have hoarded vaccine doses, leaving poorer countries with limited access. COVAX, the global initiative to ensure fair distribution, has faced funding shortfalls and supply disruptions, falling far behind its targets. For instance, as of mid-2021, Africa had received less than 2% of global vaccine doses, despite accounting for 17% of the world’s population. This disparity not only prolongs the pandemic but also allows new variants to emerge, potentially undermining vaccine efficacy worldwide. Addressing these distribution inequities requires international cooperation, financial commitment, and innovative solutions to ensure vaccines reach those who need them most.
In summary, the path to widespread vaccine availability is riddled with supply chain, manufacturing, and distribution challenges. From raw material shortages to ultra-cold storage requirements, each hurdle adds layers of complexity and delay. Overcoming these obstacles demands global collaboration, investment in infrastructure, and creative problem-solving. Only by addressing these issues holistically can we hope to accelerate vaccine timelines and bring the pandemic under control.
Healthcare Workers and COVID-19 Vaccines: Uptake, Hesitancy, and Implications
You may want to see also
Explore related products






![]()
Regulatory Approval Process: Steps and timelines for emergency use authorization and full approval by health agencies
The journey from vaccine development to public availability is a complex race against time, especially during a global health crisis. Regulatory approval is a critical phase, ensuring safety and efficacy while balancing the urgent need for a solution. This process involves multiple steps, each with its own timeline and challenges, particularly when considering emergency use authorization (EUA) versus full approval.
The Emergency Use Authorization (EUA) Pathway:
In the context of the COVID-19 pandemic, health agencies like the U.S. Food and Drug Administration (FDA) and the European Medicines Agency (EMA) have employed the EUA mechanism to expedite access to vaccines. This process is designed for emergency situations, allowing the use of medical products without the extensive data typically required for full approval. For instance, the Pfizer-BioNTech COVID-19 vaccine received EUA from the FDA in December 2020, just 11 months after the genetic sequence of the virus was shared publicly. This rapid authorization was based on data from a clinical trial involving approximately 44,000 participants, demonstrating 95% efficacy in preventing COVID-19. The EUA process typically involves a rolling review of data as it becomes available, enabling regulators to assess safety and efficacy in real-time. This approach significantly reduces the time between trial completion and vaccine availability, often from years to months.
Steps Towards Full Approval:
Full approval, or licensure, requires a more comprehensive dataset and a longer-term follow-up. After EUA, manufacturers continue to collect data, including long-term safety information and additional efficacy data from ongoing trials. For full approval, regulators scrutinize every aspect of the vaccine, from manufacturing processes to quality control. This includes inspecting production facilities and reviewing data on the vaccine's stability, ensuring consistent quality across batches. The FDA, for example, requires at least six months of follow-up data on clinical trial participants to assess long-term safety and efficacy. This extended observation period is crucial for identifying rare side effects that may not appear in the initial trials.
Timelines and Public Health Considerations:
The timeline for full approval can vary, but it typically takes several months to a year after EUA. For instance, the Pfizer-BioNTech vaccine received full FDA approval in August 2021, eight months after its EUA. This process is more rigorous, providing a higher level of assurance regarding the vaccine's safety and efficacy. However, during a public health emergency, the benefits of rapid EUA must be weighed against the need for long-term data. Health agencies often communicate the known benefits and risks to the public, ensuring informed decision-making.
Global Collaboration and Standardization:
The COVID-19 pandemic has highlighted the importance of global collaboration in regulatory processes. Health agencies worldwide have worked together to streamline approval processes, sharing data and best practices. This collaboration has led to the rapid approval of multiple vaccines, ensuring a diverse range of options for different populations. Standardizing certain aspects of the approval process, such as data requirements and safety monitoring, can further expedite vaccine availability during future health crises.
In summary, the regulatory approval process for vaccines involves a delicate balance between speed and thoroughness. Emergency use authorization provides a rapid response mechanism, while full approval ensures long-term safety and efficacy. Understanding these steps and timelines is crucial for managing public expectations and making informed decisions during a pandemic. As the world continues to battle COVID-19 and prepare for future health challenges, the efficiency and transparency of regulatory processes will remain a key focus.
Excessive DTaP Vaccines in Students: Potential Risks and Outcomes
You may want to see also
Explore related products






![]()
Efficacy and Safety Testing: Ensuring vaccines meet required standards for effectiveness and minimal side effects
Vaccine development is a meticulous process, and the race to create a coronavirus vaccine has brought unprecedented attention to its critical phases. Among these, efficacy and safety testing stand as non-negotiable pillars. Before any vaccine reaches the public, it must undergo rigorous trials to prove both its ability to prevent disease and its minimal risk of adverse effects. This dual requirement ensures that the cure doesn’t become a new problem.
Consider the phased approach to clinical trials. Phase I focuses on safety, testing the vaccine on a small group (20–100 volunteers) to evaluate dosage levels and identify side effects. For instance, a typical COVID-19 vaccine trial might start with doses ranging from 10 to 100 micrograms, monitoring participants for reactions like fever, fatigue, or injection site pain. Phase II expands to hundreds of participants, refining dosage and gathering more safety data while assessing immune response. Finally, Phase III involves thousands to tens of thousands of participants, comparing vaccinated individuals to a placebo group to determine efficacy—often defined as reducing disease incidence by at least 50%, as seen in Pfizer and Moderna’s mRNA vaccines.
However, efficacy isn’t the sole metric. Safety profiles are equally critical, particularly for diverse populations. For example, older adults, who are more susceptible to severe COVID-19, may respond differently to vaccines due to age-related immune decline. Similarly, pregnant individuals and those with comorbidities require specific safety data, often collected post-authorization through surveillance programs like the CDC’s V-safe. Rare side effects, such as anaphylaxis (occurring in ~2–5 cases per million doses for mRNA vaccines) or thrombosis with thrombocytopenia syndrome (TTS, linked to adenovirus vector vaccines), highlight the need for ongoing monitoring.
Practical tips for ensuring vaccine safety include transparent reporting of trial demographics, as underrepresentation of certain groups can delay detection of adverse events. Additionally, post-market surveillance tools like the Vaccine Adverse Event Reporting System (VAERS) allow healthcare providers and recipients to flag issues, ensuring rapid response to emerging risks. For individuals, understanding that mild side effects (e.g., soreness, headache) are normal can reduce anxiety, while knowing when to seek medical attention for severe reactions (e.g., difficulty breathing, persistent abdominal pain) is crucial.
In conclusion, efficacy and safety testing are not mere regulatory hurdles but essential safeguards. They balance the urgency of pandemic response with the imperative of public trust. By adhering to these standards, vaccines like those for COVID-19 have demonstrated remarkable effectiveness—up to 95% in preventing symptomatic disease—while maintaining acceptable safety profiles. This rigorous process ensures that when a vaccine is approved, it is both a shield against disease and a promise of protection.
Mastering Spider-Man's Pigeon Vaccine Mission: Tips and Tricks to Succeed
You may want to see also
Explore related products






![]()
Global Distribution Equity: Addressing disparities in vaccine access between developed and developing countries
The COVID-19 pandemic has starkly exposed the fault lines in global health equity, with vaccine distribution serving as a prime example. While wealthy nations have secured billions of doses, many low-income countries struggle to vaccinate even their most vulnerable populations. As of late 2021, some African nations had vaccinated less than 5% of their populations, compared to over 70% in several European countries. This disparity isn’t just a moral failure—it’s a strategic one, as unchecked virus spread in any region fuels mutations that threaten global progress. Addressing this imbalance requires more than goodwill; it demands structured, scalable solutions.
One critical step is diversifying vaccine manufacturing hubs. Currently, over 80% of vaccine production occurs in high-income countries, creating bottlenecks in supply chains and distribution. Establishing regional manufacturing centers in Africa, Southeast Asia, and Latin America could reduce dependency on imports and lower costs. For instance, the World Health Organization’s mRNA technology transfer hubs in South Africa and Brazil aim to empower local producers. However, this initiative faces hurdles like intellectual property restrictions and funding gaps. Governments and pharmaceutical companies must collaborate to waive patents temporarily and invest in infrastructure, ensuring these hubs can produce doses at scale.
Another key strategy is streamlining dose-sharing mechanisms. Programs like COVAX, designed to equitably distribute vaccines, have fallen short of their targets due to hoarding by wealthy nations and logistical challenges. To improve efficiency, donor countries should commit to sharing not just excess doses but also those with imminent expiration dates, paired with funding for cold-chain logistics. For example, a single-dose vaccine like Johnson & Johnson’s is ideal for hard-to-reach areas, but its distribution requires coordinated efforts to avoid wastage. Additionally, recipient countries need support in training healthcare workers and combating vaccine hesitancy through culturally tailored campaigns.
Finally, equitable distribution must prioritize high-risk groups globally, not just within individual countries. While wealthy nations vaccinate teenagers and administer boosters, healthcare workers and the elderly in poorer regions remain unprotected. A tiered approach could allocate 50% of global doses to low-income countries until they reach 70% coverage among vulnerable populations. This would require real-time data sharing and flexible distribution plans. For instance, if a shipment of Pfizer’s two-dose regimen is unavailable, switching to a single-dose alternative like AstraZeneca could prevent delays in protecting at-risk groups.
In conclusion, achieving global vaccine equity isn’t just about charity—it’s about rethinking systems. By decentralizing production, refining dose-sharing, and targeting high-risk groups, the world can move toward a more just and resilient response to pandemics. The lessons from COVID-19 are clear: leaving any nation behind leaves us all at risk.
What Does the DHPP Vaccine Vial Look Like? A Visual Guide
You may want to see also
Frequently asked questions
Vaccine development typically takes several years, but due to global efforts and advancements in technology, the first COVID-19 vaccines were developed and authorized for emergency use within about 11 months of the pandemic's start. However, timelines can vary depending on clinical trial results, regulatory approvals, and manufacturing capabilities.
Developing a safe and effective vaccine involves multiple stages, including research, preclinical testing, three phases of clinical trials, regulatory review, and mass production. Each step requires rigorous testing to ensure safety and efficacy, which cannot be rushed without compromising public health.
After approval, vaccine distribution depends on manufacturing capacity, supply chain logistics, and prioritization strategies. Initially, high-risk groups (e.g., healthcare workers, elderly) are vaccinated first, followed by the general public. Full global availability can take months to years, depending on production and equitable distribution efforts.