The development of a coronavirus vaccine has been a global priority since the outbreak of the COVID-19 pandemic, with unprecedented scientific collaboration and funding accelerating the process. While traditional vaccine development can take years, the urgency of the crisis has led to the rapid creation of multiple candidates, some of which have already been authorized for emergency use. However, the question of how realistic a widely available and effective vaccine is hinges on several factors, including the complexity of the virus, the speed of clinical trials, manufacturing scalability, and global distribution challenges. Additionally, public trust and vaccine hesitancy pose significant hurdles, as misinformation and skepticism could undermine vaccination efforts. Despite these obstacles, the progress made so far offers hope, but the timeline for achieving widespread immunity remains uncertain, emphasizing the need for continued caution and public health measures.
Explore related products

$126.09 $166.95





What You'll Learn
![]()
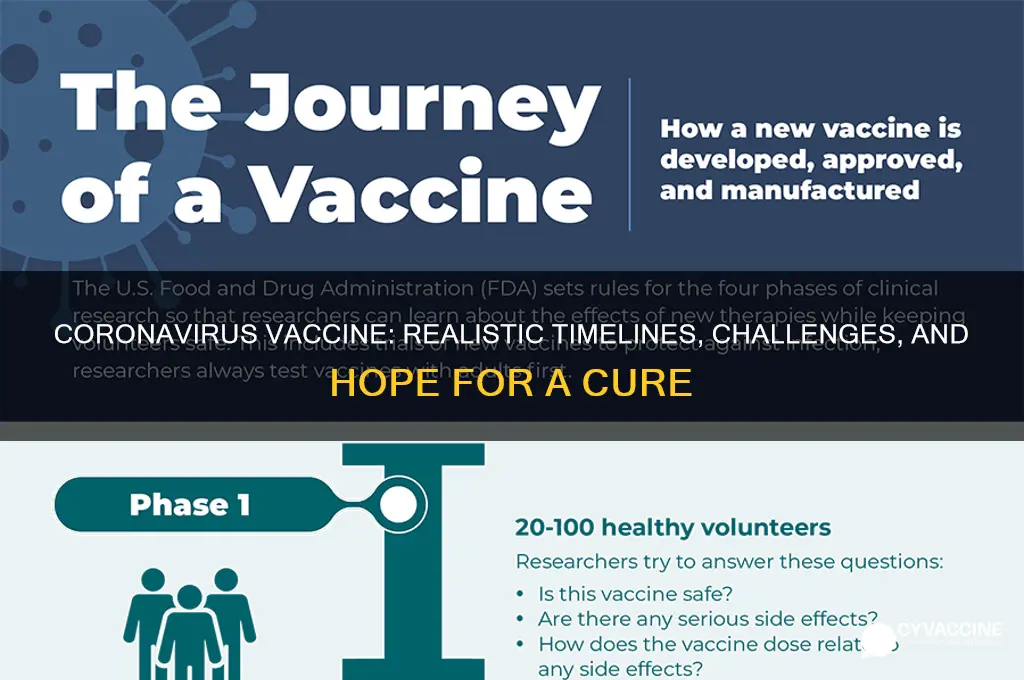
Current vaccine development timeline
The typical vaccine development process, from lab to market, spans 10–15 years. For COVID-19, this timeline has been compressed to 1–2 years, raising questions about safety and efficacy. How is this possible? Regulatory agencies like the FDA and WHO have streamlined approvals, allowing phases of testing to overlap and prioritizing emergency use authorizations. Manufacturers began large-scale production during clinical trials, a financial risk but a time-saver. Yet, shortcuts in testing duration don’t mean shortcuts in rigor—phase 3 trials for leading candidates still enrolled 30,000–45,000 participants to ensure safety and efficacy data.
Consider the mRNA vaccines, a novel technology central to this accelerated timeline. Unlike traditional vaccines, which use weakened viruses or proteins, mRNA vaccines deliver genetic instructions for cells to produce a viral protein, triggering an immune response. This platform allows for rapid design—Moderna’s mRNA-1273 took just 42 days from sequence selection to first human dosing. However, this speed relies on decades of prior research on mRNA stability and delivery systems, not on cutting corners. Dosage regimens, such as two 30-microgram injections of Pfizer’s vaccine spaced 21 days apart, were optimized through phase 1 and 2 trials to balance efficacy and side effects like fatigue or fever.
Comparatively, viral vector vaccines like AstraZeneca’s AZD1222 and Johnson & Johnson’s Janssen shot use a modified adenovirus to deliver genetic material. These vaccines offer a single-dose option (Janssen) or a lower-cost production model, making them viable for global distribution. However, rare side effects such as blood clots have prompted age-based restrictions—many countries limit AstraZeneca to individuals over 30 or 50. This highlights a critical trade-off in expedited development: post-authorization surveillance becomes essential to catch rare adverse events not detected in trials.
For practical implementation, storage and distribution present unique challenges. Pfizer’s vaccine requires ultra-cold storage (-70°C), necessitating specialized freezers or dry ice shipments, while Moderna’s can be stored at -20°C, and AstraZeneca’s at standard refrigerator temperatures. These differences influence which vaccines are deployed in rural areas or low-income countries. Additionally, public health officials must prioritize dosing schedules—whether to delay second doses to maximize first-dose coverage or adhere strictly to clinical trial intervals remains a debated strategy, with countries like the UK and Canada opting for extended intervals.
In conclusion, the COVID-19 vaccine timeline is unprecedented but not reckless. It leverages pre-existing research, innovative platforms, and adaptive regulatory frameworks. Practical considerations, from dosage to distribution, shape real-world effectiveness. As more vaccines receive authorization, understanding these nuances will help policymakers and individuals make informed decisions, balancing urgency with safety.
Reporting Vaccine Reactions: A Step-by-Step Guide to Using VAERS
You may want to see also
Explore related products






![]()
Challenges in achieving herd immunity
Achieving herd immunity against COVID-19 hinges on vaccinating a critical mass of the population, typically estimated at 70-90%. However, this goal faces significant challenges beyond vaccine development. One major obstacle is vaccine hesitancy, fueled by misinformation and mistrust in scientific institutions. Surveys show that up to 20% of people in some countries remain skeptical about COVID-19 vaccines, citing concerns over safety, efficacy, or conspiracy theories. Without widespread acceptance, even the most effective vaccine cannot achieve herd immunity. Public health campaigns must address these concerns transparently, leveraging trusted community leaders and clear, evidence-based messaging to build confidence.
Another challenge lies in the logistical complexities of global vaccine distribution. While high-income countries have secured billions of doses, low-income nations struggle to access even a fraction of what’s needed. The COVAX initiative aims to bridge this gap, but supply chain issues, storage requirements (e.g., mRNA vaccines needing ultra-cold temperatures), and funding shortfalls hinder progress. For instance, the Pfizer-BioNTech vaccine requires storage at -70°C, a logistical nightmare in regions with limited infrastructure. Without equitable distribution, herd immunity remains a distant goal, as the virus continues to circulate and mutate in underserved populations.
The emergence of new variants further complicates herd immunity efforts. Variants like Delta and Omicron have demonstrated increased transmissibility and potential immune evasion, reducing vaccine effectiveness. Studies suggest that while vaccines still prevent severe illness and death, their ability to block transmission may wane over time, particularly against new strains. Booster doses, such as a third shot of mRNA vaccines, have been recommended for vulnerable populations to maintain protection. However, this raises questions about the feasibility of repeated global vaccination campaigns and the need for updated vaccines tailored to circulating variants.
Finally, achieving herd immunity requires sustained high vaccination rates across all age groups and demographics. Children, who make up a significant portion of the population, were initially excluded from vaccine trials. While vaccines are now authorized for children as young as 5 years old (with Pfizer’s 10-microgram dose for 5-11-year-olds), uptake remains slow due to parental hesitancy and logistical barriers. Similarly, elderly populations and immunocompromised individuals may not mount a robust immune response, necessitating additional strategies like monoclonal antibody treatments or stricter public health measures. Without inclusive vaccination efforts, pockets of susceptibility will persist, undermining herd immunity.
In summary, while vaccines are a cornerstone of the fight against COVID-19, achieving herd immunity demands addressing vaccine hesitancy, ensuring equitable distribution, adapting to viral evolution, and reaching diverse populations. Practical steps include investing in global vaccine infrastructure, combating misinformation through targeted education, and developing variant-specific vaccines. Only through a multifaceted approach can we hope to control the pandemic and protect communities worldwide.
Understanding Vaccine Transparency: Decoding the Immunization Schedule for All
You may want to see also
Explore related products






![]()
Efficacy of leading vaccine candidates
The race to develop a COVID-19 vaccine has yielded several leading candidates, each with distinct efficacy profiles. Pfizer-BioNTech's mRNA vaccine, for instance, demonstrated 95% efficacy in preventing symptomatic COVID-19 in clinical trials involving over 43,000 participants. This high efficacy rate is achieved through a two-dose regimen, administered 21 days apart, with optimal protection observed seven days after the second dose. The vaccine has been authorized for individuals aged 12 and older, with ongoing trials assessing its safety and efficacy in younger age groups.
In contrast, the AstraZeneca-Oxford vaccine employs a viral vector platform, showing an average efficacy of 70% across different dosing regimens. Interestingly, a subgroup analysis revealed that a lower initial dose followed by a standard second dose 8–12 weeks later resulted in 90% efficacy, compared to 62% with two standard doses. This finding highlights the importance of dosing strategies in optimizing vaccine efficacy. The AstraZeneca vaccine is approved in many countries for adults, with some nations recommending it primarily for older age groups due to rare blood clot concerns in younger individuals.
Moderna's mRNA-1273 vaccine closely follows Pfizer's in terms of efficacy, with 94.1% effectiveness in preventing symptomatic COVID-19. Its two-dose schedule is administered 28 days apart, and it has been authorized for individuals aged 18 and older. One notable advantage of Moderna's vaccine is its storage requirements: it remains stable at standard refrigerator temperatures for up to 30 days, easing distribution challenges compared to Pfizer's ultra-cold storage needs.
Johnson & Johnson's single-dose adenovirus-based vaccine offers a unique approach, with 66% global efficacy against moderate to severe COVID-19 and 85% efficacy against severe disease. Its single-dose regimen simplifies administration, making it particularly valuable in resource-limited settings or for individuals who may struggle to return for a second dose. The vaccine is authorized for adults aged 18 and older, providing a practical alternative to two-dose regimens.
Comparatively, these leading candidates showcase diverse technologies and efficacy profiles, each addressing specific logistical and immunological needs. While mRNA vaccines (Pfizer and Moderna) boast higher efficacy rates, viral vector vaccines (AstraZeneca and Johnson & Johnson) offer advantages in dosing flexibility and storage. When selecting a vaccine, factors such as age, comorbidities, and local availability should guide decision-making. For instance, younger individuals without contraindications may opt for mRNA vaccines, while those prioritizing convenience might choose Johnson & Johnson’s single-dose option. Understanding these nuances ensures informed choices in the global vaccination effort.
Vaccine Benefits: Protecting Health, Saving Lives, and Ending Pandemics
You may want to see also
Explore related products






![]()
Distribution and accessibility issues
The global rollout of COVID-19 vaccines has been a monumental task, but the success of this endeavor hinges on more than just production capacity. Distribution and accessibility issues present a complex web of challenges that threaten to undermine the entire vaccination effort. One of the most pressing concerns is the cold chain requirement for many vaccines, particularly mRNA-based ones like Pfizer-BioNTech, which necessitates storage at ultra-low temperatures (-70°C). This poses significant logistical hurdles, especially in low-resource settings where such infrastructure is limited or non-existent. For instance, in rural areas of sub-Saharan Africa, maintaining this cold chain from manufacturing plants to remote villages is a herculean task, often requiring specialized equipment and trained personnel.
Consider the Pfizer-BioNTech vaccine, which initially required two doses administered 21 days apart, with a recommended storage temperature of -70°C. This stringent requirement led to early distribution bottlenecks, as many countries lacked the necessary ultra-cold freezers. In contrast, the Oxford-AstraZeneca vaccine, which can be stored at standard refrigerator temperatures (2-8°C), offered a more feasible solution for widespread distribution, particularly in developing nations. However, this vaccine faced its own set of challenges, including dosage interval adjustments and rare side effects, highlighting the trade-offs in vaccine accessibility.
Another critical issue is equitable distribution across countries. Wealthier nations have secured a disproportionate share of vaccine doses through advance purchase agreements, leaving low- and middle-income countries at a disadvantage. For example, as of early 2021, Canada had procured enough doses to vaccinate its population five times over, while many African countries struggled to secure even a single dose per capita. Initiatives like COVAX, a global vaccine-sharing program, aim to address this disparity, but they face funding shortfalls and logistical challenges. A persuasive argument can be made for wealthy nations to donate surplus doses and invest in global vaccine equity, not only as a moral imperative but also to prevent the emergence of new variants that could prolong the pandemic.
Practical tips for improving accessibility include decentralized vaccination sites, mobile clinics, and community-based outreach programs. For instance, in India, the government partnered with local NGOs to set up vaccination camps in rural areas, ensuring that elderly and immobile individuals could receive their doses without traveling long distances. Additionally, clear communication about vaccine availability, eligibility criteria (e.g., age groups, priority populations), and appointment scheduling is crucial. In the U.S., platforms like VaccineFinder and state-specific registration portals streamlined the process, though disparities in digital literacy and internet access still left some communities behind.
Ultimately, addressing distribution and accessibility issues requires a multifaceted approach that combines technological innovation, global cooperation, and localized solutions. While the development of vaccines was a scientific triumph, their successful deployment depends on overcoming these logistical and equity challenges. Without concerted efforts to ensure fair and efficient distribution, the promise of a coronavirus vaccine risks remaining out of reach for millions, prolonging the pandemic’s impact on global health and economies.
Is Hepatitis B Vaccine Mandatory for Newborns in California?
You may want to see also
Explore related products



$15.99



![]()
Potential long-term side effects
The rapid development and deployment of COVID-19 vaccines have raised questions about their long-term safety, a concern that persists despite extensive clinical trials and ongoing surveillance. While short-term side effects like fatigue, fever, and injection site pain are well-documented, the potential for rare or delayed adverse reactions remains a critical area of study. For instance, the mRNA vaccines (Pfizer-BioNTech and Moderna) and viral vector vaccines (AstraZeneca and Johnson & Johnson) have been linked to rare cases of myocarditis and thrombosis with thrombocytopenia syndrome (TTS), respectively. These instances, though infrequent, underscore the need for continued monitoring to understand their long-term implications.
Consider the case of myocarditis, an inflammation of the heart muscle, which has been observed primarily in young males after the second dose of mRNA vaccines. While most cases resolve with rest and treatment, the long-term cardiac health of affected individuals remains under investigation. Similarly, TTS, associated with the AstraZeneca and Johnson & Johnson vaccines, has raised concerns about clotting disorders. These examples highlight the importance of age-specific risk assessments and personalized vaccination strategies. For younger populations, particularly adolescents and young adults, healthcare providers must weigh the benefits of vaccination against the rare but serious risks of these side effects.
To mitigate potential long-term side effects, individuals should adhere to post-vaccination monitoring guidelines. For those experiencing persistent symptoms like chest pain, shortness of breath, or unusual bruising after vaccination, immediate medical consultation is essential. Additionally, maintaining a health journal to track symptoms and sharing this information with healthcare providers can aid in early detection and management of adverse reactions. Public health agencies, such as the CDC and WHO, recommend reporting any severe or unexpected side effects through established vaccine safety monitoring systems, ensuring that data collection remains robust and responsive.
Comparatively, the long-term side effects of COVID-19 vaccines must be contextualized against the risks of the disease itself. Long COVID, characterized by symptoms like fatigue, cognitive dysfunction, and respiratory issues, affects a significant portion of infected individuals, often persisting for months. The vaccines, while not without risks, have demonstrably reduced severe illness, hospitalization, and death. This comparative analysis reinforces the net benefit of vaccination, even as research into rare side effects continues.
In conclusion, while the potential long-term side effects of COVID-19 vaccines warrant attention, they should not overshadow the vaccines' proven efficacy in preventing severe disease. Ongoing research, transparent communication, and individualized risk assessment are key to addressing public concerns. By staying informed and proactive, individuals can make educated decisions about vaccination, balancing protection against both the virus and its preventive measures.
Quarantined Ship Vaccine Supply: Origins and Distribution Explained
You may want to see also
Frequently asked questions
Developing a coronavirus vaccine is realistic, but the timeline is accelerated compared to traditional vaccines. While typical vaccine development takes 10+ years, COVID-19 vaccines were developed in under a year due to global collaboration, funding, and existing research on coronaviruses. Safety and efficacy were not compromised, as rigorous testing and regulatory approvals were maintained.
It is realistic to expect a coronavirus vaccine to provide immunity, though the duration varies. Vaccines like Pfizer and Moderna have shown high efficacy in preventing severe disease and hospitalization. Booster shots may be needed to maintain protection, especially against variants, but ongoing research is refining vaccine strategies for long-term immunity.
It is realistic that coronavirus vaccines will remain effective against many variants, but their efficacy may vary. Current vaccines still protect against severe illness and death from most variants, including Delta and Omicron. Vaccine manufacturers are developing updated formulations to target specific variants, ensuring continued effectiveness.
Achieving global vaccination coverage is realistic but challenging. Wealthy nations have higher vaccination rates, while low-income countries face supply and distribution hurdles. Initiatives like COVAX aim to bridge this gap. With continued efforts, equitable global vaccination is possible, though it requires international cooperation and resource allocation.
It is not realistic to expect a coronavirus vaccine to completely eradicate the virus. While vaccines significantly reduce transmission and severity, SARS-CoV-2 is likely to become endemic, meaning it will continue to circulate at lower levels. Vaccines, along with public health measures, will help manage the virus rather than eliminate it entirely.







![PANDEMIC [Blu-ray]](https://m.media-amazon.com/images/I/71xlZkgPU4L._AC_UL320_.jpg)
![Pandemic [DVD]](https://m.media-amazon.com/images/I/51vChb09XaL._AC_UL320_.jpg)

![Pandemic [DVD]](https://m.media-amazon.com/images/I/91ynbSGeZVS._AC_UL320_.jpg)


![Pandemic [DVD]](https://m.media-amazon.com/images/I/81G1z+AOoNL._AC_UL320_.jpg)