The rotavirus vaccine, a pivotal tool in preventing severe diarrhea and dehydration in infants and young children, has been a cornerstone of pediatric immunization since its introduction. Developed in response to the global burden of rotavirus infections, which historically caused hundreds of thousands of deaths annually, the vaccine first became available in the early 2000s. The initial rotavirus vaccine, RotaShield, was licensed in 1998 but was later withdrawn due to safety concerns. Its successors, RotaTeq (approved in 2006) and Rotarix (approved in 2008), have since been widely adopted and are now included in routine childhood vaccination schedules in many countries. These vaccines have significantly reduced rotavirus-related hospitalizations and mortality, marking a major public health achievement. As of now, the rotavirus vaccine has been in use for over two decades, continually evolving to improve safety and efficacy.
Explore related products

$9.99 $9.99





What You'll Learn
- Vaccine Development Timeline: When was the rotavirus vaccine first created and approved for use
- Age Recommendations: What ages are targeted for rotavirus vaccine administration globally
- Historical Impact: How has the vaccine reduced rotavirus cases since introduction
- Global Rollout: When did different countries start implementing the rotavirus vaccine
- Vaccine Updates: Have there been newer versions or updates to the rotavirus vaccine
![]()
Vaccine Development Timeline: When was the rotavirus vaccine first created and approved for use?
The rotavirus vaccine's journey from concept to approval is a testament to the power of scientific perseverance. The virus, a leading cause of severe diarrhea in infants and young children, was first identified in the 1970s. However, it wasn't until the 1980s that researchers began developing a vaccine. The initial attempts faced significant challenges, including safety concerns and limited efficacy. Despite these setbacks, the scientific community remained committed to finding a solution, driven by the urgent need to reduce the global burden of rotavirus-related hospitalizations and deaths.
One of the earliest milestones in rotavirus vaccine development was the creation of the first candidate vaccines in the late 1980s and early 1990s. These early vaccines, such as Rotashield (RotaShield), were designed to mimic natural infection and stimulate immunity. Rotashield was approved by the U.S. Food and Drug Administration (FDA) in 1998 for infants aged 2 months and older, administered in three oral doses at 2, 4, and 6 months of age. However, its success was short-lived. Post-approval surveillance revealed a rare but serious side effect: intussusception, a type of bowel obstruction. This led to the vaccine's withdrawal in 1999, underscoring the critical importance of rigorous safety monitoring in vaccine development.
The setback with Rotashield prompted a reevaluation of rotavirus vaccine strategies, leading to the development of safer and more effective alternatives. By the mid-2000s, two new vaccines emerged: RotaTeq (Rotateq) and Rotarix (Rotarix). RotaTeq, a pentavalent vaccine targeting five common rotavirus strains, was approved by the FDA in 2006 for infants aged 6–32 weeks. It is administered in three oral doses at 2, 4, and 6 months. Rotarix, a monovalent vaccine, received FDA approval in 2008 for infants aged 6 weeks to 24 weeks, given in two or three doses depending on the country’s immunization schedule. Both vaccines demonstrated high efficacy and a significantly lower risk of intussusception compared to their predecessor.
The approval of these vaccines marked a turning point in the fight against rotavirus. Their introduction into national immunization programs worldwide has led to dramatic reductions in rotavirus-related hospitalizations and deaths. For instance, in countries with high vaccination coverage, rotavirus hospitalizations have decreased by 80–90%. This success highlights the importance of continued investment in vaccine research and development, as well as global collaboration to ensure equitable access to life-saving vaccines.
For parents and caregivers, understanding the rotavirus vaccine’s timeline and its practical implications is crucial. The vaccine is typically administered orally, making it easy to include in routine immunization schedules. It is most effective when given at the recommended ages, as delaying doses can reduce immunity. Side effects are generally mild and may include temporary diarrhea or irritability. By staying informed and adhering to vaccination guidelines, families can protect their children from this preventable yet potentially severe disease. The rotavirus vaccine’s history serves as a reminder of the challenges and triumphs in medical science, ultimately saving lives through innovation and persistence.
Effective Tips to Ease Discomfort After Getting Vaccinated
You may want to see also
Explore related products

$11.93 $21.99





![]()
Age Recommendations: What ages are targeted for rotavirus vaccine administration globally?
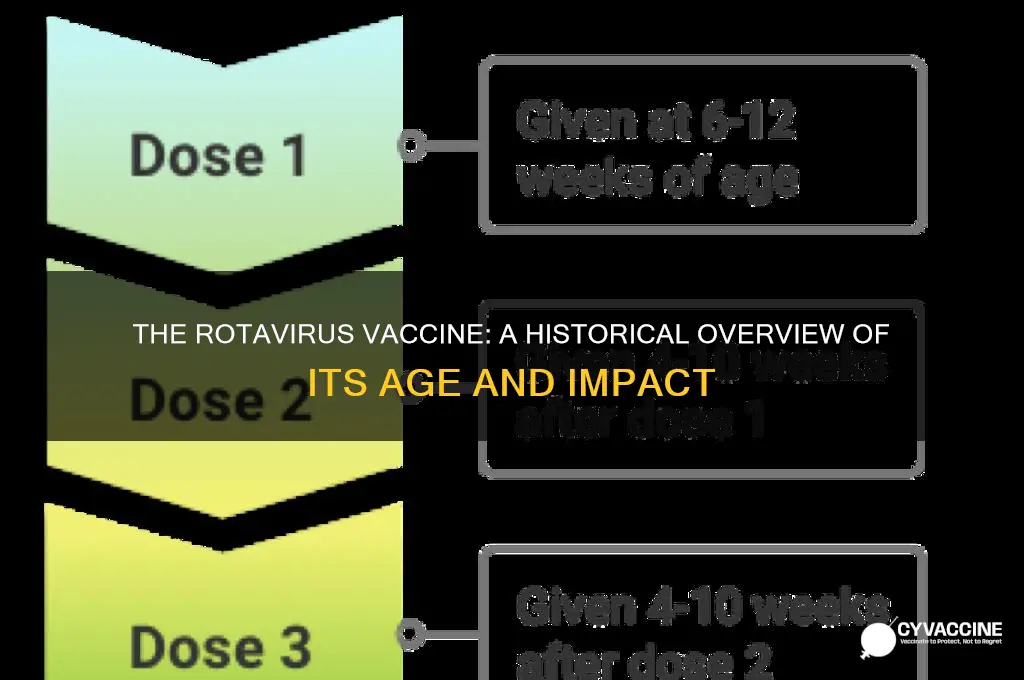
The rotavirus vaccine is typically administered to infants, with global health organizations emphasizing the importance of timely vaccination to maximize protection against severe rotavirus gastroenteritis. The World Health Organization (WHO) recommends that the first dose be given at 6–15 weeks of age, depending on the specific vaccine and national immunization schedules. This early intervention is critical because infants are most vulnerable to rotavirus infection during their first year of life, and delaying vaccination reduces its effectiveness. For example, the RotaTeq® vaccine is administered in a 3-dose series at 2, 4, and 6 months of age, while Rotarix® follows a 2-dose schedule at 2 and 4 months. Adhering to these timelines ensures optimal immune response and long-term protection.
Instructively, healthcare providers must consider the age limits for rotavirus vaccination, as it is not recommended for infants older than 8 months (for Rotarix®) or 32 weeks (for RotaTeq®). This restriction is due to the vaccine’s live, attenuated nature and the potential for decreased efficacy or adverse reactions in older infants. Parents and caregivers should be educated about the narrow age window for vaccination, as missed doses cannot be administered outside the approved timeframe. Practical tips include scheduling vaccinations during routine pediatric visits and ensuring caregivers are aware of the vaccine’s age-specific requirements to avoid delays.
Comparatively, age recommendations for rotavirus vaccination vary slightly across countries, influenced by local disease burden, healthcare infrastructure, and vaccine availability. For instance, high-income countries with lower rotavirus prevalence may prioritize earlier vaccination within the 6–12-week range, while low-income countries with higher disease burden might focus on broader age coverage up to 15 weeks. Despite these differences, the global consensus remains consistent: vaccinate infants as early as possible within the approved age range to prevent severe dehydration, hospitalizations, and deaths caused by rotavirus.
Persuasively, the age-targeted approach to rotavirus vaccination has proven highly effective in reducing global morbidity and mortality. Studies show that vaccinating infants before 15 weeks of age can reduce rotavirus-related hospitalizations by up to 90%. This success underscores the importance of strict adherence to age recommendations, as even slight delays can compromise herd immunity and increase disease transmission. Policymakers and healthcare providers must collaborate to ensure equitable access to the vaccine, particularly in regions where rotavirus remains a leading cause of childhood diarrhea.
Descriptively, the rotavirus vaccine’s age-specific administration is a cornerstone of pediatric immunization programs worldwide. Its design as an oral vaccine simplifies delivery, making it accessible even in resource-limited settings. However, the narrow age window requires meticulous planning and community engagement to ensure timely uptake. By targeting infants at 6–15 weeks of age, the vaccine not only protects individual children but also contributes to broader public health goals, reducing the socioeconomic burden of rotavirus-related illnesses on families and healthcare systems.
Vaccines: Safeguarding Vulnerable Populations Through Immunity and Community Protection
You may want to see also
Explore related products






![]()
Historical Impact: How has the vaccine reduced rotavirus cases since introduction?
The rotavirus vaccine, first introduced in the United States in 2006, has fundamentally reshaped the landscape of pediatric health by dramatically reducing the incidence of severe rotavirus gastroenteritis. Before its introduction, rotavirus was responsible for approximately 200,000 emergency room visits, 55,000 to 70,000 hospitalizations, and 20 to 60 deaths annually among U.S. children under five. The vaccine’s rollout marked a turning point, with studies showing a 75-90% reduction in rotavirus-related hospitalizations within just a few years of its implementation. This success underscores the vaccine’s role as a cornerstone of preventive medicine, offering a clear example of how targeted immunization can transform public health outcomes.
Analyzing the vaccine’s impact reveals a multi-faceted approach to disease prevention. The rotavirus vaccine is administered orally in a 2- or 3-dose series, depending on the brand (RotaTeq or Rotarix), starting at 2 months of age and completing by 8 months. Its efficacy extends beyond individual protection; herd immunity has played a significant role in reducing rotavirus circulation, even among unvaccinated populations. For instance, countries with high vaccination rates, such as the U.S. and Australia, have reported near-elimination of rotavirus as a leading cause of childhood diarrhea. This dual benefit—direct protection and community-wide reduction—highlights the vaccine’s historical significance in combating a once-ubiquitous pathogen.
A comparative perspective further illustrates the vaccine’s impact. In low-income countries, where access to the vaccine has been slower, rotavirus remains a leading cause of child mortality, with over 125,000 deaths annually. In contrast, high-income nations with robust vaccination programs have seen rotavirus-related deaths become virtually nonexistent. This disparity emphasizes the vaccine’s potential to address global health inequities, provided barriers to access are overcome. Practical steps, such as integrating the vaccine into routine immunization schedules and reducing costs, could amplify its historical impact on a global scale.
Persuasively, the rotavirus vaccine’s success serves as a model for future vaccine development and implementation. Its ability to reduce hospitalizations, healthcare costs, and mortality within a decade of introduction is unparalleled. For parents, ensuring timely vaccination is critical; delaying doses beyond the recommended age window can reduce efficacy. Healthcare providers should emphasize the vaccine’s safety profile, which includes rare but manageable side effects like mild fever or irritability. By learning from the rotavirus vaccine’s historical impact, we can advocate for similar interventions against other preventable diseases, cementing its legacy as a lifesaving innovation.
Vaccine Efficacy: Understanding Protection Against Severe Illness Post-Vaccination
You may want to see also
Explore related products




![]()
Global Rollout: When did different countries start implementing the rotavirus vaccine?
The rotavirus vaccine, a cornerstone in the fight against severe childhood diarrhea, has seen a staggered global rollout since its inception. Developed in the early 2000s, the first rotavirus vaccines, RotaShield and later RotaTeq, marked a significant milestone in pediatric health. However, their introduction into national immunization programs varied widely across countries, influenced by factors such as economic status, disease burden, and policy priorities. Understanding this timeline offers insights into global health disparities and the challenges of vaccine accessibility.
High-income countries led the charge, with the United States and Australia among the first to implement rotavirus vaccination in 2006. The U.S. Centers for Disease Control and Prevention (CDC) recommended a 3-dose schedule of RotaTeq for infants at 2, 4, and 6 months of age, while Australia opted for a 2-dose regimen of Rotarix at 2 and 4 months. These early adopters saw dramatic reductions in rotavirus-related hospitalizations, setting a precedent for other nations. For instance, the U.S. reported a 90% decline in severe rotavirus cases within a decade of vaccine introduction.
Middle-income countries followed suit, albeit with delays. Brazil and Mexico introduced the rotavirus vaccine in 2006 and 2007, respectively, leveraging their robust public health infrastructures. Brazil’s program, which included a 2-dose schedule of Rotarix, achieved over 80% coverage within the first year, showcasing the feasibility of rapid scale-up in resource-constrained settings. In contrast, India, despite a high burden of rotavirus disease, only introduced the vaccine in 2016 as part of its Universal Immunization Programme, highlighting the challenges of affordability and logistical coordination in large, diverse populations.
Low-income countries faced the greatest barriers to implementation. Gavi, the Vaccine Alliance, played a pivotal role in accelerating access by subsidizing vaccine costs for eligible nations. Countries like Ghana and Rwanda introduced the rotavirus vaccine in 2012 and 2014, respectively, through Gavi support. However, coverage remains uneven, with many African nations still struggling to reach WHO’s target of 90% immunization. Practical challenges, such as cold chain maintenance and community hesitancy, underscore the need for tailored strategies in these settings.
The global rollout of the rotavirus vaccine reflects both progress and persistent inequities in health systems. While high- and middle-income countries have largely reaped the benefits, low-income nations continue to grapple with implementation hurdles. Policymakers and health advocates must prioritize sustainable solutions, such as local vaccine production and community engagement, to ensure that all children, regardless of geography, are protected from this preventable disease. The rotavirus vaccine’s journey serves as a reminder that innovation alone is insufficient—equitable access is the ultimate measure of success.
Why Relying Solely on a Vaccine Could Be Risky
You may want to see also
![]()
Vaccine Updates: Have there been newer versions or updates to the rotavirus vaccine?
The rotavirus vaccine has been a cornerstone of pediatric immunization since its introduction in the early 2000s, significantly reducing hospitalizations and deaths from severe diarrhea in children. However, like many vaccines, it has evolved over time to address emerging strains and improve efficacy. One notable update came in 2008 with the introduction of the RotaTeq vaccine, a pentavalent formulation designed to protect against five common rotavirus strains. This was followed by Rotarix, a monovalent vaccine approved in 2008, which targets the most prevalent G1P[8] strain globally. These advancements marked a shift toward broader protection, ensuring the vaccine remained effective against circulating strains.
Analyzing the latest developments, the World Health Organization (WHO) has emphasized the importance of strain-specific updates to address regional variations in rotavirus prevalence. For instance, in some low-income countries, the P[6] strain has emerged as a significant cause of rotavirus gastroenteritis, prompting research into vaccines that cover this strain. Additionally, efforts are underway to develop heat-stable formulations, which would eliminate the need for strict cold chain storage—a critical barrier in resource-limited settings. These innovations aim to enhance accessibility and ensure the vaccine’s effectiveness in diverse environments.
From a practical standpoint, parents and healthcare providers should be aware of the recommended dosing schedules for the current rotavirus vaccines. RotaTeq is administered in three doses at 2, 4, and 6 months of age, while Rotarix requires only two doses at 2 and 4 months. It’s crucial to adhere to these schedules, as deviations can reduce the vaccine’s protective efficacy. Additionally, the vaccine is given orally, making it easier to administer compared to injectable vaccines. However, caregivers should avoid feeding infants for at least 30 minutes after vaccination to ensure the vaccine is not expelled.
Comparatively, newer versions of the rotavirus vaccine are not just about adding strains but also improving safety profiles. Early versions, such as RotaShield (withdrawn in 1999), were associated with a rare but serious side effect called intussusception. Modern vaccines like RotaTeq and Rotarix have significantly lower risks, with studies showing a small increase in intussusception cases (1-5 additional cases per 100,000 vaccinated infants). This underscores the balance between maximizing protection and minimizing adverse effects, a key consideration in vaccine updates.
Looking ahead, the pipeline for rotavirus vaccines includes next-generation candidates like the RV3-BB vaccine, which is currently in clinical trials. This vaccine is designed to be more affordable and easier to produce, potentially expanding access in low- and middle-income countries. Another promising development is the exploration of combination vaccines, which could protect against rotavirus alongside other pathogens like norovirus. These advancements highlight the ongoing commitment to refining the rotavirus vaccine, ensuring it remains a vital tool in global health.
Protecting Your Child: The Meningitis B Vaccine Decision Explained
You may want to see also
Frequently asked questions
The first rotavirus vaccine was licensed for use in the United States in 1998, but it was withdrawn in 1999 due to safety concerns. The currently used rotavirus vaccines, RotaTeq and Rotarix, were introduced in 2006.
The development of the rotavirus vaccine began in the 1980s, with the first vaccine (RotaShield) approved in 1998. However, it was later withdrawn, and safer versions were developed and introduced in the mid-2000s.
The current rotavirus vaccines, RotaTeq and Rotarix, have been in use globally since 2006, with widespread adoption in many countries as part of routine childhood immunization programs.