The monkeypox vaccine, originally developed to combat smallpox, has a history dating back to the mid-20th century. The most well-known vaccine, MVA-BN (also known as Jynneos or Imvamune), was first approved for use against smallpox in 2013 and later repurposed for monkeypox due to the viruses' close genetic relationship. Another vaccine, ACAM2000, a second-generation smallpox vaccine, has also been used off-label for monkeypox but is associated with more side effects. The age of these vaccines highlights their long-standing role in public health, with ongoing research and adaptations to address emerging diseases like the 2022 monkeypox outbreak.
| Characteristics | Values |
|---|---|
| Vaccine Name | JYNNEOS (also known as Imvamune or Imvanex) |
| Development Year | Originally developed in the 1980s as a smallpox vaccine |
| Approval for Monkeypox | Approved by the FDA in 2019 for prevention of smallpox and monkeypox |
| Vaccine Type | Live, non-replicating virus (modified vaccinia Ankara - MVA) |
| Target Population | Individuals at high risk of exposure to orthopoxviruses, including monkeypox |
| Age Approval | Approved for individuals 18 years and older (some off-label use in younger populations under specific circumstances) |
| Dosage Regimen | Two doses administered subcutaneously, 4 weeks apart |
| Efficacy Against Monkeypox | High efficacy based on animal studies and inferred from smallpox protection; limited human data specific to monkeypox |
| Storage Requirements | Stored frozen (-15°C to -25°C) until ready for use, then refrigerated (2°C to 8°C) for up to 8 weeks |
| Side Effects | Generally mild, including pain at injection site, fatigue, headache, and muscle pain |
| Manufacturer | Bavarian Nordic |
| Availability | Limited global supply, prioritized for outbreak response and high-risk groups |
| Historical Context | Developed as a safer alternative to older smallpox vaccines due to reduced side effects |
Explore related products






What You'll Learn
- Origins of the Vaccine: Developed in 1980s, based on smallpox vaccine research
- First Approval: Licensed in 2019 for smallpox, later used for monkeypox
- Vaccine Type: Third-generation, non-replicating vaccinia virus (MVA-BN)
- Initial Use: Primarily for smallpox eradication campaigns globally
- Monkeypox Application: Adopted for monkeypox in 2022 outbreaks
![]()
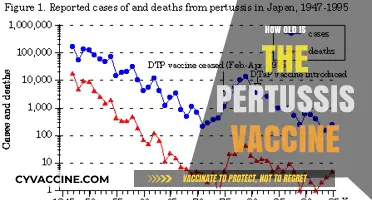
Origins of the Vaccine: Developed in 1980s, based on smallpox vaccine research
The monkeypox vaccine, though not widely recognized until recent outbreaks, traces its roots to the 1980s, emerging from decades of smallpox vaccine research. Developed during a period of heightened concern over bioterrorism and the potential re-emergence of smallpox, the vaccine was initially designed as a countermeasure against orthopoxviruses, a family that includes both smallpox and monkeypox. This strategic repurposing of existing knowledge allowed scientists to leverage the smallpox vaccine’s proven efficacy, adapting it to address the less severe but still concerning monkeypox virus.
Analytically, the 1980s development of the monkeypox vaccine exemplifies the principle of scientific foresight. Researchers recognized that the attenuated vaccinia virus used in the smallpox vaccine (e.g., ACAM2000) could cross-protect against related orthopoxviruses. This insight was validated by animal studies, which demonstrated efficacy against monkeypox in non-human primates. However, human trials were limited due to ethical considerations and the rarity of monkeypox cases at the time. The vaccine’s shelf life, typically 5–10 years when stored at 2–8°C, ensured its availability for future outbreaks, though it remained largely unused until the 2003 U.S. outbreak and subsequent global cases.
Instructively, the vaccine’s administration follows a specific protocol: a single dose of 0.5 mL is administered via subcutaneous injection, preferably in the deltoid muscle for adults. For children aged 1–12, the dose is reduced to 0.1 mL, given intradermally. A key caution is the vaccine’s live virus component, which contraindicates its use in immunocompromised individuals, pregnant women, and those with certain skin conditions like eczema. Adverse effects, such as fever, fatigue, and injection site reactions, are generally mild but require monitoring.
Persuasively, the 1980s-developed vaccine underscores the value of investing in broad-spectrum solutions. By building on smallpox research, scientists created a tool that could address multiple threats, a strategy increasingly relevant in today’s interconnected world. The recent approval of third-generation vaccines like JYNNEOS (also known as Imvamune or Imvanex) further highlights this legacy, offering a safer, non-replicating alternative for broader populations, including at-risk groups.
Comparatively, while the 1980s vaccine shares its origins with smallpox immunization, its application differs significantly. Smallpox eradication campaigns involved mass vaccination, whereas monkeypox vaccination has been targeted, focusing on high-risk groups like healthcare workers and those exposed to infected individuals. This tailored approach reflects evolving public health strategies, balancing efficacy with safety and resource allocation. Practically, individuals should consult healthcare providers to determine eligibility and follow post-vaccination guidelines, such as avoiding contact with immunocompromised persons until the injection site heals.
Measles Vaccination: Understanding the Required Shots for Full Protection
You may want to see also
Explore related products






![]()
First Approval: Licensed in 2019 for smallpox, later used for monkeypox
The monkeypox vaccine's origins trace back to its initial approval for a different virus altogether. In 2019, the U.S. Food and Drug Administration (FDA) licensed the JYNNEOS vaccine (also known as Imvamune or Imvanex) for the prevention of smallpox in individuals 18 years of age and older. This marked a significant milestone, as smallpox had been eradicated globally since 1980, and the vaccine was primarily stockpiled for emergency use in case of bioterrorism threats. JYNNEOS, a live, non-replicating vaccine derived from the Modified Vaccinia Ankara (MVA) virus, offered a safer alternative to older smallpox vaccines, which could cause severe side effects in certain populations, such as those with weakened immune systems.
The vaccine’s journey from smallpox to monkeypox began during the 2022 monkeypox outbreak, when health authorities recognized its potential cross-protection. Unlike the smallpox virus, monkeypox is caused by a related orthopoxvirus, and studies had already demonstrated JYNNEOS’s efficacy against monkeypox in animal models. In response to the outbreak, the FDA granted emergency use authorization (EUA) for JYNNEOS to prevent monkeypox in adults and children under 18 years old, administered as a two-dose series 28 days apart. Each dose contains 0.5 mL of the vaccine, delivered subcutaneously (just under the skin), typically in the upper arm.
From a practical standpoint, the repurposing of JYNNEOS highlights the adaptability of vaccine development in the face of emerging threats. Its approval for monkeypox was expedited due to its established safety profile and the urgent need for a countermeasure. However, its use is not without considerations. While generally well-tolerated, common side effects include pain at the injection site, fatigue, headache, and muscle pain. It is not recommended for individuals with severe allergies to any of its components, and pregnant or breastfeeding individuals should consult their healthcare provider before vaccination.
Comparatively, JYNNEOS stands apart from older smallpox vaccines like ACAM2000, which uses a live replicating virus and carries risks such as myocarditis and skin infections. This makes JYNNEOS a preferred option for broader populations, including immunocompromised individuals and those with skin conditions like eczema. Its deployment during the monkeypox outbreak underscores the importance of maintaining a robust vaccine stockpile and investing in research that allows for rapid repurposing of existing tools.
In conclusion, the monkeypox vaccine’s roots in smallpox prevention demonstrate the value of forward-thinking public health strategies. Licensed in 2019, JYNNEOS’s transition to monkeypox use in 2022 exemplifies how scientific preparedness can save lives during unexpected outbreaks. For those eligible, following the recommended two-dose regimen and staying informed about potential side effects ensures optimal protection. This vaccine’s story serves as a reminder that today’s investments in medical innovation can become tomorrow’s critical defenses.
Skipping Cat Vaccines: Risks, Consequences, and Why They're Essential
You may want to see also
Explore related products


$12.33 $30




![]()
Vaccine Type: Third-generation, non-replicating vaccinia virus (MVA-BN)
The third-generation, non-replicating vaccinia virus vaccine, known as MVA-BN (Modified Vaccinia Ankara - Bavarian Nordic), represents a significant advancement in smallpox and monkeypox prevention. Developed in the early 2000s, this vaccine emerged as a safer alternative to earlier replicative vaccinia-based vaccines, which often caused severe side effects, particularly in immunocompromised individuals. MVA-BN is a highly attenuated virus that cannot replicate in human cells, making it suitable for a broader population, including those with weakened immune systems. Its approval for medical use began in 2013 in Canada and later expanded to other countries, including the European Union and the United States, primarily for smallpox but also as a critical tool against monkeypox outbreaks.
From a practical standpoint, MVA-BN is administered in a two-dose regimen, typically given 28 days apart. Each dose is 0.5 mL, delivered subcutaneously, preferably in the deltoid region of the arm. It is approved for individuals aged 18 and older, though off-label use in younger populations has been considered during severe outbreaks. Unlike earlier vaccines, MVA-BN does not leave a scar at the injection site, a hallmark of older smallpox vaccines. Recipients should be monitored for 15 minutes post-injection for immediate adverse reactions, which are rare but can include mild symptoms like fatigue, headache, or injection site pain.
Comparatively, MVA-BN stands out for its safety profile. First-generation vaccines, such as Dryvax, were associated with serious complications like myopericarditis and progressive vaccinia, particularly in those with HIV or eczema. Second-generation vaccines, like ACAM2000, improved safety but still posed risks due to their replicative nature. MVA-BN eliminates these concerns by using a non-replicating virus, making it the preferred choice for modern immunization campaigns. Its efficacy against monkeypox, while not initially its primary target, has been demonstrated in recent outbreaks, with studies showing a significant reduction in disease severity and transmission.
For those considering MVA-BN, it’s essential to understand its limitations. While highly effective, it is not 100% protective, and breakthrough infections, though rare, can occur. Additionally, the vaccine’s availability remains limited in many regions, often prioritized for high-risk groups like healthcare workers and close contacts of confirmed cases. Storage requirements are less stringent than some other vaccines, as MVA-BN remains stable at standard refrigerator temperatures (2–8°C), facilitating distribution in resource-limited settings.
In conclusion, MVA-BN exemplifies the evolution of vaccine technology, offering a safer, more inclusive solution for smallpox and monkeypox prevention. Its development underscores the importance of innovation in addressing emerging and re-emerging infectious diseases. As monkeypox continues to pose global health challenges, MVA-BN remains a cornerstone of response strategies, balancing efficacy, safety, and accessibility in ways its predecessors could not.
Polio's Grip: Pre-Vaccine America's Battle with the Crippling Disease
You may want to see also
Explore related products





![]()
Initial Use: Primarily for smallpox eradication campaigns globally
The origins of the monkeypox vaccine are deeply intertwined with the global campaign to eradicate smallpox, a devastating disease that plagued humanity for centuries. Developed in the mid-20th century, the smallpox vaccine, known as Vaccinia, became the cornerstone of the World Health Organization’s (WHO) eradication efforts. This vaccine, administered via a bifurcated needle in a unique scarification method, provided cross-protection against monkeypox due to the genetic similarities between the two viruses. During this era, the vaccine was primarily targeted at high-risk populations in endemic regions, such as healthcare workers and individuals in close contact with infected patients, to create a protective barrier against smallpox outbreaks.
The global smallpox eradication campaign, which ran from 1967 to 1977, relied heavily on mass vaccination strategies. The vaccine was administered to individuals as young as 1 year old, with a standard dose of 0.0025 mL of reconstituted vaccine. The process involved piercing the skin 15 times in a small area, typically on the upper arm, to ensure a robust immune response. This method, while effective, was not without risks, including rare but serious side effects like progressive vaccinia or eczema vaccinatum. Despite these challenges, the campaign’s success led to the declaration of smallpox eradication in 1980, marking one of the greatest achievements in public health history.
During this period, the smallpox vaccine’s dual role in preventing monkeypox was largely incidental but significant. In regions where smallpox was endemic, such as parts of Africa, the vaccine inadvertently reduced monkeypox cases by providing cross-immunity. However, as smallpox vaccination campaigns ceased post-eradication, the population’s immunity to both viruses began to wane. This decline in immunity, coupled with increased human-animal interactions in endemic areas, contributed to the resurgence of monkeypox cases in subsequent decades. The initial use of the vaccine, therefore, laid the groundwork for understanding its broader applications beyond smallpox.
Practical considerations during the smallpox eradication campaigns offer valuable lessons for monkeypox vaccination today. For instance, the bifurcated needle technique, though unconventional, ensured efficient vaccine delivery with minimal training. Modern monkeypox vaccination efforts could adopt similar low-tech, high-impact strategies to maximize reach in resource-limited settings. Additionally, the historical focus on ring vaccination—targeting close contacts of infected individuals—remains a relevant approach for controlling outbreaks. By studying these early campaigns, public health officials can refine strategies to address contemporary challenges posed by monkeypox.
In conclusion, the initial use of the smallpox vaccine in global eradication campaigns not only eliminated smallpox but also provided a foundation for combating monkeypox. Its legacy underscores the importance of vaccination as a public health tool and highlights the need for sustained efforts to maintain immunity against re-emerging threats. As monkeypox continues to spread globally, revisiting these historical strategies can inform more effective and equitable vaccination programs.
VA Shingrix Vaccine Availability: What Veterans Need to Know
You may want to see also
Explore related products






![]()
Monkeypox Application: Adopted for monkeypox in 2022 outbreaks
The monkeypox vaccine, originally developed for smallpox, has been a critical tool in the fight against the 2022 monkeypox outbreaks. While the vaccine itself is not new, its application for monkeypox is a recent development, highlighting the adaptability of medical science in response to emerging threats. The vaccine, known as MVA-BN (modified vaccinia Ankara-Bavarian Nordic), was first approved for smallpox in 2013 but gained prominence in 2022 as a strategic intervention for monkeypox due to the viruses' close genetic relationship. This repurposing underscores the importance of existing medical resources in addressing new public health challenges.
From a practical standpoint, the monkeypox vaccine is administered in two doses, typically 28 days apart, for optimal immunity. The recommended dosage for individuals aged 18 and older is 0.5 mL per injection, delivered subcutaneously. For those under 18, dosage adjustments are made based on weight and age, though vaccination in this demographic is less common unless at high risk. It’s crucial to follow the vaccination schedule strictly, as incomplete dosing may compromise protection. Side effects are generally mild, including pain at the injection site, fatigue, and headache, but these are far outweighed by the vaccine’s efficacy in preventing severe disease.
The adoption of the monkeypox vaccine in 2022 was driven by the urgent need to curb the spread of the virus, particularly among high-risk populations. Public health campaigns emphasized targeted vaccination strategies, focusing on healthcare workers, close contacts of confirmed cases, and communities with higher transmission rates. This approach not only mitigated the outbreak’s impact but also demonstrated the value of rapid, data-driven decision-making in public health. The vaccine’s dual-purpose use for both smallpox and monkeypox serves as a testament to the foresight of vaccine development and the importance of maintaining a robust medical arsenal.
Comparatively, the monkeypox vaccine’s deployment differs from that of COVID-19 vaccines in terms of scale and distribution. While COVID-19 vaccines were rolled out globally to billions, monkeypox vaccination efforts have been more localized and targeted, reflecting the diseases' differing transmission dynamics and risk profiles. This tailored approach ensures that resources are allocated efficiently, maximizing impact where the need is greatest. Additionally, the monkeypox vaccine’s long history of safety data from smallpox eradication efforts provided a head start in building public trust, a critical factor in any vaccination campaign.
In conclusion, the 2022 monkeypox outbreaks marked a pivotal moment in the application of the monkeypox vaccine, transforming it from a smallpox-specific tool into a versatile defense against a related virus. Its adoption highlights the importance of vaccine adaptability, strategic distribution, and evidence-based public health responses. For individuals, understanding the vaccine’s dosage, administration, and benefits is key to making informed decisions. As the medical community continues to monitor and respond to emerging threats, the monkeypox vaccine stands as a prime example of how preparedness and innovation can save lives.
Pfizer Vaccine Results: Why Experts Are Cautiously Optimistic
You may want to see also
Frequently asked questions
The monkeypox vaccine, specifically the JYNNEOS (also known as Imvamune or Imvanex) vaccine, was first approved for use in the United States in 2019. However, earlier versions of smallpox vaccines, which also provide cross-protection against monkeypox, have been in use since the mid-20th century.
The first vaccines effective against monkeypox were smallpox vaccines, which date back to the late 1700s. The modern monkeypox-specific vaccine, JYNNEOS, was developed in the early 21st century and approved in 2019.
The monkeypox vaccine (JYNNEOS) is not the same as the older smallpox vaccines but is derived from a similar virus. It is a newer, safer alternative specifically designed to protect against both smallpox and monkeypox.
The JYNNEOS vaccine has been in use globally since its approval in 2019, primarily for at-risk populations. Its use expanded significantly during the 2022 monkeypox outbreak.
Older smallpox vaccines, such as ACAM2000, are still used in some cases for monkeypox prevention, but they are less commonly used due to potential side effects. The newer JYNNEOS vaccine is preferred for its safety profile.