The Hib vaccine, which protects against Haemophilus influenzae type b (Hib), a bacterium that can cause severe infections such as meningitis and pneumonia, has been a cornerstone of pediatric immunization since its introduction in the 1980s. Developed in response to the high incidence of Hib-related diseases in young children, the vaccine first became available in the United States in 1985, with subsequent improvements leading to the creation of conjugate vaccines in the early 1990s. These advancements significantly enhanced its efficacy and safety, making it a standard component of childhood vaccination schedules worldwide. Today, the Hib vaccine stands as a testament to the power of medical innovation in reducing the burden of preventable diseases.
| Characteristics | Values |
|---|---|
| Year of Introduction | 1985 (first Hib conjugate vaccine approved in the US) |
| Target Population | Infants and young children (primarily under 5 years old) |
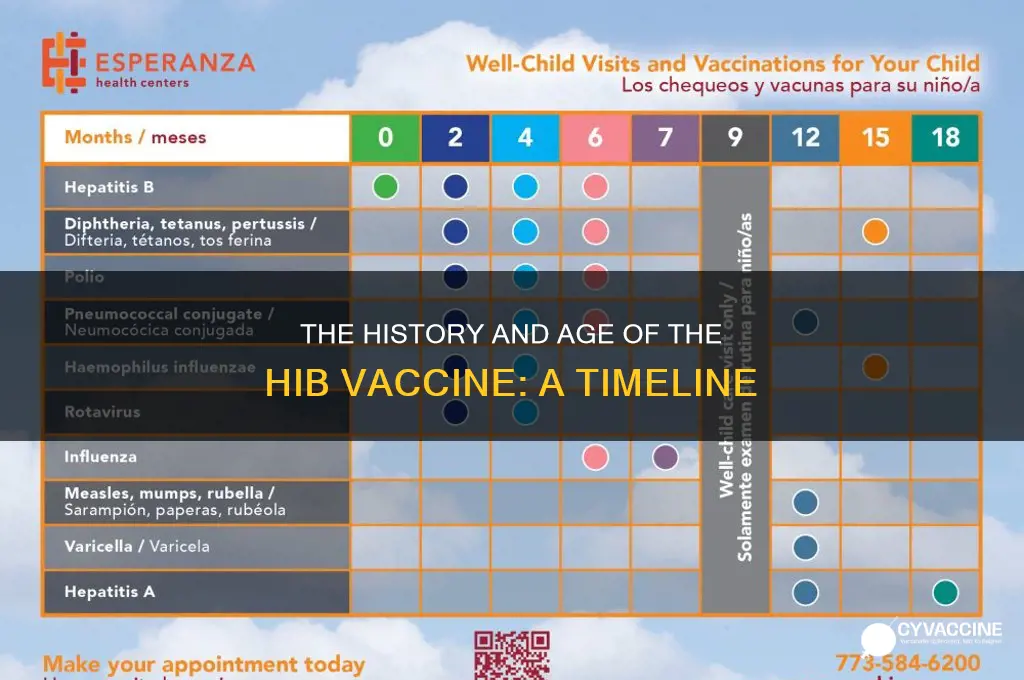
| Recommended Age for Vaccination | Typically given at 2, 4, and 6 months of age, with a booster dose at 12-15 months |
| Vaccine Types | Hib conjugate vaccines (e.g., ActHIB, PedvaxHIB, Hiberix) |
| Disease Prevented | Invasive Haemophilus influenzae type b (Hib) diseases, such as meningitis, pneumonia, and epiglottitis |
| Effectiveness | Over 95% effective in preventing invasive Hib diseases |
| Global Impact | Reduced Hib disease incidence by >90% in countries with widespread vaccination |
| Current Status | Routine immunization in many countries, included in national vaccination schedules |
| Age-Specific Considerations | Not routinely recommended for individuals over 5 years old, unless at increased risk (e.g., asplenia, HIV) |
| Last Updated Guidelines | Varies by country; follow local health authority recommendations (e.g., CDC, WHO) |
Explore related products


$11.93 $21.99




What You'll Learn
- Hib Vaccine Development Timeline: When was the Hib vaccine first created and approved for use
- Age Recommendations: What ages are recommended for Hib vaccine administration in children
- Historical Impact: How has the Hib vaccine reduced diseases like meningitis and pneumonia
- Vaccine Composition: What components make up the Hib vaccine and how do they work
- Global Availability: When did the Hib vaccine become widely accessible worldwide
![]()
Hib Vaccine Development Timeline: When was the Hib vaccine first created and approved for use?
The Hib vaccine, a cornerstone in pediatric immunization, emerged in the late 20th century as a response to the devastating impact of *Haemophilus influenzae* type b (Hib) infections. Before its development, Hib was a leading cause of bacterial meningitis and other severe illnesses in children under five, claiming hundreds of thousands of lives annually. The journey from identifying the need for a vaccine to its widespread approval is a testament to scientific perseverance and public health innovation.
The first Hib vaccine prototype was developed in the early 1970s, but it wasn’t until 1985 that a purified polysaccharide vaccine was licensed in the United States. This initial version, however, was only effective in children over two years old, leaving infants—the most vulnerable age group—unprotected. This limitation spurred the creation of conjugate vaccines, which combined Hib polysaccharides with proteins to enhance immune response in younger children. By 1987, the first Hib conjugate vaccine, ProHIBIT (now discontinued), was approved in the U.S., marking a breakthrough in pediatric immunology.
The 1990s saw the introduction of more advanced Hib conjugate vaccines, such as ActHIB and PedvaxHIB, which were approved for infants as young as two months. These vaccines were administered in a series of doses—typically at 2, 4, and 6 months of age, with a booster at 12–15 months—to ensure robust immunity during the period of highest risk. The success of these vaccines led to a dramatic decline in Hib-related diseases, with cases in the U.S. dropping by over 99% within a decade of widespread vaccination.
Globally, the adoption of Hib vaccines followed a similar trajectory, though timelines varied. The World Health Organization (WHO) recommended Hib vaccination for all countries in 1998, but full integration into national immunization programs took years due to cost and accessibility challenges. Today, Hib vaccines are often combined with other antigens, such as DTaP and hepatitis B, in multi-dose formulations like Pentacel, streamlining administration and improving compliance.
In retrospect, the Hib vaccine’s development and approval timeline—spanning from the 1970s to the 1990s—exemplifies the iterative process of vaccine science. From initial failures to global success, it underscores the importance of targeted research, technological innovation, and public health collaboration. For parents and caregivers, ensuring timely Hib vaccination remains a critical step in protecting children from preventable, life-threatening diseases.
Pfizer Vaccine Ingredients: A Detailed Breakdown of Its Components
You may want to see also
Explore related products






![]()
Age Recommendations: What ages are recommended for Hib vaccine administration in children?
The Hib vaccine, a cornerstone of pediatric immunization, is typically administered in a series of doses starting as early as 2 months of age. This initial dose is crucial, as it primes the immune system to recognize and combat *Haemophilus influenzae* type b (Hib), a bacterium that can cause severe infections like meningitis and pneumonia. Subsequent doses are given at 4 months and 6 months of age, with a booster dose recommended between 12 and 15 months. This schedule ensures that infants develop robust immunity during their most vulnerable period.
While the standard schedule is widely followed, variations exist based on vaccine type and regional guidelines. For instance, some Hib vaccines are combined with other antigens, such as diphtheria, tetanus, and pertussis (DTaP), streamlining the immunization process. In such cases, the number of doses or intervals between them may differ slightly. For example, a combination vaccine like DTaP-Hib-IPV may be given at 2, 4, 6, and 15–18 months, with the Hib component adhering to the core schedule. Always consult local health authorities or a pediatrician to confirm the appropriate regimen for your child.
Catch-up vaccination is another critical aspect of Hib immunization, particularly for children who missed early doses. For children aged 7–11 months who received only one or two doses, a single additional dose is typically sufficient. However, children aged 12–59 months who are unvaccinated or incompletely vaccinated require a two-dose series, with doses spaced 2 months apart. This ensures that even older children can achieve adequate protection against Hib-related diseases.
Practical tips for parents include scheduling vaccinations during well-child visits to minimize stress and ensuring that children are healthy at the time of vaccination. Mild side effects, such as redness at the injection site or low-grade fever, are common and generally resolve within a day or two. Keeping a record of vaccination dates is essential, as it helps healthcare providers determine if additional doses or boosters are needed. By adhering to these recommendations, parents can safeguard their children from the potentially devastating effects of Hib infections.
Florida Trial Vaccine: Breast Cancer Eliminated
You may want to see also
Explore related products





![]()
Historical Impact: How has the Hib vaccine reduced diseases like meningitis and pneumonia?
The Hib vaccine, first licensed in the United States in 1985, has been a cornerstone in the fight against *Haemophilus influenzae* type b (Hib) infections, which were once a leading cause of bacterial meningitis and pneumonia in young children. Before its introduction, Hib diseases were responsible for approximately 20,000 cases of invasive infections annually in the U.S. alone, with meningitis and pneumonia accounting for the majority of severe outcomes. The vaccine’s development marked a turning point in pediatric health, offering a shield against these life-threatening conditions.
Analyzing its impact, the Hib vaccine has demonstrated remarkable efficacy in reducing disease burden. Studies show that within five years of its introduction, Hib-related meningitis cases in the U.S. plummeted by over 90%. Similarly, pneumonia cases linked to Hib dropped significantly, particularly in children under five, who are most vulnerable. This success is attributed to the vaccine’s ability to stimulate the production of antibodies against the Hib bacterium, preventing colonization and subsequent infection. The recommended dosage for infants typically involves a series of shots at 2, 4, and 6 months, with a booster at 12–15 months, ensuring robust immunity during the critical early years.
From a comparative perspective, the Hib vaccine’s impact is even more striking when contrasted with pre-vaccine era statistics. In the 1980s, Hib meningitis was fatal in 5% of cases and left 15–30% of survivors with permanent disabilities, such as hearing loss or developmental delays. Post-vaccination, these numbers have become rare in countries with high immunization rates. For instance, the UK saw a 98% reduction in Hib cases within a decade of introducing the vaccine into its routine immunization schedule. This underscores the vaccine’s role not just in saving lives but also in preventing long-term disabilities.
Practically, the Hib vaccine’s integration into global immunization programs has been a game-changer. In low-income countries, where access to healthcare is limited, the vaccine has been particularly impactful. The GAVI Alliance, a global health partnership, has supported Hib vaccination in over 70 countries, leading to a 70% reduction in Hib-related deaths worldwide. Parents in these regions are advised to adhere strictly to the vaccination schedule, as delays can leave children susceptible during peak vulnerability periods. Additionally, combining the Hib vaccine with other routine immunizations, such as DTaP and pneumococcal vaccines, has streamlined healthcare delivery and improved coverage rates.
In conclusion, the Hib vaccine’s historical impact on reducing meningitis and pneumonia is a testament to the power of immunization. Its introduction has not only saved millions of lives but also alleviated the socioeconomic burden of treating and managing these diseases. As the vaccine continues to evolve, with newer conjugates offering broader protection, its legacy as a public health triumph remains unchallenged. For parents and healthcare providers, ensuring timely vaccination remains the most effective strategy to safeguard children from Hib’s devastating effects.
STD Vaccines: What Exists and What's on the Horizon?
You may want to see also
Explore related products




![]()
Vaccine Composition: What components make up the Hib vaccine and how do they work?
The Hib vaccine, a cornerstone in pediatric immunization, has been protecting children from *Haemophilus influenzae* type b (Hib) infections since its introduction in the 1990s. Its composition is a marvel of scientific precision, designed to elicit a robust immune response without causing the disease itself. At its core, the vaccine contains purified polysaccharides from the Hib bacteria’s capsule, a structure that shields the pathogen from the immune system. However, these polysaccharides alone are poorly immunogenic in infants, the primary target group. To address this, the Hib vaccine employs a strategy called conjugation, where the polysaccharides are chemically linked to a carrier protein, typically tetanus toxoid or meningococcal protein. This conjugation transforms the vaccine into a potent immunogen, capable of stimulating both short-term and long-term immunity in children as young as 2 months old.
Analyzing the vaccine’s mechanism reveals a sophisticated interplay between its components and the immune system. When administered, the conjugated polysaccharide-protein complex is recognized as foreign by the body’s immune cells. Antigen-presenting cells (APCs) engulf the vaccine particles, process them, and present fragments of the polysaccharide and carrier protein to T cells. This triggers a cascade of immune responses, including the production of antibodies specifically targeted at the Hib capsule. The carrier protein also stimulates T-cell-dependent memory, ensuring that the immune system “remembers” the pathogen for future encounters. This dual action is why the Hib vaccine is so effective, reducing Hib meningitis cases by over 99% in countries with widespread immunization programs.
Practical considerations for administering the Hib vaccine highlight its adaptability to different age groups and health contexts. Infants typically receive a primary series of 2–3 doses starting at 2 months of age, with a booster dose around 12–15 months. The exact schedule varies by country and vaccine brand, such as ActHIB® or PedvaxHIB®, but all formulations adhere to the conjugation principle. For children with compromised immune systems, additional doses or adjusted schedules may be recommended. Notably, the Hib vaccine is often combined with other vaccines, such as DTaP (diphtheria, tetanus, pertussis) or pneumococcal vaccines, to streamline immunization and improve compliance. This combination approach underscores the vaccine’s versatility and its role in comprehensive childhood immunization strategies.
A comparative look at Hib vaccine formulations reveals subtle differences that impact their efficacy and usage. For instance, PRP-T (polysaccharide conjugated to tetanus toxoid) and PRP-OMP (polysaccharide conjugated to meningococcal outer membrane protein) are two common types. PRP-T vaccines, like ActHIB®, are widely used globally due to their proven track record and cost-effectiveness. PRP-OMP vaccines, such as PedvaxHIB®, offer the advantage of being immunogenic in younger infants and requiring fewer doses, but they are generally more expensive. These variations highlight the importance of tailoring vaccine selection to regional health needs, resource availability, and epidemiological trends.
In conclusion, the Hib vaccine’s composition is a testament to the ingenuity of vaccine design, blending purified polysaccharides and carrier proteins to create a safe, effective, and adaptable immunization tool. Its mechanism of action, rooted in conjugation and immune memory, ensures robust protection against a once-devastating pathogen. Practical considerations, from dosing schedules to combination formulations, further enhance its utility in global health programs. Understanding these components and their functions not only underscores the vaccine’s significance but also empowers healthcare providers and parents to make informed decisions about Hib immunization.
Subcutaneous Vaccines: Which Shots Should Be Administered Under the Skin?
You may want to see also
![]()
Global Availability: When did the Hib vaccine become widely accessible worldwide?
The Hib vaccine, a cornerstone in preventing Haemophilus influenzae type b (Hib) infections, began its journey in the late 1970s and early 1980s. However, its global availability was a gradual process, influenced by factors such as manufacturing capacity, cost, and public health priorities. While high-income countries like the United States and those in Western Europe introduced the vaccine into their routine immunization schedules by the mid-1990s, low- and middle-income countries faced significant delays. The turning point came with the establishment of the Gavi, the Vaccine Alliance, in 2000, which aimed to accelerate access to vaccines for the world’s poorest children. By 2006, over 100 countries had incorporated the Hib vaccine into their national immunization programs, marking a significant milestone in its global accessibility.
Analyzing the timeline reveals a stark disparity in access. In the United States, the Hib vaccine was licensed in 1985, and by 1990, it was widely available, leading to a 95% reduction in Hib cases within a decade. Contrast this with sub-Saharan Africa, where introduction lagged until the early 2000s due to financial constraints and logistical challenges. For instance, Kenya introduced the Hib vaccine in 2001, while Nigeria followed in 2007. This delay highlights the critical role of international partnerships in bridging the gap between developed and developing nations. The Hib vaccine’s global rollout underscores the importance of sustained investment in vaccine infrastructure and equitable distribution.
From a practical standpoint, the Hib vaccine is typically administered in a series of doses, starting as early as 2 months of age. The World Health Organization (WHO) recommends a 2- or 3-dose primary series, depending on the vaccine formulation, followed by a booster dose at 12–15 months. In regions with high Hib disease burden, early and complete vaccination is crucial. Parents and caregivers should adhere to the recommended schedule, as partial vaccination may not provide adequate protection. Additionally, healthcare providers in low-resource settings must navigate challenges like cold chain maintenance and supply chain disruptions to ensure consistent availability.
Persuasively, the global availability of the Hib vaccine is a testament to the power of collaboration and innovation in public health. The vaccine’s success in reducing meningitis, pneumonia, and other Hib-related diseases has saved millions of lives, particularly among children under 5. However, disparities persist, with some countries still struggling to achieve full coverage. Advocates must continue to push for increased funding, policy support, and community engagement to ensure that every child, regardless of geography, has access to this life-saving intervention. The Hib vaccine’s story is not just about its age but about the ongoing effort to make it universally accessible.
Comparatively, the Hib vaccine’s global rollout shares similarities with other vaccines like pneumococcal conjugate vaccine (PCV) and rotavirus vaccine, which also faced delays in reaching low-income countries. However, the Hib vaccine’s journey stands out due to its earlier development and the lessons learned from its distribution, which informed strategies for subsequent vaccines. For example, the Hib vaccine’s success in reducing disease burden provided a compelling case for investing in vaccine programs, paving the way for faster uptake of newer vaccines. This historical context emphasizes the need for proactive planning and resource allocation to ensure timely global access to future vaccines.
DC's New Bill: Vaccinating Children?
You may want to see also
Frequently asked questions
The Hib (Haemophilus influenzae type b) vaccine was first licensed for use in the United States in 1985, making it over 35 years old.
The Hib vaccine became widely available in the late 1980s and early 1990s, after its initial introduction in 1985.
Since its introduction, the Hib vaccine has been improved with the development of conjugate vaccines, which are more effective and suitable for infants. It is now often combined with other vaccines for convenience.
Yes, the Hib vaccine is still in use today and is a routine part of childhood immunization schedules worldwide, effectively preventing Hib-related diseases.
The Hib vaccine is typically administered to infants starting at 2 months of age, with additional doses given at 4 months, 6 months (depending on the brand), and a booster dose at 12–15 months.