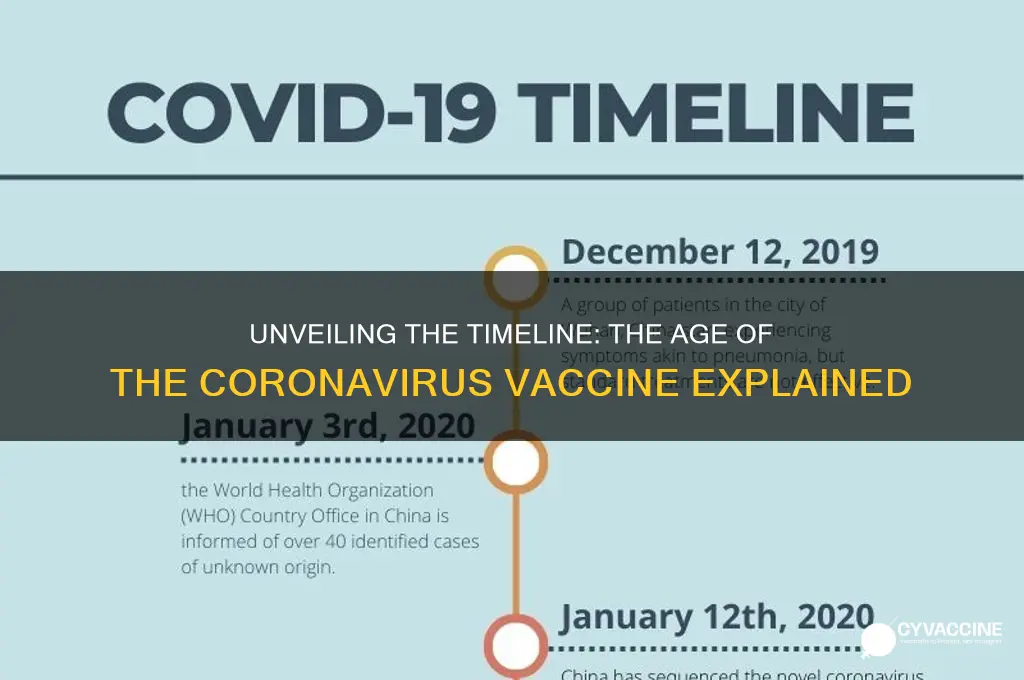
The coronavirus vaccine, developed in response to the global COVID-19 pandemic, emerged with unprecedented speed due to international scientific collaboration and advancements in mRNA technology. The first vaccines, such as Pfizer-BioNTech and Moderna, received emergency use authorization in late 2020, less than a year after the pandemic began. This rapid development was made possible by decades of research on coronaviruses and vaccine platforms, as well as significant investment and regulatory streamlining. Since then, the vaccines have undergone continuous monitoring and updates to address new variants, ensuring their effectiveness and safety. As of now, the coronavirus vaccine is just over three years old, marking a historic milestone in medical science and public health.
| Characteristics | Values |
|---|---|
| First Authorized Vaccine | December 2020 (Pfizer-BioNTech, Moderna, and AstraZeneca in various regions) |
| Vaccine Development Time | ~10 months (unprecedented speed due to global collaboration and funding) |
| Vaccine Types | mRNA (Pfizer, Moderna), Viral Vector (AstraZeneca, J&J), Inactivated (Sinovac, Sinopharm) |
| Global Rollout Start | December 2020 |
| Current Age of Vaccines | ~3.5 years (as of June 2024) |
| Booster Availability | Available since late 2021, with updated formulations for variants |
| Vaccination Coverage | Over 13 billion doses administered globally (as of June 2024) |
| Efficacy Against Variants | Varies; updated boosters target Omicron and other variants |
| Safety Profile | Proven safe and effective, with rare side effects monitored globally |
| Ongoing Research | Continuous studies on long-term immunity and next-generation vaccines |
Explore related products





What You'll Learn
- Vaccine Development Timeline: From research to approval, tracing the COVID-19 vaccine's creation process
- First Vaccine Approval: Pfizer-BioNTech's historic authorization in December 2020 marked a global milestone
- Vaccine Age Requirements: Initial rollout focused on adults, later expanded to include children
- Booster Shot Timing: Recommendations for additional doses to maintain immunity over time
- Global Vaccine Distribution: Efforts to ensure equitable access across countries and populations
![]()
Vaccine Development Timeline: From research to approval, tracing the COVID-19 vaccine's creation process
The COVID-19 vaccines emerged with unprecedented speed, but their development was no overnight miracle. Tracing their journey from research to approval reveals a meticulous process compressed into a fraction of the typical vaccine timeline. This acceleration was achieved through global collaboration, innovative technologies, and strategic prioritization, not by cutting corners.
Let's dissect the key stages:
Preclinical Research & Platform Selection (Early 2020): Within weeks of the SARS-CoV-2 genome sequencing in January 2020, researchers leveraged existing knowledge from previous coronavirus outbreaks (SARS, MERS) to identify the virus's spike protein as a prime target. This allowed them to rapidly adapt vaccine platforms like mRNA (Pfizer-BioNTech, Moderna) and viral vector (AstraZeneca, Johnson & Johnson). These platforms, already under development for other diseases, offered a head start, bypassing years of foundational research.
Animal studies commenced immediately, assessing safety and immunogenicity (the ability to provoke an immune response).
- Clinical Trials: A Phased Approach (Spring 2020 - Late 2020): Phase 1 trials focused on safety and dosage, enrolling small groups of healthy volunteers. Phase 2 expanded to larger groups, refining dosage and gathering preliminary efficacy data. Phase 3, the largest and most crucial, involved tens of thousands of participants, randomly assigned to receive either the vaccine or a placebo. This stage rigorously tested efficacy in preventing symptomatic COVID-19 and monitored for rare side effects. Notably, trials overlapped to save time, a departure from traditional sequential phases.
- Emergency Use Authorization & Rolling Reviews (Late 2020 - Early 2021): Regulatory agencies like the FDA implemented rolling reviews, analyzing data as it became available during trials, rather than waiting for complete submissions. This allowed for expedited evaluation without compromising safety standards. Emergency Use Authorization (EUA) was granted based on compelling Phase 3 data, permitting immediate distribution to high-risk populations while ongoing studies continued to gather long-term safety and efficacy data.
- Manufacturing & Distribution: A Global Effort (2021 - Present): Scaling up production to meet global demand presented a monumental challenge. Manufacturers invested in new facilities, optimized supply chains, and collaborated internationally to ensure equitable access. Distribution required meticulous planning, considering cold chain requirements (especially for mRNA vaccines) and prioritizing vulnerable populations.
Practical Takeaways:
- Dosage & Administration: Most COVID-19 vaccines require two primary doses, with boosters recommended periodically to maintain immunity. Dosage varies by vaccine type and age group. Follow healthcare provider instructions and stay updated on evolving recommendations.
- Age Eligibility: Initially approved for adults, vaccines were gradually authorized for younger age groups as safety and efficacy data became available. Currently, vaccines are available for individuals as young as 6 months old, with specific formulations tailored to different age categories.
- Stay Informed: Vaccine development is an ongoing process. New variants and emerging data may lead to updated formulations or adjusted dosing schedules. Stay informed through reliable sources like the CDC, WHO, and local health authorities.
COVID-19 Vaccines: Immune Booster or Buster?
You may want to see also
Explore related products






![]()
First Vaccine Approval: Pfizer-BioNTech's historic authorization in December 2020 marked a global milestone
The Pfizer-BioNTech COVID-19 vaccine, authorized for emergency use by the U.S. FDA on December 11, 2020, was the first to receive such approval globally. This milestone marked a turning point in the pandemic, offering a glimmer of hope after months of lockdowns, surging cases, and overwhelming healthcare systems. The vaccine’s rapid development, from lab to authorization in less than a year, was unprecedented, thanks to mRNA technology and global collaboration. This authorization wasn’t just a scientific achievement—it was a logistical and regulatory triumph, setting the stage for mass vaccination campaigns worldwide.
Analytically, the Pfizer-BioNTech vaccine’s approval was a testament to the power of innovation and urgency. Unlike traditional vaccines, which rely on weakened viruses or viral proteins, this mRNA vaccine instructs cells to produce a harmless piece of the SARS-CoV-2 spike protein, triggering an immune response. The Phase 3 trial involved over 43,000 participants, demonstrating 95% efficacy in preventing symptomatic COVID-19. However, the authorization came with conditions: it was initially approved for individuals aged 16 and older, with a two-dose regimen administered 21 days apart. Each dose contains 30 micrograms of mRNA, a precise formulation that balances efficacy and safety.
Instructively, the rollout of the Pfizer-BioNTech vaccine required meticulous planning. Its ultra-cold storage requirement (-70°C) posed significant challenges, necessitating specialized freezers and thermal shipping containers. Healthcare providers had to adhere to strict handling guidelines to ensure vaccine stability. For recipients, the process was straightforward: a quick injection in the deltoid muscle, followed by a 15-minute observation period to monitor for rare allergic reactions. Practical tips included scheduling the second dose promptly and reporting side effects (e.g., fatigue, headache, or fever) through platforms like the CDC’s v-safe program.
Persuasively, the Pfizer-BioNTech authorization wasn’t just about science—it was about restoring hope. By December 2020, global COVID-19 deaths had surpassed 1.5 million, and economies were reeling. The vaccine’s approval signaled that humanity could fight back against the virus. It also highlighted the importance of equitable distribution, as wealthier nations initially secured the majority of doses. The authorization spurred other regulatory bodies worldwide to expedite their reviews, accelerating vaccine availability across continents. This moment underscored the need for global solidarity in the face of a shared threat.
Comparatively, the Pfizer-BioNTech vaccine’s approval stands out when contrasted with other milestones. While Moderna’s mRNA vaccine followed closely behind, authorized in December 2020, and AstraZeneca’s viral vector vaccine gained approval in the UK in December 2020 and later elsewhere, Pfizer-BioNTech’s was the first to cross the finish line. Its success paved the way for subsequent vaccines and demonstrated the potential of mRNA technology for future pandemics. As of 2023, over 14 billion COVID-19 vaccine doses have been administered globally, a testament to the impact of that historic December 2020 authorization.
Hepatitis B Vaccine Symptoms: What to Expect After Vaccination
You may want to see also
Explore related products






![]()
Vaccine Age Requirements: Initial rollout focused on adults, later expanded to include children
The initial rollout of the coronavirus vaccine prioritized adults, particularly those over 65 and individuals with underlying health conditions, due to their heightened risk of severe illness and death. This strategic decision was based on clinical trial data, which primarily involved adult participants, and the urgent need to protect the most vulnerable populations. As vaccine supply stabilized and real-world efficacy data emerged, health authorities gradually expanded eligibility to younger age groups, including adolescents and, eventually, children as young as 6 months.
From an analytical perspective, this phased approach balanced risk mitigation with logistical feasibility. Adults, especially older adults, accounted for the majority of COVID-19 hospitalizations and fatalities, making them the logical first recipients. For instance, the Pfizer-BioNTech vaccine received emergency use authorization (EUA) for individuals aged 16 and older in December 2020, followed by Moderna’s EUA for those 18 and up. This adult-first strategy not only saved lives but also allowed healthcare systems to monitor vaccine safety and efficacy in a controlled manner before extending access to younger, generally healthier populations.
When the rollout expanded to children, dosage adjustments became critical. For example, children aged 5–11 received one-third of the adult dose of the Pfizer vaccine, while those under 5 received an even smaller amount. This precision ensured safety and efficacy, as children’s immune systems respond differently to vaccines. Parents and caregivers were advised to consult pediatricians to address concerns about side effects, such as fever or fatigue, which are typically mild and short-lived. The expansion to younger age groups also required child-friendly vaccination sites and communication strategies to ease anxiety and encourage uptake.
Comparatively, the inclusion of children marked a turning point in the pandemic response, shifting from individual protection to community immunity. Vaccinating children not only reduced their risk of severe illness but also minimized transmission in schools and households, protecting vulnerable individuals who could not be vaccinated. However, this phase faced unique challenges, including lower parental acceptance rates and the need for age-appropriate formulations. For instance, the Moderna vaccine for children aged 6–17 was authorized later than Pfizer’s, providing families with additional options but also complicating public health messaging.
In conclusion, the evolution of vaccine age requirements from adults to children exemplifies adaptive public health strategy. It underscores the importance of data-driven decision-making, tailored dosing, and targeted outreach. As the pandemic continues to evolve, this approach serves as a model for future vaccine rollouts, emphasizing flexibility, inclusivity, and the critical role of age-specific considerations in achieving widespread immunity.
Lyme Disease Vaccine for Horses: Availability, Benefits, and Prevention Tips
You may want to see also
Explore related products






![]()
Booster Shot Timing: Recommendations for additional doses to maintain immunity over time
The COVID-19 vaccines have been a cornerstone of the global response to the pandemic, with the first doses administered in December 2020. As time passes, the question of booster shots becomes increasingly relevant. Immunity wanes naturally over time, and new variants emerge, making it crucial to understand when and why additional doses are necessary.
The Science Behind Booster Timing
Research indicates that the protective effects of COVID-19 vaccines, particularly against symptomatic infection and mild illness, begin to decline approximately 6 to 8 months after the initial series. This is not unique to COVID-19 vaccines; many vaccines require periodic boosters to maintain immunity. For instance, the Pfizer-BioNTech and Moderna mRNA vaccines show a gradual decrease in efficacy against infection, though protection against severe disease remains robust for longer. Studies suggest that a booster dose significantly enhances antibody levels, restoring protection to over 90% against severe outcomes.
Who Needs a Booster and When?
Health authorities, such as the CDC and WHO, recommend booster shots for most individuals, with specific guidelines based on age, health status, and vaccine type. For adults aged 18 and older, a booster is advised 5 months after completing the Pfizer or Moderna series, or 2 months after the Johnson & Johnson single-dose vaccine. Immunocompromised individuals, including those undergoing cancer treatment or organ transplant recipients, should receive an additional dose 28 days after their initial series, followed by a booster at the standard interval. Adolescents aged 12–17 are eligible for a Pfizer booster 5 months after their second dose, though recommendations may vary by region.
Practical Tips for Scheduling Your Booster
Timing is key to maximizing the benefits of a booster shot. Plan your appointment around the recommended interval, but don’t stress if you’re a few weeks late—getting the booster is more important than strict adherence to the timeline. Consider seasonal trends; for example, getting boosted before winter can provide added protection during peak respiratory virus seasons. If you’ve recently had COVID-19, wait at least 3 months after recovery before getting a booster, as natural immunity can temporarily enhance vaccine efficacy.
Balancing Risks and Benefits
While boosters are highly effective, it’s essential to weigh individual needs against potential side effects, which are typically mild and short-lived, including fatigue, headache, and soreness at the injection site. For older adults and those with comorbidities, the benefits of reduced hospitalization and death risk far outweigh these minor inconveniences. Conversely, young, healthy individuals may experience more pronounced side effects, though the long-term protective benefits still justify the booster.
Looking Ahead: The Future of Booster Recommendations
As the virus evolves, so too will booster strategies. Bivalent vaccines, targeting both the original strain and Omicron variants, are already in use, offering broader protection. Experts are exploring the possibility of annual boosters, similar to the flu shot, to keep pace with emerging variants. Staying informed through trusted sources and consulting healthcare providers will remain critical as guidelines continue to adapt to the changing landscape of the pandemic.
Global Vaccination Progress: Tracking Worldwide Immunization Efforts and Impact
You may want to see also
Explore related products






![]()
Global Vaccine Distribution: Efforts to ensure equitable access across countries and populations
The COVID-19 vaccines, first authorized in late 2020, have been administered in over 13 billion doses globally as of 2023. Yet, this staggering number masks a stark disparity: while some nations have vaccinated over 80% of their populations, others struggle to reach 10% coverage. This gap underscores the urgent need for equitable vaccine distribution, a complex challenge requiring coordinated global efforts.
One key initiative addressing this imbalance is COVAX, a global collaboration co-led by the World Health Organization (WHO), Gavi, and the Coalition for Epidemic Preparedness Innovations (CEPI). COVAX aims to provide 2 billion vaccine doses to low- and middle-income countries by the end of 2023, prioritizing healthcare workers and vulnerable populations. For instance, in countries like Ghana and Rwanda, COVAX has delivered millions of doses, enabling vaccination campaigns targeting individuals aged 12 and older, with specific protocols for administering a 30-microgram dose of the Pfizer-BioNTech vaccine to adolescents.
However, equitable distribution isn’t just about delivering doses—it’s about ensuring they’re accessible and acceptable. In remote areas, cold chain logistics pose a significant hurdle, as vaccines like Moderna require storage at -20°C. Solar-powered refrigerators and drone deliveries have emerged as innovative solutions, though their scalability remains limited. Additionally, vaccine hesitancy fueled by misinformation demands localized communication strategies. In India, for example, community health workers conducted door-to-door campaigns, dispelling myths and encouraging uptake among elderly populations, who often require a second booster dose for enhanced protection.
A comparative analysis reveals that high-income countries initially hoarded vaccines, purchasing enough doses to vaccinate their populations multiple times over. This "vaccine nationalism" delayed global equity efforts. In contrast, countries like Cuba and China prioritized sharing their domestically produced vaccines with Latin America and Africa, respectively. Such examples highlight the importance of diversifying vaccine sources and fostering South-South cooperation.
To sustain progress, global leaders must address structural barriers. Wealthy nations should fulfill funding pledges to COVAX and waive intellectual property rights for vaccine production, enabling local manufacturing in low-resource settings. Simultaneously, countries must strengthen their health systems to administer vaccines efficiently. Practical tips for governments include mapping vulnerable populations, training healthcare workers in dose administration (e.g., 0.5 mL for AstraZeneca), and leveraging digital platforms for appointment scheduling and monitoring.
In conclusion, ensuring equitable vaccine access is a moral and practical imperative. While strides have been made, the journey is far from over. By combining global solidarity, innovative solutions, and local action, the world can bridge the vaccine divide and protect all populations from COVID-19.
Lyme Disease Vaccination for Pets: Optimal Frequency and Timing Explained
You may want to see also
Frequently asked questions
The first COVID-19 vaccines were authorized for emergency use in December 2020, making them approximately 3 years old as of 2023.
The first COVID-19 vaccines, such as Pfizer-BioNTech and Moderna, were developed and authorized in late 2020, following an unprecedented global effort to combat the pandemic.
Yes, the COVID-19 vaccines have been administered to billions of people worldwide since 2020, with extensive monitoring confirming their safety and effectiveness in preventing severe illness and death.