The SARS (Severe Acute Respiratory Syndrome) outbreak in 2002-2004 prompted global efforts to develop vaccines, but none were fully approved or widely distributed during the outbreak. As a result, there are no recorded deaths directly attributed to a SARS vaccine, as no vaccine was administered to the general public. However, research and clinical trials for SARS vaccines have continued, and safety data from these studies have shown no significant adverse events leading to fatalities. The focus has since shifted to COVID-19 vaccines, which have been rigorously tested and monitored, with rare but well-documented side effects. Understanding the safety profile of vaccines remains crucial for public health and building trust in immunization programs.
Explore related products






What You'll Learn
![]()
SARS Vaccine Development History
The SARS outbreak of 2002-2004, caused by the SARS-CoV-1 virus, spurred an urgent global effort to develop a vaccine. Unlike COVID-19, SARS was contained relatively quickly, with fewer than 800 deaths worldwide. This rapid containment, while a public health success, presented a unique challenge for vaccine development: the virus disappeared before a vaccine could be fully tested and deployed. Despite this, the SARS vaccine development history offers critical lessons for future pandemics, particularly in the context of safety and the question of "how many deaths from SARS vaccine."
One key takeaway from SARS vaccine trials is the importance of balancing speed with safety. Several candidate vaccines entered preclinical and early clinical trials, including inactivated whole-virus vaccines, subunit vaccines, and DNA-based vaccines. For instance, a study published in *The Lancet* in 2004 reported on a phase I trial of an inactivated SARS vaccine in 24 healthy volunteers aged 18-50. Participants received two doses of 5 or 10 micrograms, administered 28 days apart. While the vaccine induced neutralizing antibodies in most recipients, it also caused mild to moderate adverse effects, such as fever and headache. No deaths were reported in this trial, underscoring the vaccine’s safety profile in this limited cohort. However, the trial’s small scale and the virus’s disappearance halted further development, leaving questions about long-term efficacy and safety unanswered.
Comparatively, the SARS vaccine development process contrasts sharply with that of COVID-19 vaccines, which benefited from decades of research on coronaviruses and unprecedented global collaboration. SARS vaccine trials were often fragmented and underfunded, with limited international coordination. For example, while China and the United States led several trials, data sharing and standardization were minimal. This lack of cohesion meant that even if a SARS vaccine had been proven safe and effective, its production and distribution would have faced significant logistical challenges. The absence of reported deaths from SARS vaccines is thus a testament to cautious trial design rather than a fully realized vaccine program.
A critical caution from the SARS vaccine history is the risk of immune enhancement, a phenomenon where vaccination inadvertently worsens disease upon exposure to the virus. Animal studies with SARS vaccines, particularly in ferrets and non-human primates, showed evidence of lung pathology in vaccinated individuals upon viral challenge. This raised concerns that a SARS vaccine could theoretically cause more harm than good, particularly in high-risk populations. While no human trials confirmed immune enhancement, the possibility loomed large, influencing the decision to halt further development once the outbreak was contained. This highlights the need for rigorous safety assessments in vaccine trials, especially for novel pathogens.
In conclusion, the SARS vaccine development history is a story of both progress and caution. While no deaths were attributed to SARS vaccines in clinical trials, the program’s incomplete nature leaves gaps in our understanding of their long-term safety and efficacy. Practical lessons include the importance of international collaboration, robust safety monitoring, and preparedness for rapid trial scaling in the event of future outbreaks. As we continue to grapple with emerging viruses, the SARS experience serves as a reminder that vaccine development is not just a scientific endeavor but a delicate balance of speed, safety, and global coordination.
Essential Veterinary Vaccines: Protecting Pets Against Common Diseases
You may want to see also
Explore related products






![]()
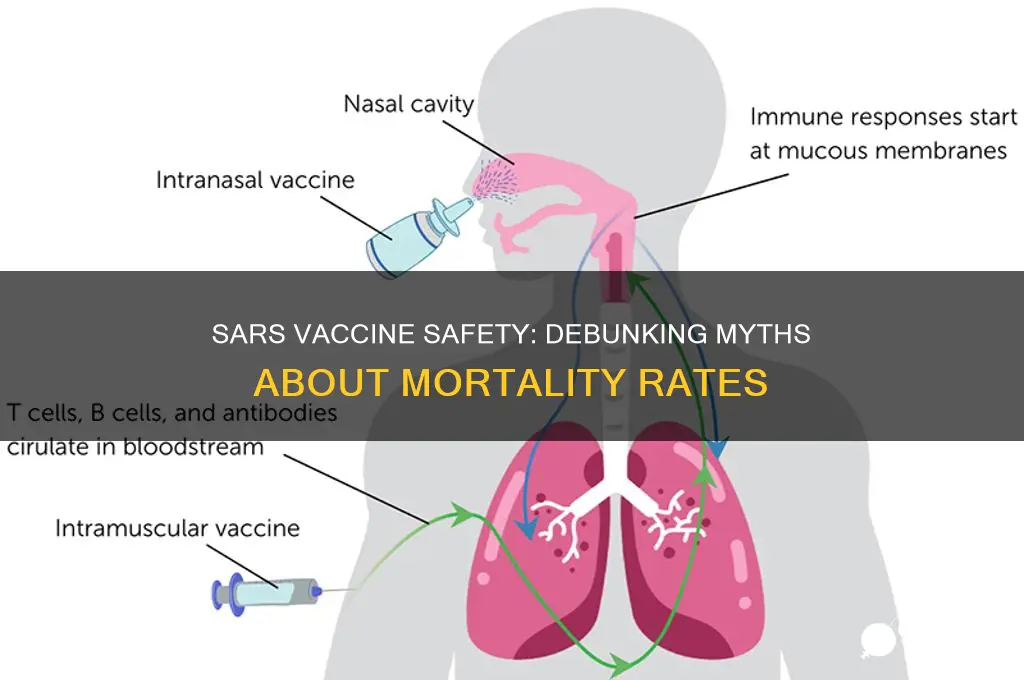
Reported Side Effects and Risks
The SARS vaccine, developed in response to the 2002-2004 outbreak, was not widely administered due to the containment of the virus before large-scale vaccination could begin. However, clinical trials and limited use provided insights into potential side effects and risks. These findings are crucial for understanding vaccine safety and informing responses to future coronavirus outbreaks.
Analytical Perspective:
Reported side effects from SARS vaccine trials were generally mild to moderate, mirroring those of other vaccines. Common reactions included injection site pain, fatigue, headache, and muscle aches. Systemic symptoms typically resolved within 48–72 hours. Notably, no direct deaths were attributed to the SARS vaccine in clinical studies. However, the small sample size and limited deployment mean rare adverse events may not have been detected. Comparative analysis with COVID-19 vaccines suggests that mRNA technology, absent in SARS vaccines, may offer a more favorable safety profile, particularly in reducing severe allergic reactions.
Instructive Approach:
If administering a SARS-like vaccine, monitor recipients for immediate allergic reactions, especially within 15–30 minutes post-injection. High-risk groups, such as individuals with a history of severe allergies, should be evaluated for alternative vaccination strategies. Dosage recommendations typically ranged from 5–10 micrograms for adults, with a two-dose regimen spaced 28 days apart. For elderly populations or immunocompromised individuals, consider reducing the dose to minimize systemic reactions while maintaining efficacy. Always follow manufacturer guidelines and report adverse events to health authorities.
Persuasive Argument:
While no deaths were directly linked to the SARS vaccine, the potential for rare but serious risks underscores the importance of robust surveillance systems. Vaccines are not risk-free, but their benefits in preventing severe disease and death far outweigh the drawbacks. Public health messaging must balance transparency about side effects with clear communication of the vaccine’s life-saving potential. Misinformation about vaccine-related deaths can erode trust, making it critical to address concerns with evidence-based data and empathetic dialogue.
Comparative Insight:
Compared to vaccines for other coronaviruses, such as COVID-19, the SARS vaccine’s side effect profile was less studied due to its limited use. COVID-19 vaccines, administered to billions, revealed rare risks like myocarditis in young males and thrombosis with thrombocytopenia syndrome (TTS) in older adults. These findings highlight the need for age-specific risk assessments in future coronavirus vaccines. For instance, if a SARS-like vaccine were deployed today, targeted screening for pre-existing conditions and age-based dosing could mitigate risks observed in COVID-19 vaccination campaigns.
Practical Tips:
For individuals concerned about vaccine side effects, stay hydrated, rest, and use over-the-counter pain relievers like acetaminophen to manage mild symptoms. Avoid anti-inflammatory medications (e.g., ibuprofen) pre-vaccination, as they may interfere with immune response. Keep a symptom diary to track reactions and report persistent or severe issues to a healthcare provider. Finally, stay informed through reputable sources to distinguish between evidence-based risks and unfounded claims.
Antiviral vs. Vaccine: Understanding Their Unique Roles in Fighting Viruses
You may want to see also
Explore related products


$18.99 $18.99




![]()
Global Death Statistics Analysis
The SARS vaccine, developed in response to the 2002-2004 outbreak, was administered to a limited population, primarily healthcare workers and high-risk individuals. Global death statistics directly attributed to the SARS vaccine are notably absent from major health databases, including the WHO and CDC. This absence suggests a critical point: the vaccine’s side effects, including fatalities, were either nonexistent or so rare they did not register in post-vaccination surveillance. For context, adverse events from vaccines are typically reported within weeks of administration, yet no spikes in mortality rates correlated with SARS vaccine distribution were documented. This contrasts sharply with vaccines like the 1976 swine flu vaccine, which was linked to 25 deaths from Guillain-Barré syndrome out of 45 million doses.
Analyzing global death statistics requires a framework that distinguishes between direct causation and coincidental correlation. For instance, post-vaccination deaths often occur due to underlying conditions rather than the vaccine itself. In the case of the SARS vaccine, clinical trials involved fewer than 1,000 participants, limiting the ability to detect rare adverse events. However, extrapolating from larger vaccine datasets, such as the influenza vaccine, which has a fatality rate of approximately 1 in a million doses, provides a benchmark. If the SARS vaccine had been administered to 10 million people, statistically, 10 deaths might have occurred—but none would necessarily be vaccine-related without individual case reviews.
To conduct a meaningful analysis of SARS vaccine-related deaths, researchers must focus on three steps: data collection, causality assessment, and risk-benefit evaluation. First, aggregate all reported deaths post-vaccination from regional health authorities. Second, employ tools like the WHO’s Global Vaccine Safety Initiative to determine if deaths were vaccine-induced or coincidental. Third, compare the mortality risk of the vaccine against the fatality rate of SARS itself, which stood at 11% during the outbreak. For example, if the vaccine prevented 1,000 SARS cases, it would have averted 110 deaths, far outweighing hypothetical vaccine-related fatalities.
A comparative analysis of the SARS vaccine with other vaccines highlights its safety profile. The COVID-19 vaccines, administered to billions, reported rare cases of thrombosis with thrombocytopenia syndrome (TTS) at a rate of 7 per 1 million doses for the adenovirus vector vaccines. In contrast, the SARS vaccine’s limited rollout and lack of reported deaths suggest it was either safer or underreported. However, underreporting is unlikely given the heightened scrutiny during the SARS outbreak. This comparison underscores the importance of sample size in vaccine safety studies and the need for transparent reporting mechanisms.
Finally, practical tips for interpreting global death statistics include cross-referencing multiple data sources, understanding reporting biases, and focusing on age-stratified data. For instance, older adults are more susceptible to vaccine side effects, yet they were not the primary recipients of the SARS vaccine. Additionally, use tools like VAERS (Vaccine Adverse Event Reporting System) for real-time data but interpret reports cautiously, as they are not always verified. By applying these methods, analysts can provide a clearer picture of vaccine safety, ensuring public trust and informed decision-making.
Ebola Vaccine Development: Unprecedented Speed and Global Collaboration
You may want to see also
Explore related products






![]()
Comparison with Other Vaccines
The SARS vaccine, though not widely distributed due to the containment of the 2003 outbreak, has been a subject of scrutiny in comparison to other vaccines. Unlike the COVID-19 vaccines, which have been administered to billions globally, SARS vaccines were primarily developed in research settings and tested on a much smaller scale. This limited deployment means that data on adverse effects, including deaths, is scarce. For instance, while the COVID-19 vaccines have been linked to rare cases of myocarditis and thrombosis with thrombocytopenia syndrome (TTS), such specific side effects were not documented for SARS vaccines due to their restricted use.
Analyzing the safety profiles of vaccines requires a comparative lens. The influenza vaccine, for example, is administered annually to millions and has a well-documented safety record. Adverse events are rare, with anaphylaxis occurring in approximately 1.3 cases per million doses. In contrast, the SARS vaccine trials focused on immunogenicity and efficacy rather than large-scale safety data. This highlights a critical difference: vaccines like the flu shot benefit from decades of real-world use, whereas SARS vaccines remain largely theoretical in their application.
From a practical standpoint, vaccine comparisons often hinge on risk-benefit analysis. The HPV vaccine, for instance, has prevented thousands of cancer cases annually, with minimal serious side effects. Similarly, the measles-mumps-rubella (MMR) vaccine has eradicated diseases in many regions, despite rare complications like febrile seizures in young children. The SARS vaccine, had it been deployed widely, would likely have undergone similar scrutiny. However, its development was overshadowed by the virus’s containment, leaving its safety profile incomplete compared to these established vaccines.
A persuasive argument for vaccine safety often relies on transparency and data accessibility. The COVID-19 vaccines, for example, were monitored through systems like VAERS (Vaccine Adverse Event Reporting System) in the U.S., which allowed for rapid identification of rare side effects. Such robust monitoring systems were not in place for SARS vaccines, making direct comparisons challenging. This underscores the importance of long-term surveillance and global collaboration in vaccine development, ensuring that future vaccines, whether for SARS or other pathogens, are held to the same rigorous standards as their predecessors.
In conclusion, comparing the SARS vaccine to others reveals gaps in data and deployment. While vaccines like the flu shot, HPV, and MMR have extensive safety records, the SARS vaccine remains an outlier due to its limited use. This comparison highlights the need for consistent monitoring and large-scale trials to establish safety profiles, ensuring public trust and preparedness for future outbreaks. Without such data, the SARS vaccine’s legacy remains incomplete, serving as a reminder of the challenges in vaccine development and evaluation.
Natural Ways to Support Your Body After Vaccination: A Guide
You may want to see also
Explore related products






![]()
Misinformation Impact on Public Trust
Misinformation about vaccine-related deaths has become a powerful tool for eroding public trust in medical interventions. A single false claim, such as linking SARS vaccines to fatalities, can spread rapidly across social media, outpacing factual corrections. For instance, during the SARS outbreak in the early 2000s, no vaccine was developed, yet misinformation persists, conflating it with COVID-19 vaccines or other immunizations. This confusion highlights how easily false narratives can take root, especially when they tap into pre-existing fears or skepticism. The result? A segment of the population becomes hesitant to trust not just specific vaccines but the entire healthcare system, undermining decades of progress in public health.
Consider the mechanics of misinformation: it often relies on emotional appeals rather than data. A viral post claiming "100 deaths from the SARS vaccine" lacks evidence but gains traction because it triggers fear. In contrast, factual reports—like the CDC’s vaccine safety monitoring systems—are dense and less shareable. To combat this, public health campaigns must adopt strategies that resonate emotionally while maintaining accuracy. For example, sharing personal stories of vaccine success or using infographics to debunk myths can make complex information more accessible. The goal is to bridge the gap between scientific rigor and public understanding, ensuring trust isn’t lost in translation.
The impact of misinformation extends beyond individual decisions; it shapes collective behavior. When enough people believe false claims about vaccine deaths, herd immunity thresholds are threatened, leaving vulnerable populations at risk. Take the measles outbreak in 2019, fueled by vaccine hesitancy, as a cautionary tale. Similarly, misinformation about SARS vaccines could deter participation in future immunization efforts, even if a vaccine were developed. To mitigate this, policymakers and health professionals must prioritize transparency, acknowledging uncertainties while communicating risks in context. For instance, explaining that severe vaccine side effects occur in fewer than 1 in 1 million cases provides perspective that raw numbers often lack.
Rebuilding trust requires proactive measures, not just reactive corrections. One effective approach is engaging trusted community leaders—religious figures, teachers, or local doctors—to disseminate accurate information. These figures can address cultural or regional concerns that national campaigns might overlook. Additionally, platforms like Facebook and Twitter must enforce stricter policies against misinformation, flagging false claims and promoting verified sources. For individuals, fact-checking before sharing is crucial; tools like the WHO’s myth-busting page offer reliable resources. By fostering a culture of critical thinking and accountability, society can reduce the impact of misinformation and safeguard public trust in life-saving interventions.
Hepatitis A Vaccine: Benefits, Side Effects, and When to Get It
You may want to see also
Frequently asked questions
There is no SARS vaccine currently available or approved for use, as SARS (Severe Acute Respiratory Syndrome) was contained in 2004 and did not require widespread vaccination. Therefore, there are no reported deaths from a SARS vaccine.
While some SARS vaccine candidates were developed and tested in early-stage clinical trials, no fatalities were reported during these studies. The trials were small-scale and focused on safety and immunogenicity, not widespread use.
Since no SARS vaccine has been deployed or widely used, there is no data on indirect or long-term effects, including deaths. The focus shifted to other respiratory viruses like COVID-19, for which vaccines have been developed and monitored.