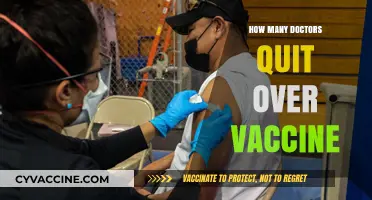
The topic of deaths attributed to childhood vaccines is a subject of significant public interest and scientific scrutiny. While vaccines are widely recognized as one of the most effective public health interventions, saving millions of lives annually, concerns about their safety persist. According to extensive research and data from organizations like the World Health Organization (WHO) and the Centers for Disease Control and Prevention (CDC), serious adverse events, including deaths, from vaccines are extremely rare. Studies indicate that the risk of severe complications or fatalities from vaccine-preventable diseases far outweighs the minimal risks associated with vaccination. For instance, the risk of death from measles is approximately 1 in 1,000 cases, whereas severe reactions to the measles vaccine are estimated at less than 1 in a million doses. Public health experts emphasize that rigorous testing, monitoring, and surveillance systems are in place to ensure vaccine safety, making fatalities from childhood vaccines exceptionally uncommon.
Explore related products




$9.99 $9.99


What You'll Learn
![]()
Historical vaccine-related deaths
The history of vaccination is a testament to human ingenuity, but it is not without its tragic footnotes. Early vaccines, developed in the 18th and 19th centuries, often lacked the rigorous safety standards we expect today. For instance, the first smallpox vaccine, introduced by Edward Jenner in 1796, occasionally caused severe reactions, including bacterial infections at the vaccination site. These complications were not due to the vaccine itself but to the unsanitary conditions under which it was administered. By the mid-20th century, contaminated vaccine batches occasionally led to fatalities. One notable example is the 1955 Cutter incident, where improperly inactivated polio vaccine caused 40,000 cases of polio, including 56 paralytic cases and 5 deaths. Such incidents underscore the critical importance of manufacturing and regulatory oversight in vaccine safety.
Analyzing historical vaccine-related deaths reveals a pattern of risk tied to technological limitations and procedural errors. Early vaccines were often produced using animal tissues, which introduced the risk of contamination with foreign pathogens. For example, the use of monkey kidney cells in early polio vaccines sometimes led to simian virus 40 (SV40) contamination, though its long-term health effects remain debated. Similarly, the diphtheria-tetanus-pertussis (DTP) vaccine, before the acellular version was introduced in the 1990s, was associated with rare but severe adverse events, including high fevers and seizures, leading to a handful of fatalities annually. These cases highlight the tension between the lifesaving benefits of vaccines and the unavoidable, albeit minimal, risks inherent in any medical intervention.
A comparative look at historical vaccine fatalities versus disease mortality provides crucial context. Before the measles vaccine was introduced in 1963, the disease caused approximately 2.6 million deaths annually worldwide. In contrast, severe allergic reactions (anaphylaxis) to the measles vaccine occur at a rate of about 1 in a million doses, with fatalities even rarer. Similarly, smallpox vaccination carried a risk of death of about 1 in a million, yet smallpox itself had a fatality rate of 30%. These comparisons illustrate that the risks of vaccination have always been dwarfed by the dangers of the diseases they prevent. Historical vaccine-related deaths, while tragic, represent a tiny fraction of the lives saved through immunization.
To minimize vaccine-related risks, historical lessons have informed modern practices. For example, the development of purified, cell-culture-based vaccines has virtually eliminated contamination risks. The introduction of the Vaccine Adverse Event Reporting System (VAERS) in the U.S. in 1990 allows for real-time monitoring of potential side effects, enabling swift action when issues arise. Parents and caregivers can further reduce risks by ensuring children are up to date on recommended vaccines, reporting any pre-existing conditions to healthcare providers, and monitoring for severe reactions post-vaccination. While no medical intervention is entirely risk-free, the evolution of vaccine safety protocols has made historical tragedies increasingly rare, reinforcing vaccines as one of the most effective public health tools ever created.
Easy Steps to Register for Your BC Vaccine Passport Online
You may want to see also
Explore related products




$26.59 $32.99


![]()
Reported adverse reactions data
Adverse reactions to childhood vaccines are meticulously tracked through systems like the Vaccine Adverse Event Reporting System (VAERS) in the United States and the Yellow Card scheme in the UK. These databases rely on voluntary submissions from healthcare providers, parents, and individuals, capturing a wide range of symptoms, from mild (e.g., fever, soreness) to severe (e.g., anaphylaxis, seizures). While these systems are vital for monitoring vaccine safety, their data must be interpreted cautiously. Underreporting and lack of verification mean that raw numbers do not equate to causation. For instance, a reported death following vaccination does not automatically imply the vaccine was the cause; it merely indicates a temporal association.
Analyzing reported adverse reactions requires distinguishing between correlation and causation. Epidemiological studies, such as case-control investigations, are often employed to determine whether a specific reaction is directly linked to a vaccine. For example, the rare association between the measles-mumps-rubella (MMR) vaccine and febrile seizures in children aged 12–23 months has been confirmed through such studies. However, these seizures are typically benign and resolve without long-term consequences. Similarly, anaphylaxis, though severe, occurs at a rate of approximately 1.3 cases per million vaccine doses and is treatable with prompt medical intervention.
Transparency in reporting adverse reactions is critical for maintaining public trust in vaccination programs. Health authorities often publish periodic safety updates, summarizing trends and addressing concerns. For instance, the Centers for Disease Control and Prevention (CDC) regularly reviews VAERS data to identify potential signals of risk. When a signal is detected, further investigation is conducted to determine whether the vaccine is indeed the cause. This process ensures that rare but serious adverse events, such as the temporary pause of the Johnson & Johnson COVID-19 vaccine due to rare blood clots, are swiftly addressed.
Practical tips for parents and caregivers include monitoring children for common reactions, such as fever or irritability, following vaccination. Over-the-counter medications like acetaminophen can be used to manage discomfort, but only as directed by a healthcare provider. It is also essential to report any unusual symptoms to a doctor and, if appropriate, to the relevant adverse event reporting system. This proactive approach not only aids in individual care but also contributes to the collective understanding of vaccine safety.
In conclusion, reported adverse reactions data serve as a cornerstone of vaccine safety monitoring, but their interpretation requires nuance. By understanding the limitations of reporting systems, distinguishing between correlation and causation, and staying informed through official updates, stakeholders can navigate this complex topic with confidence. Practical vigilance and reporting participation further strengthen the system, ensuring that childhood vaccines remain one of the safest and most effective public health interventions.
Does Insurance Cover Pneumonia Vaccines? What You Need to Know
You may want to see also
Explore related products






![]()
Vaccine safety studies overview
Childhood vaccines undergo rigorous safety testing before approval, but concerns about adverse events persist. Vaccine safety studies employ diverse methodologies to assess risks, including clinical trials, post-market surveillance, and epidemiological analyses. For instance, the Vaccine Adverse Event Reporting System (VAERS) collects data on potential side effects, while the Vaccine Safety Datalink (VSD) monitors outcomes in large populations. These systems help identify rare events, such as anaphylaxis, which occurs in approximately 1.3 cases per million vaccine doses administered. Understanding these mechanisms is crucial for evaluating claims about vaccine-related deaths.
One critical aspect of vaccine safety studies is the distinction between correlation and causation. Reports of deaths following vaccination often emerge, but causality is rarely established. For example, sudden infant death syndrome (SIDS) has been investigated in relation to vaccines, yet studies consistently show no causal link. A 2003 Institute of Medicine (IOM) report concluded that evidence does not support a connection between vaccines and SIDS. Such findings highlight the importance of interpreting data within a scientific framework rather than relying on anecdotal evidence or temporal associations.
Vaccine safety studies also address specific age categories and dosages to ensure tailored protection. For instance, the MMR (measles, mumps, rubella) vaccine is administered in two doses, typically at 12–15 months and 4–6 years. Studies have confirmed its safety profile, with severe reactions being extremely rare. Similarly, the DTaP (diphtheria, tetanus, pertussis) vaccine, given in a series of five doses starting at 2 months, has been rigorously tested to minimize risks. Parents can enhance safety by following the CDC’s immunization schedule and reporting any unusual symptoms to healthcare providers promptly.
Despite robust evidence supporting vaccine safety, misinformation often amplifies fears. A comparative analysis of vaccine-related deaths versus disease-related deaths underscores the benefits of immunization. For example, measles vaccination has prevented an estimated 25.5 million deaths globally between 2000 and 2018. In contrast, vaccine-related fatalities are exceptionally rare, with no credible evidence linking childhood vaccines to significant mortality rates. This disparity emphasizes the need for public education to combat myths and promote informed decision-making.
Practical tips for parents include staying informed through reputable sources like the CDC or WHO, maintaining open communication with healthcare providers, and monitoring children for common side effects such as fever or soreness. Additionally, understanding the role of adjuvants and preservatives in vaccines can alleviate concerns. For instance, thimerosal, once used in multidose vials, has been removed from most childhood vaccines due to public apprehension, despite no evidence of harm. By engaging with evidence-based information, parents can confidently protect their children through vaccination.
Kennel Cough Vaccine: Protection, Prevention, and Pet Health Essentials
You may want to see also
Explore related products



![Death Becomes Her - Full Frame Edition [DVD]](https://m.media-amazon.com/images/I/81JFyq9rEmL._AC_UY218_.jpg)


![]()
Global mortality statistics analysis
Childhood vaccines save millions of lives annually, yet concerns about vaccine-related deaths persist. Global mortality statistics reveal that such fatalities are exceedingly rare, with estimates suggesting fewer than one death per million doses administered. For context, the measles vaccine, one of the most widely used, has a reported mortality rate of approximately 0.000001%, primarily linked to severe allergic reactions (anaphylaxis). These figures underscore the safety of immunization programs, which prevent roughly 2-3 million deaths each year from diseases like measles, polio, and tetanus.
Analyzing regional disparities highlights the importance of healthcare infrastructure. In low-income countries, vaccine-related deaths are slightly higher due to challenges like improper storage, contaminated equipment, or inadequate medical response to rare adverse events. For instance, the use of multi-dose vials without proper sterilization has historically led to infections in settings with limited resources. In contrast, high-income nations report negligible mortality rates, thanks to stringent safety protocols, single-dose vials, and immediate access to emergency care.
A comparative analysis of vaccine types reveals varying risk profiles. Live-attenuated vaccines, such as the MMR (measles, mumps, rubella), carry a slightly higher risk of adverse events compared to inactivated vaccines like the injectable polio vaccine. However, even for live vaccines, severe outcomes are rare. For example, the risk of developing a serious allergic reaction to the MMR vaccine is approximately 1 in 1 million doses, while the risk of dying from measles itself is 1 in 500 cases in unvaccinated populations.
To minimize risks, healthcare providers must adhere to best practices. Administering vaccines at the correct dosage—typically 0.5 mL for intramuscular injections in infants—and avoiding vaccination in children with severe immunodeficiency or a history of anaphylaxis to vaccine components are critical. Parents should monitor children for 15-30 minutes post-vaccination and seek immediate medical attention for symptoms like difficulty breathing, swelling, or rapid heartbeat.
In conclusion, global mortality statistics affirm that childhood vaccines are among the safest medical interventions. While no medical procedure is entirely risk-free, the benefits of vaccination in preventing deadly diseases far outweigh the rare instances of adverse outcomes. Strengthening healthcare systems globally and maintaining public trust through transparent data sharing are essential to maximizing the lifesaving potential of immunization programs.
Is the Chickenpox Vaccine Live? Understanding Varicella Immunization
You may want to see also
Explore related products




![Death Becomes Her - Collector's Edition 4K Ultra HD + Blu-ray [4K UHD]](https://m.media-amazon.com/images/I/71MFd6R2qRL._AC_UY218_.jpg)
![]()
Common misconceptions debunked
Childhood vaccines save millions of lives annually, yet misinformation persists about their safety. One common myth is that vaccines cause more deaths than the diseases they prevent. Data from the World Health Organization (WHO) and the Centers for Disease Control and Prevention (CDC) consistently show that vaccine-preventable diseases like measles, polio, and whooping cough claim far more lives globally than vaccine-related adverse events. For instance, measles alone caused over 207,500 deaths in 2019, primarily among children under five, while severe reactions to the measles vaccine are exceedingly rare, occurring in fewer than one in a million doses.
Another misconception is that vaccines contain harmful ingredients in dangerous amounts. While it’s true that vaccines may include substances like formaldehyde or aluminum, these are present in trace amounts far below levels that could cause harm. For example, a baby receives more aluminum from breast milk (about 10 milligrams in six months) than from all recommended vaccines combined (4 milligrams by age six). These ingredients serve critical functions, such as preserving the vaccine or enhancing the immune response, and are rigorously tested for safety.
Some claim that vaccines weaken the immune system, leaving children vulnerable to other illnesses. In reality, vaccines strengthen the immune system by training it to recognize and fight specific pathogens. A child’s immune system handles thousands of antigens daily from food, dust, and bacteria, and vaccines add a minuscule fraction to this load. Studies show that vaccinated children are no more likely to develop infections than unvaccinated children, and in fact, they are better protected against life-threatening diseases.
Finally, the idea that natural immunity is superior to vaccine-induced immunity is often touted. While recovering from a disease can provide immunity, this approach carries significant risks. For example, surviving a measles infection can lead to pneumonia, encephalitis, or lifelong disabilities. Vaccines, on the other hand, provide a safer way to build immunity without the dangers of the disease itself. Public health experts agree that the benefits of vaccination far outweigh the risks, making it a cornerstone of preventive medicine.
Practical tip: Always consult reputable sources like the CDC, WHO, or your pediatrician for vaccine information. Avoid relying on anecdotal stories or unverified claims, which can perpetuate myths and endanger public health. Vaccines are one of the most thoroughly tested medical products, with ongoing monitoring to ensure their safety and efficacy. By understanding the facts, parents can make informed decisions to protect their children and communities.
Understanding the Tdap Vaccine: Key Components and Their Functions
You may want to see also
Frequently asked questions
The number of deaths directly attributed to childhood vaccines is extremely rare. According to the Centers for Disease Control and Prevention (CDC) and the World Health Organization (WHO), serious adverse events, including deaths, are estimated to occur in fewer than 1 in a million vaccinations.
No, childhood vaccines are not a leading cause of death in children. Vaccine-related deaths are exceptionally rare, while the diseases prevented by vaccines (e.g., measles, polio, whooping cough) have historically caused significant morbidity and mortality.
Vaccine safety is rigorously monitored through systems like the Vaccine Adverse Event Reporting System (VAERS) and the Vaccine Safety Datalink (VSD). Reported deaths are thoroughly investigated, and the vast majority are found to be unrelated to vaccination. The benefits of vaccines in preventing disease and saving lives far outweigh the minimal risks.
Extensive research has found no causal link between childhood vaccines and SIDS. While some vaccinated infants have tragically died of SIDS, studies show that vaccination does not increase the risk of SIDS. SIDS remains a complex and poorly understood condition with no proven connection to vaccines.




![The Death of Stalin [DVD]](https://m.media-amazon.com/images/I/61kr1OahLBL._AC_UY218_.jpg)