The debate surrounding vaccine safety often includes discussions about the number of deaths attributed to vaccines versus the lives saved by them. While vaccines are rigorously tested and monitored for safety, no medical intervention is entirely risk-free. Reports of adverse events, including rare fatalities, are meticulously documented and investigated by health authorities. However, the number of deaths directly caused by vaccines is extremely low compared to the millions of lives saved annually from preventable diseases. For instance, vaccines have eradicated smallpox and significantly reduced the incidence of polio, measles, and other deadly illnesses. The benefits of vaccination overwhelmingly outweigh the risks, making it one of the most effective public health interventions in history.
Explore related products




$9.99 $9.99


What You'll Learn
- Historical vaccine mortality rates compared to disease-related deaths
- COVID-19 vaccine fatalities versus virus-caused deaths globally
- Adverse reactions leading to death post-vaccination analysis
- Childhood vaccine deaths versus preventable disease fatalities
- Flu vaccine mortality rates compared to influenza deaths annually
![]()
Historical vaccine mortality rates compared to disease-related deaths
Vaccine-related deaths are exceedingly rare, with historical data showing rates often below 1 in a million doses administered. For instance, the smallpox vaccine, one of the earliest and most impactful vaccines, had a fatality rate of approximately 1 to 2 per million vaccinations. In stark contrast, smallpox itself killed roughly 30% of those infected, highlighting the vast disparity in risk between vaccination and disease exposure. This comparison underscores the critical role vaccines have played in reducing mortality on a global scale.
Consider the measles vaccine, introduced in the 1960s, which has saved an estimated 20 million lives worldwide. Severe adverse reactions, including death, occur in fewer than 1 in a million doses. Meanwhile, measles carries a fatality rate of 1 to 3 per 1,000 cases, particularly in young children and immunocompromised individuals. This disparity illustrates the life-saving efficacy of vaccines, even when accounting for the minuscule risks associated with their administration. Parents and caregivers should note that timely vaccination, following the CDC’s recommended schedule (e.g., MMR vaccine at 12-15 months and 4-6 years), maximizes protection while minimizing risk.
Historical outbreaks provide further context. During the 1950s polio epidemic, the disease paralyzed or killed over 15,000 Americans annually. The introduction of the polio vaccine reduced cases by 99% within two decades, with vaccine-related deaths occurring in fewer than 1 in 10 million doses. To put this in perspective, the risk of paralysis from polio infection was 1 in 200 for children, making vaccination the safer choice by orders of magnitude. Modern inactivated polio vaccines (IPV) further eliminate the rare risk of vaccine-associated paralytic polio seen in earlier oral formulations.
Critics often cite the 1976 swine flu vaccine campaign, where 25 deaths were linked to Guillain-Barré syndrome (GBS) out of 45 million vaccinations. While tragic, this event remains an outlier, and subsequent vaccines have undergone rigorous safety testing to prevent recurrence. Compare this to the 1918 influenza pandemic, which killed 50 million globally, or even seasonal flu, which causes 12,000 to 52,000 U.S. deaths annually despite vaccine availability. Annual flu vaccination, particularly for high-risk groups like pregnant women and those over 65, remains a cornerstone of public health, with serious side effects occurring in less than 1 in a million doses.
In summary, historical data consistently demonstrates that the mortality risk from vaccine-preventable diseases far exceeds the rare risks associated with vaccination. From smallpox to COVID-19, vaccines have saved millions of lives, with adverse events occurring at rates often lower than natural background risks (e.g., lightning strikes or car accidents). Public health officials emphasize informed decision-making, leveraging resources like the Vaccine Adverse Event Reporting System (VAERS) and clinical trials to ensure ongoing safety. By focusing on evidence, individuals can make choices that protect both personal and community health.
Quezon City Vaccination Registration: A Step-by-Step Guide for Residents
You may want to see also
Explore related products


$29.95 $25.48




![]()
COVID-19 vaccine fatalities versus virus-caused deaths globally
The COVID-19 pandemic has starkly highlighted the life-saving impact of vaccines, but it has also fueled debates about their safety. A critical comparison emerges when examining fatalities directly linked to COVID-19 vaccines versus deaths caused by the virus itself. Data from global health organizations, including the World Health Organization (WHO) and the Centers for Disease Control and Prevention (CDC), reveal a profound disparity. As of late 2023, COVID-19 has claimed over 6.5 million lives globally, with millions more suffering severe complications. In contrast, vaccine-related deaths are exceedingly rare, estimated at fewer than 0.004% of administered doses, primarily involving severe allergic reactions (anaphylaxis) or rare conditions like thrombosis with thrombocytopenia syndrome (TTS) associated with adenovirus vector vaccines.
Analyzing the risk-benefit ratio provides clarity. For instance, the Pfizer-BioNTech and Moderna mRNA vaccines, administered in billions of doses, have anaphylaxis rates of approximately 2 to 5 cases per million doses. Even for the Johnson & Johnson vaccine, linked to TTS, the risk is approximately 7 per 1 million doses in women aged 18–49. These figures pale in comparison to the 0.5% to 1% mortality rate of COVID-19 infections, which increases significantly for older adults and those with comorbidities. A 65-year-old with hypertension, for example, faces a 10% mortality risk if infected, whereas their risk from vaccination is virtually negligible.
Practical considerations underscore the importance of vaccination. Health agencies recommend specific precautions, such as monitoring for 15–30 minutes post-vaccination to address immediate reactions. For those with a history of severe allergies, consulting an allergist before vaccination is advised. Additionally, the CDC emphasizes that the benefits of vaccination far outweigh the risks, particularly for vulnerable populations. For instance, a single dose of the Pfizer vaccine reduces severe illness risk by 80% in individuals over 65, a statistic that has driven global vaccination campaigns.
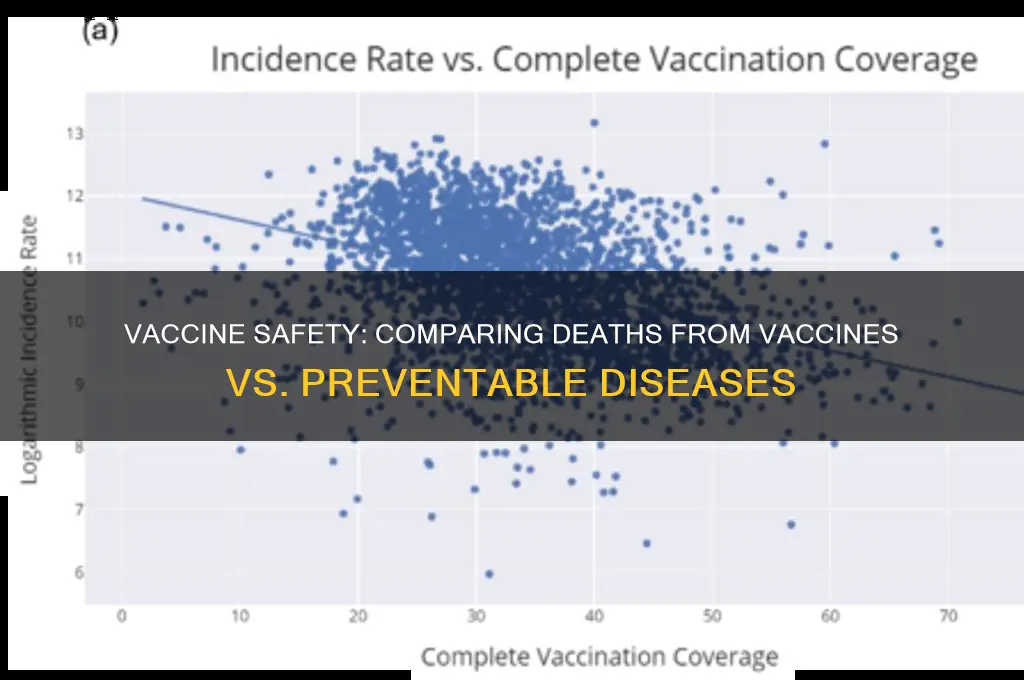
Comparatively, the societal impact of vaccine hesitancy due to safety concerns cannot be overlooked. In regions with low vaccination rates, COVID-19 continues to overwhelm healthcare systems, causing preventable deaths. For example, countries with less than 30% vaccination coverage experienced mortality rates 50 times higher than those with 70% coverage during the Omicron wave. This disparity highlights the indirect consequences of misinformation, which often exaggerates vaccine risks while downplaying the virus’s lethality.
In conclusion, the data unequivocally demonstrates that COVID-19 vaccines are a vital tool in reducing mortality, with fatalities from vaccination being exceptionally rare compared to deaths caused by the virus. By focusing on evidence-based information and following health guidelines, individuals can make informed decisions that protect both personal and public health. The pandemic’s trajectory underscores a clear message: vaccines save lives, and their risks are minuscule in comparison to the threat they mitigate.
Vaccine Approval: FDA's Role and Importance
You may want to see also
Explore related products






![]()
Adverse reactions leading to death post-vaccination analysis
Vaccine safety monitoring systems, such as the Vaccine Adverse Event Reporting System (VAERS) in the United States and the Yellow Card scheme in the UK, play a crucial role in identifying potential adverse reactions post-vaccination. These systems rely on healthcare professionals and the public to report any suspected side effects, including severe cases leading to hospitalization or death. While these reports are essential for signal detection, they do not inherently prove causation. For instance, a reported death following vaccination could be coincidental, especially in elderly populations where mortality rates are higher due to pre-existing conditions. Analyzing these reports involves rigorous statistical methods and clinical reviews to differentiate between correlation and causation, ensuring that public trust in vaccination programs remains intact.
Consider the case of anaphylaxis, a rare but severe allergic reaction that can occur within minutes to hours after vaccination. For mRNA COVID-19 vaccines, the incidence of anaphylaxis is estimated at approximately 2 to 5 cases per million doses administered. While fatalities from vaccine-induced anaphylaxis are exceedingly rare, they highlight the importance of post-vaccination observation periods and immediate access to emergency medical care. Healthcare providers are instructed to monitor patients for at least 15–30 minutes post-injection, particularly those with a history of severe allergies. This proactive approach minimizes risks and ensures prompt intervention if an adverse reaction occurs.
Another critical aspect of post-vaccination death analysis is the examination of age-specific risks. For example, the rare association between adenovirus vector-based COVID-19 vaccines (e.g., AstraZeneca and Johnson & Johnson) and vaccine-induced immune thrombotic thrombocytopenia (VITT) has been observed predominantly in younger adults, particularly women under 50. VITT is a condition characterized by blood clots combined with low platelet counts, and while treatable if identified early, it has led to fatalities in a small number of cases. As a result, many countries have adjusted their vaccination guidelines, recommending alternative vaccines for younger age groups. This example underscores the need for tailored vaccine strategies based on demographic risk profiles.
To conduct a comprehensive analysis of adverse reactions leading to death, researchers employ pharmacovigilance tools such as disproportionality analysis and case-control studies. Disproportionality analysis compares the observed frequency of a specific adverse event to its expected frequency, helping identify potential safety signals. For instance, if deaths reported post-vaccination are disproportionately higher for a particular vaccine-event pair, further investigation is warranted. Case-control studies, on the other hand, compare individuals who experienced the adverse event to those who did not, controlling for confounding factors. These methodologies, combined with clinical expertise, enable a nuanced understanding of vaccine-related mortality risks.
Practical tips for healthcare providers and the public include staying informed about vaccine safety updates from reputable sources, such as the World Health Organization (WHO) or national health agencies. Individuals should disclose their full medical history before vaccination to help providers assess potential risks. In the event of an adverse reaction, timely reporting to national surveillance systems is crucial for ongoing safety monitoring. Finally, maintaining perspective is essential: while adverse reactions leading to death are tragic, they remain extremely rare compared to the millions of lives saved through vaccination. Evidence-based communication and transparency are key to addressing concerns and upholding public confidence in immunization programs.
When Should Kids Get Measles Vaccines: A Parent's Guide
You may want to see also
Explore related products






![]()
Childhood vaccine deaths versus preventable disease fatalities
Vaccine safety is a cornerstone of public health, yet concerns about adverse effects persist, particularly regarding childhood immunizations. Data from the Centers for Disease Control and Prevention (CDC) and the World Health Organization (WHO) consistently show that serious vaccine-related deaths are exceedingly rare. For instance, the Vaccine Adverse Event Reporting System (VAERS) records fewer than one death per million vaccine doses administered annually. These fatalities are often linked to severe, pre-existing conditions or rare allergic reactions, such as anaphylaxis, which occurs in approximately 1 in a million doses. In contrast, the diseases vaccines prevent—like measles, pertussis, and polio—historically claimed millions of lives annually, particularly among children under five.
Consider measles, a highly contagious virus that once caused over 2.6 million deaths per year before widespread vaccination. In 2020, global measles fatalities dropped to around 73,000, largely due to immunization efforts. However, vaccine hesitancy has led to resurgence in some regions, with outbreaks disproportionately affecting unvaccinated children. For example, a 2019 outbreak in Samoa resulted in 83 deaths, primarily among infants too young to receive the MMR vaccine. This stark contrast highlights the life-saving impact of vaccines and the deadly consequences of preventable diseases.
Analyzing the risk-benefit ratio further underscores the importance of childhood vaccination. While no medical intervention is entirely risk-free, the likelihood of a fatal outcome from a vaccine is minuscule compared to the mortality rates of the diseases they prevent. For instance, the fatality rate for measles is approximately 0.2% globally, meaning 1 in 500 unvaccinated children who contract the virus will die. In comparison, the risk of death from the MMR vaccine is virtually nonexistent, with no causal link established between the vaccine and fatalities in healthy individuals. This data-driven perspective is crucial for parents weighing the risks of vaccination against the dangers of vaccine-preventable diseases.
Practical steps can help mitigate rare vaccine-related risks while maximizing protection. Ensure children receive vaccines at the recommended ages, typically starting at 2 months, to align with their developing immune systems. Monitor for mild side effects, such as fever or soreness, which are normal and resolve within days. For children with known allergies or medical conditions, consult a pediatrician before vaccination to assess potential risks. Finally, stay informed through reputable sources like the CDC or WHO, avoiding misinformation that often exaggerates vaccine dangers. By focusing on evidence, parents can make informed decisions that prioritize their child’s health and contribute to community immunity.
In conclusion, the comparison between childhood vaccine deaths and preventable disease fatalities reveals a clear disparity. While vaccines carry a negligible risk of severe outcomes, the diseases they prevent remain significant threats to child health. By understanding this balance and following best practices, families can confidently embrace vaccination as a vital tool in safeguarding lives.
Pfizer Vaccine Deaths: Separating Facts from Misinformation and Fears
You may want to see also
Explore related products






![]()
Flu vaccine mortality rates compared to influenza deaths annually
The flu vaccine is a cornerstone of public health, yet its mortality rate is often misunderstood. Data from the Centers for Disease Control and Prevention (CDC) show that severe adverse reactions to the flu vaccine are exceedingly rare, with anaphylaxis occurring in approximately 1.3 cases per million doses administered. In contrast, influenza itself claims tens of thousands of lives annually in the United States alone, with the CDC estimating 12,000 to 52,000 deaths each year depending on the severity of the flu season. This stark disparity highlights the vaccine’s safety profile compared to the risks of the disease it prevents.
Consider the age-specific impact of influenza versus the flu vaccine. For older adults, aged 65 and above, influenza is particularly deadly, accounting for up to 90% of flu-related deaths. The flu vaccine, while not 100% effective, significantly reduces the risk of severe illness and hospitalization in this demographic. Studies indicate that vaccinated older adults are 40-70% less likely to be hospitalized for flu-related complications compared to their unvaccinated peers. Meanwhile, vaccine-related deaths in this age group are virtually nonexistent, with no documented cases directly attributed to the vaccine itself.
For parents weighing the risks, the flu vaccine is a critical tool in protecting children. Pediatric influenza deaths average around 100 annually in the U.S., with children under 5 facing the highest risk. The vaccine’s side effects in this age group are typically mild—fever, soreness, or fatigue—and severe reactions are extremely rare. For example, the Vaccine Adverse Event Reporting System (VAERS) records fewer than 100 serious adverse events annually among millions of pediatric doses administered, none of which are consistently linked to mortality. This underscores the vaccine’s safety compared to the tangible threat of influenza.
Practical steps can maximize the flu vaccine’s benefits while minimizing concerns. First, ensure you or your child receive the vaccine from a reputable healthcare provider, who can address specific health conditions or allergies. Second, monitor for mild side effects, such as arm soreness or low-grade fever, which typically resolve within 48 hours. Finally, stay informed about the flu’s prevalence in your area through local health department updates, as this can help you understand the urgency of vaccination. By framing the decision in terms of risk comparison, the choice becomes clear: the flu vaccine’s mortality rate is negligible, while influenza’s annual death toll is a preventable tragedy.
Hepatitis A Vaccine at Birth: Origins and Implementation Timeline
You may want to see also
Frequently asked questions
The number of deaths directly caused by vaccines is extremely low. According to the CDC and WHO, serious adverse events, including deaths, are rare, with estimates ranging from 1 to 2 deaths per million vaccine doses administered.
Deaths from vaccine-preventable diseases far exceed those from vaccines. For example, before widespread vaccination, diseases like measles, polio, and influenza caused millions of deaths globally annually, whereas vaccine-related fatalities are negligible in comparison.
Yes, reliable data from health organizations like the CDC, WHO, and peer-reviewed studies show that vaccines save millions of lives annually, while vaccine-related deaths are exceedingly rare, typically occurring in fewer than 0.001% of recipients.