Vaccines for bacterial diseases have been a cornerstone of public health, significantly reducing the incidence of once-devastating illnesses such as tuberculosis, diphtheria, tetanus, and pertussis. These vaccines work by stimulating the immune system to recognize and combat specific bacterial pathogens, either by introducing inactivated or weakened bacteria, toxin components, or specific antigens. Unlike viral vaccines, which often target the virus itself, bacterial vaccines frequently focus on neutralizing toxins produced by the bacteria or preventing their colonization. While highly effective, the development of bacterial vaccines faces unique challenges, including bacterial diversity, antibiotic resistance, and the complexity of bacterial structures. Despite these hurdles, ongoing research continues to expand the arsenal of bacterial vaccines, offering hope for controlling emerging threats and improving global health outcomes.
| Characteristics | Values |
|---|---|
| Definition | Vaccines designed to prevent bacterial infections by stimulating immunity. |
| Mechanism | Use inactivated/attenuated bacteria, toxoids, or bacterial components. |
| Examples | Tuberculosis (BCG), Tetanus, Diphtheria, Pertussis, Pneumococcal, Meningococcal, Typhoid, Cholera. |
| Types | Live-attenuated, Inactivated, Subunit/Conjugate, Toxoid, mRNA (emerging). |
| Administration | Injected (IM/SC), Oral, Intranasal (depending on vaccine). |
| Efficacy | Varies by vaccine; e.g., Tdap (90%+), Typhoid (50-80%), BCG (variable). |
| Duration of Protection | Varies; e.g., Tetanus (10 years), Pneumococcal (5-10 years), BCG (variable). |
| Side Effects | Mild: Pain, redness, fever; Rare: Severe allergic reactions. |
| Global Impact | Significantly reduced morbidity/mortality from bacterial diseases. |
| Challenges | Antibiotic resistance, Vaccine hesitancy, Access in low-income regions. |
| Research Focus | Developing vaccines for antibiotic-resistant bacteria (e.g., MRSA, TB). |
| Latest Advances | mRNA vaccines for bacterial infections, Broad-spectrum vaccines. |
Explore related products






What You'll Learn
- Vaccine Types: Conjugate, subunit, toxoid, live attenuated, and polysaccharide vaccines explained
- Common Bacterial Vaccines: Vaccines for TB, tetanus, diphtheria, pertussis, and pneumococcal diseases
- Vaccine Development: Process from identification to clinical trials and approval
- Efficacy and Safety: Effectiveness, side effects, and long-term immunity of bacterial vaccines
- Global Impact: Role in reducing bacterial disease prevalence and mortality worldwide
![]()
Vaccine Types: Conjugate, subunit, toxoid, live attenuated, and polysaccharide vaccines explained
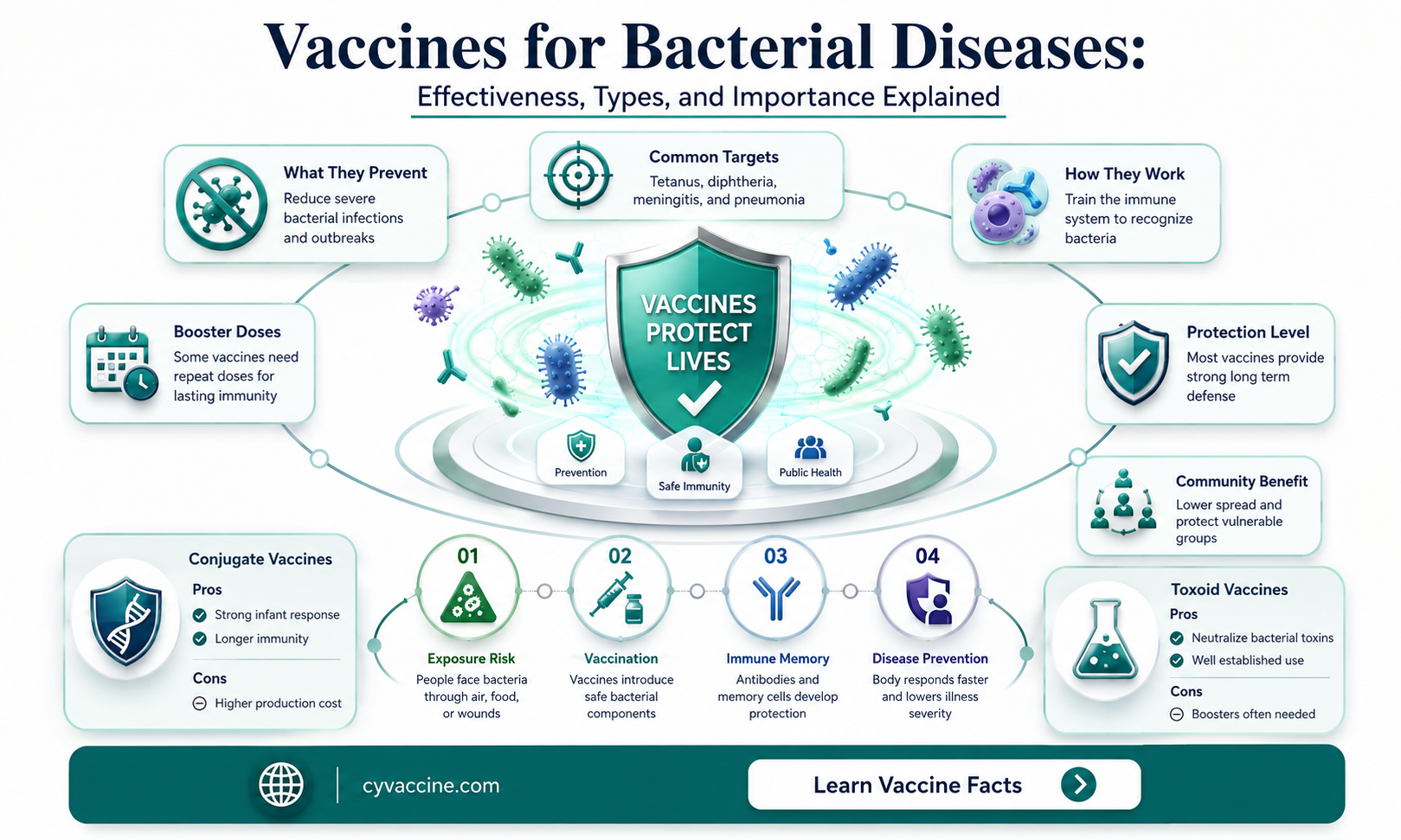
Bacterial diseases have long been a target for vaccine development, and the arsenal of vaccines available today reflects a sophisticated understanding of bacterial pathogenesis. Among these, conjugate, subunit, toxoid, live attenuated, and polysaccharide vaccines stand out for their unique mechanisms and applications. Each type is tailored to address specific challenges posed by bacterial infections, from eliciting robust immune responses in young children to neutralizing potent toxins. Understanding these vaccine types is crucial for appreciating how they protect against diseases like meningitis, pertussis, and tetanus.
Conjugate vaccines are a cornerstone in combating bacterial infections, particularly in infants and young children. These vaccines combine a weak antigen (a polysaccharide from the bacterial capsule) with a strong antigen (a protein carrier) to enhance the immune response. For example, the Haemophilus influenzae type b (Hib) conjugate vaccine has drastically reduced meningitis cases in children under 5. Administered in a series of doses starting at 2 months of age, it primes the immature immune system to recognize and attack the bacterium. The success of conjugate vaccines lies in their ability to induce immunological memory, ensuring long-term protection against invasive bacterial diseases.
Subunit and toxoid vaccines, on the other hand, focus on specific components of bacteria rather than the whole organism. Subunit vaccines use fragments of the pathogen, such as proteins or peptides, to trigger an immune response. The acellular pertussis vaccine (DTaP), for instance, contains purified antigens from Bordetella pertussis, reducing the risk of side effects compared to whole-cell vaccines. Toxoid vaccines, like the tetanus and diphtheria toxoids, neutralize harmful bacterial toxins by using inactivated versions of them. These vaccines are typically administered in combination (e.g., Tdap for adolescents and adults) and require booster doses every 10 years to maintain immunity.
Live attenuated vaccines offer a unique approach by using weakened but still living bacteria to stimulate a strong immune response. The Bacillus Calmette-Guérin (BCG) vaccine, used against tuberculosis, is a prime example. While not universally effective, it provides significant protection in regions with high TB prevalence. Live attenuated vaccines mimic natural infection, often conferring lifelong immunity with just one or two doses. However, they are contraindicated in immunocompromised individuals due to the risk of the attenuated pathogen causing disease.
Polysaccharide vaccines target the sugar-based capsules surrounding certain bacteria, such as Streptococcus pneumoniae and Neisseria meningitidis. These vaccines are particularly effective in adults but less so in young children, whose immune systems struggle to respond to polysaccharide antigens alone. To address this, polysaccharide-protein conjugate vaccines (e.g., PCV13 for pneumococcus) have been developed, offering improved efficacy across all age groups. Polysaccharide vaccines are often recommended for older adults and individuals with specific medical conditions, such as asplenia, to prevent severe bacterial infections.
In practice, the choice of vaccine type depends on the bacterial target, the age and health of the recipient, and the desired duration of immunity. For instance, conjugate vaccines are ideal for infants, while toxoid vaccines are essential for maintaining immunity in adults. Live attenuated vaccines provide robust protection but require careful consideration of safety. Polysaccharide vaccines, though less immunogenic in children, remain vital for preventing diseases in at-risk populations. By leveraging these diverse vaccine types, public health efforts can effectively combat bacterial diseases, saving millions of lives worldwide.
BCG Vaccine: How It Boosts Immunity Against TB Bacteria
You may want to see also
Explore related products






![]()
Common Bacterial Vaccines: Vaccines for TB, tetanus, diphtheria, pertussis, and pneumococcal diseases
Bacterial infections, once leading causes of mortality, have been significantly curbed through vaccination. Among the most impactful are vaccines targeting tuberculosis (TB), tetanus, diphtheria, pertussis, and pneumococcal diseases. Each of these vaccines operates uniquely, addressing specific pathogens and their modes of transmission, yet collectively they exemplify the power of immunization in preventing severe bacterial illnesses.
Consider the Bacillus Calmette-Guérin (BCG) vaccine for TB, primarily administered to infants in high-incidence regions. While it doesn’t prevent all forms of TB, it significantly reduces the risk of severe, disseminated disease in children. Its efficacy varies geographically, but its role in early childhood protection is undisputed. In contrast, the tetanus vaccine, often given as part of the DTaP (diphtheria, tetanus, pertussis) series, requires booster doses every 10 years for adults. Tetanus, caused by *Clostridium tetani*, is not contagious but enters the body through wounds, making vaccination a critical preventive measure. A single dose of tetanus toxoid (0.5 mL intramuscularly) is recommended for wound management if vaccination status is unclear.
Diphtheria and pertussis vaccines are typically combined in formulations like DTaP for children and Tdap for adolescents and adults. Diphtheria, a respiratory infection caused by *Corynebacterium diphtheriae*, can lead to pseudomembrane formation in the throat, while pertussis (whooping cough) causes severe, prolonged coughing fits. The CDC recommends DTaP doses at 2, 4, 6, and 15–18 months, followed by a booster at 4–6 years. For adults, a Tdap dose replaces one tetanus booster, offering continued protection against all three diseases. Pregnant individuals are advised to receive Tdap during each pregnancy to protect newborns, who are too young to be vaccinated.
Pneumococcal vaccines, such as PCV13 (Prevnar 13) and PPSV23 (Pneumovax 23), target *Streptococcus pneumoniae*, a leading cause of pneumonia, meningitis, and sepsis. PCV13 is recommended for children under 2 years, administered in a 4-dose series (at 2, 4, 6, and 12–15 months), while PPSV23 is used for adults over 65 and immunocompromised individuals. Adults with risk factors may receive both vaccines, spaced 8 weeks apart, to broaden protection against pneumococcal serotypes.
In summary, these bacterial vaccines differ in their mechanisms, schedules, and target populations, but share a common goal: preventing life-threatening diseases. Adherence to recommended dosages and timing is crucial, as is awareness of booster requirements. By understanding these specifics, individuals and healthcare providers can maximize the benefits of vaccination, reducing morbidity and mortality from these bacterial infections.
Upholding Parental Trust in Vaccines Amidst Misinformation and Challenges
You may want to see also
Explore related products






![]()
Vaccine Development: Process from identification to clinical trials and approval
Bacterial diseases, such as tuberculosis, pertussis, and pneumococcal pneumonia, pose significant global health challenges, making the development of effective vaccines critical. The journey from identifying a bacterial target to a fully approved vaccine is complex, involving multiple stages of research, testing, and regulatory scrutiny. This process ensures that vaccines are both safe and efficacious before they reach the public.
Step 1: Identification and Target Selection
The first step in vaccine development is identifying the bacterial pathogen and its specific antigens—components of the bacterium that trigger an immune response. For example, the *Streptococcus pneumoniae* vaccine targets the bacterium’s polysaccharide capsule, which varies across strains. Researchers analyze disease prevalence, severity, and existing treatment gaps to prioritize targets. This stage often involves genomic studies and epidemiological data to understand the pathogen’s evolution and transmission patterns.
Step 2: Preclinical Development and Testing
Once a target is selected, scientists develop vaccine candidates using various approaches, such as live-attenuated, inactivated, subunit, or conjugate vaccines. For instance, the *Haemophilus influenzae type b* (Hib) vaccine uses a conjugate design, linking the bacterium’s polysaccharide to a protein carrier to enhance immune response in infants. Preclinical testing in animals evaluates safety, immunogenicity, and efficacy. Dosage levels are refined, often starting with microgram quantities, to balance potency and side effects.
Step 3: Clinical Trials: Phases I–III
Clinical trials are conducted in three phases. Phase I trials involve small groups (20–100 volunteers) to assess safety, dosage, and immune response. Phase II expands to several hundred participants to evaluate efficacy and side effects. For bacterial vaccines, this phase often includes specific age groups, such as infants for the Hib vaccine or older adults for the pneumococcal vaccine. Phase III trials involve thousands of participants to confirm efficacy, monitor rare side effects, and compare the vaccine to a placebo or existing vaccine. For example, the meningococcal vaccine’s Phase III trial demonstrated 90% efficacy in adolescents with a standard 0.5 mL intramuscular dose.
Regulatory Review and Approval
After successful clinical trials, manufacturers submit data to regulatory bodies like the FDA or EMA for approval. These agencies review safety, quality, and efficacy data, ensuring manufacturing standards are met. Post-approval, Phase IV trials (pharmacovigilance) monitor long-term effects in the general population. Practical tips for healthcare providers include adhering to storage guidelines (e.g., 2–8°C for most vaccines) and following age-specific dosing schedules, such as the 2-dose series for the Tdap vaccine in adolescents.
Challenges and Innovations
Developing bacterial vaccines faces challenges like antigenic diversity (e.g., *Neisseria gonorrhoeae*) and antimicrobial resistance. Innovations like mRNA technology and adjuvants are being explored to improve efficacy. For instance, the *Shingrix* vaccine uses a recombinant protein and adjuvant system to achieve 90% efficacy in adults over 50. Comparative studies show that conjugate vaccines, like PCV13, provide broader protection than earlier polysaccharide vaccines by inducing T-cell-dependent immunity.
This structured process ensures that bacterial vaccines are rigorously tested and safe, offering practical solutions to combat infectious diseases globally.
Over-Vaccination in Children: Risks, Effects, and What Parents Need to Know
You may want to see also
Explore related products






![]()
Efficacy and Safety: Effectiveness, side effects, and long-term immunity of bacterial vaccines
Bacterial vaccines have proven to be highly effective in preventing diseases such as tetanus, diphtheria, and pertussis, with efficacy rates often exceeding 85%. For instance, the Tdap vaccine, which protects against all three diseases, is recommended for adolescents and adults every 10 years, providing robust immunity. However, effectiveness can vary depending on factors like age, underlying health conditions, and the specific vaccine formulation. Understanding these nuances is crucial for maximizing protection.
Side effects of bacterial vaccines are generally mild and short-lived, including soreness at the injection site, fever, and fatigue. For example, the pneumococcal conjugate vaccine (PCV13), administered to infants and young children in a series of four doses, may cause irritability or decreased appetite in some recipients. Serious adverse reactions are rare, occurring in less than 1 in a million cases. Healthcare providers often advise applying a cool compress to the injection site and administering acetaminophen for discomfort, ensuring a smoother vaccination experience.
Long-term immunity is a critical aspect of bacterial vaccines, though it varies by disease. Vaccines like the one for tetanus require booster shots every decade to maintain protection, while others, such as the meningococcal vaccine, may provide immunity for up to 5 years. Research into conjugate vaccines, which link a weak antigen to a strong one, has significantly improved long-term responses, particularly in vulnerable populations like the elderly. Monitoring antibody levels through titers can help determine when a booster is necessary.
Comparatively, bacterial vaccines often outperform their antiviral counterparts in terms of durability and efficacy due to the stable nature of bacterial antigens. For example, the Haemophilus influenzae type b (Hib) vaccine has nearly eradicated Hib meningitis in countries with high vaccination rates, a feat unmatched by many viral vaccines. This highlights the importance of continued investment in bacterial vaccine research and development to address emerging strains and improve global health outcomes.
Practical tips for ensuring optimal vaccine efficacy include adhering to recommended schedules, especially for multi-dose series like the HPV vaccine, which requires three doses over 6 months for full protection. Parents should keep a vaccination record for their children, and adults should consult their healthcare provider to stay up-to-date. Additionally, maintaining a healthy lifestyle—adequate sleep, nutrition, and hydration—can enhance the immune response to vaccines, further bolstering their effectiveness.
Understanding Legal Requirements for Childhood Vaccinations: Rights and Responsibilities
You may want to see also
Explore related products






![]()
Global Impact: Role in reducing bacterial disease prevalence and mortality worldwide
Bacterial diseases have historically been a leading cause of morbidity and mortality worldwide, but the advent and widespread use of vaccines have dramatically altered this landscape. Vaccines such as those for *Streptococcus pneumoniae* (pneumococcus), *Haemophilus influenzae type b* (Hib), and *Mycobacterium tuberculosis* (BCG) have played a pivotal role in reducing the global burden of bacterial infections. For instance, the pneumococcal conjugate vaccine (PCV) has been shown to reduce invasive pneumococcal disease by up to 90% in children under 5 years old, a demographic particularly vulnerable to this infection. This success underscores the transformative power of vaccination in combating bacterial pathogens.
Consider the case of Hib, a bacterium once responsible for millions of childhood deaths annually from meningitis and pneumonia. The introduction of the Hib vaccine in the 1990s led to a near-elimination of Hib-related diseases in countries with high vaccination coverage. In the United States, for example, Hib cases dropped from 20,000 per year in the pre-vaccine era to fewer than 100 annually. This dramatic reduction highlights the vaccine's efficacy and its role in reshaping global health outcomes. However, disparities in access to such vaccines persist, particularly in low-income countries, where bacterial diseases remain a significant threat.
To maximize the global impact of bacterial vaccines, targeted strategies are essential. For instance, the World Health Organization (WHO) recommends a 3-dose schedule of PCV for infants, typically administered at 6, 10, and 14 weeks of age, with a booster dose in some regions. Similarly, the BCG vaccine, while primarily used to prevent severe forms of tuberculosis in children, requires careful administration via intradermal injection to ensure efficacy. Public health initiatives must also address logistical challenges, such as cold chain maintenance and community education, to ensure vaccines reach those most in need. Without such efforts, the potential of these vaccines to reduce bacterial disease prevalence and mortality will remain unrealized in many parts of the world.
A comparative analysis of vaccine-preventable bacterial diseases reveals both successes and areas for improvement. While diseases like tetanus and diphtheria have been largely controlled through vaccination, others like typhoid fever and cholera continue to pose challenges due to limited vaccine availability and low uptake in endemic regions. For example, the typhoid conjugate vaccine (TCV) offers longer-lasting protection compared to older polysaccharide vaccines but is not yet widely implemented in high-burden countries. By prioritizing the development and distribution of such vaccines, the global health community can further reduce the toll of bacterial diseases on vulnerable populations.
Ultimately, the role of bacterial vaccines in reducing disease prevalence and mortality is undeniable, but their full potential remains untapped. Practical steps, such as integrating bacterial vaccines into routine immunization programs, leveraging technology for vaccine delivery, and fostering international collaboration, can amplify their impact. For individuals, staying informed about recommended vaccines and adhering to immunization schedules is crucial. For policymakers, investing in vaccine research, infrastructure, and equitable distribution is imperative. Together, these efforts can pave the way for a future where bacterial diseases no longer claim millions of lives annually.
Vaccines: The Greatest Medical Breakthrough Saving Lives Globally
You may want to see also
Frequently asked questions
No, vaccines are not available for all bacterial diseases. While vaccines exist for some common bacterial infections like tetanus, diphtheria, pertussis, and pneumococcal disease, many bacterial pathogens still lack effective vaccines due to scientific and developmental challenges.
Vaccines for bacterial diseases typically work by introducing a harmless component of the bacterium (e.g., a protein, toxin, or weakened/killed bacteria) to the immune system. This triggers the production of antibodies and immune memory, preparing the body to fight off the actual bacterium if exposed in the future.
No, vaccines for bacterial diseases cannot cause the illness they are designed to prevent. Most bacterial vaccines use inactivated or purified components of the bacteria, which cannot cause infection. In rare cases, vaccines with weakened bacteria (e.g., BCG for tuberculosis) may cause mild symptoms but not the full-blown disease.