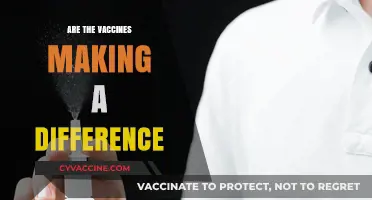
The question of whether vaccines are part of a clinical trial is a common concern, often fueled by misinformation and misunderstanding of the vaccine development and approval process. Vaccines undergo rigorous testing in multiple phases of clinical trials before they are approved for public use, ensuring their safety and efficacy. These trials involve thousands of volunteers and are closely monitored by regulatory bodies such as the FDA, CDC, and WHO. Once approved, vaccines continue to be monitored through post-market surveillance to detect any rare side effects. Therefore, by the time vaccines are administered to the public, they are no longer considered part of a clinical trial but rather a proven and essential tool in preventing diseases.
| Characteristics | Values |
|---|---|
| Vaccine Development Stage | Completed clinical trials and authorized for emergency/full use |
| Clinical Trial Phases Completed | Phase 1 (Safety), Phase 2 (Efficacy), Phase 3 (Large-scale testing) |
| Regulatory Approval Status | Emergency Use Authorization (EUA) or Full Approval by agencies like FDA, EMA, WHO |
| Trial Participants (Phase 3) | Tens of thousands (e.g., Pfizer-BioNTech: ~44,000, Moderna: ~30,000) |
| Efficacy Rates (Phase 3) | Pfizer-BioNTech: 95%, Moderna: 94.1%, AstraZeneca: 70-90% (varies by dose), Johnson & Johnson: 66-72% |
| Safety Monitoring | Ongoing post-authorization surveillance (e.g., VAERS, V-safe) |
| Long-Term Follow-Up | Typically 2 years post-vaccination for full approval |
| Current Status | No longer in clinical trial phase; widely distributed globally |
| Booster Recommendations | Authorized for specific populations based on waning immunity and variant emergence |
| Adverse Events Reporting | Rare but monitored (e.g., myocarditis, blood clots) |
Explore related products

$23.6 $32.99





What You'll Learn
![]()
Vaccine Safety Protocols
Vaccine development is a rigorous process, but public concern often centers on whether widespread vaccination constitutes an ongoing clinical trial. To address this, Vaccine Safety Protocols are implemented as a multi-layered system designed to ensure safety at every stage, from pre-clinical studies to post-market surveillance. These protocols include phased clinical trials, regulatory approvals, and continuous monitoring systems like the Vaccine Adverse Event Reporting System (VAERS) in the U.S. and the Yellow Card scheme in the U.K. For instance, during the COVID-19 pandemic, mRNA vaccines underwent Phase 3 trials involving tens of thousands of participants, with strict adherence to dosage regimens (e.g., 30 µg of Pfizer-BioNTech’s vaccine per dose) and age-specific guidelines (initially approved for ages 16+ before expanding to younger groups).
Consider the phases of clinical trials as a cornerstone of safety protocols. Phase 1 trials focus on dosage safety and immunogenicity in small groups (20–100 volunteers), while Phase 2 expands to several hundred to assess efficacy and side effects. Phase 3 involves thousands to confirm effectiveness and monitor rare adverse events. For example, the Moderna vaccine’s Phase 3 trial included 30,000 participants, with half receiving a placebo, ensuring statistically significant safety data. Post-approval, Phase 4 surveillance tracks long-term effects in the general population. This structured approach ensures vaccines meet safety thresholds before public distribution, debunking the notion that vaccination is an uncontrolled experiment.
Practical post-vaccination safety measures are equally critical. Individuals are advised to wait 15–30 minutes post-injection for observation of immediate reactions, such as anaphylaxis, which occurs in approximately 2–5 cases per million doses. Healthcare providers follow protocols like the Centers for Disease Control and Prevention (CDC) guidelines, which recommend avoiding vaccines for those with severe allergies to components like polyethylene glycol (PEG). For children, age-specific dosages (e.g., 10 µg for Pfizer in 5–11-year-olds) and staggered administration schedules minimize risks. Parents should monitor for mild side effects like fever or fatigue, which typically resolve within 48 hours.
Comparatively, vaccine safety protocols differ from typical clinical trials in their scale and real-world application. While trials operate in controlled environments, post-market surveillance relies on passive and active reporting systems. For instance, the CDC’s V-safe program uses smartphone-based health checks to collect data from millions of vaccine recipients, identifying trends like increased myocarditis risk in young males post-mRNA vaccination (10–100 cases per million doses). This data informs updates to safety guidelines, such as the temporary pause of the Johnson & Johnson vaccine in 2021 to investigate rare blood clots. Such adaptive protocols demonstrate a commitment to safety beyond initial trial phases.
In conclusion, Vaccine Safety Protocols are not a one-time check but a dynamic system integrating scientific rigor, regulatory oversight, and public health vigilance. From precise dosing in trials to real-time monitoring post-approval, these protocols ensure vaccines remain among the safest medical interventions. Understanding these mechanisms can alleviate concerns that vaccination is an extension of clinical trials, emphasizing instead their role as a safeguard for global health. Practical adherence to guidelines, such as age-appropriate dosing and post-vaccination observation, empowers individuals to participate confidently in vaccination programs.
Understanding the Key Components in the Coronavirus Vaccine
You may want to see also
Explore related products






![]()
Emergency Use Authorization
The COVID-19 pandemic accelerated the development and distribution of vaccines at an unprecedented pace, raising questions about their safety and efficacy. One mechanism that facilitated this rapid rollout was Emergency Use Authorization (EUA), a regulatory pathway that allows the use of medical products during public health emergencies without the typical lengthy approval process. Unlike full approval, which requires extensive data from large-scale clinical trials, EUA relies on preliminary evidence that the product’s benefits outweigh its risks. This distinction is critical for understanding why some perceive vaccines as part of an ongoing clinical trial, even though they are administered to the general public.
Consider the practical implications of EUA for vaccine distribution. For instance, the Pfizer-BioNTech COVID-19 vaccine received EUA in December 2020 for individuals aged 16 and older, based on data from a Phase 3 trial involving approximately 44,000 participants. The EUA allowed healthcare providers to administer a two-dose regimen, 21 days apart, while ongoing trials continued to monitor long-term effects. This phased approach ensured immediate access to a potentially life-saving intervention while acknowledging the need for further study. It’s important to note that EUA is not a shortcut but a balanced response to urgent public health needs, prioritizing speed without compromising core safety standards.
Critics often argue that EUA vaccines are experimental, conflating their status with ongoing clinical trials. However, this comparison is misleading. Clinical trials are tightly controlled studies with specific inclusion criteria, placebo groups, and rigorous data collection. In contrast, EUA vaccines are administered broadly, with real-world data collected through surveillance systems like the CDC’s V-safe program. For example, the Moderna vaccine’s EUA was supported by a trial showing 94.1% efficacy, but post-authorization monitoring tracked rare side effects like myocarditis, particularly in young males aged 12–29. This distinction highlights how EUA bridges the gap between controlled trials and population-wide use, ensuring both accessibility and ongoing safety evaluation.
To navigate the nuances of EUA, it’s essential to understand its limitations and safeguards. Unlike fully approved vaccines, EUA products carry specific instructions and restrictions. For instance, the Johnson & Johnson vaccine’s EUA included a warning about rare blood clots in women under 50, leading to targeted recommendations for this demographic. Additionally, healthcare providers must inform recipients of the vaccine’s EUA status and provide an FDA fact sheet detailing risks and benefits. This transparency empowers individuals to make informed decisions while acknowledging the provisional nature of the authorization.
In conclusion, Emergency Use Authorization is a vital tool that balances urgency with safety, enabling rapid vaccine deployment during crises. While it differs from full approval and clinical trials, it is not synonymous with experimentation. By understanding EUA’s role, specific requirements, and ongoing monitoring mechanisms, the public can better appreciate the rigor behind vaccine distribution. This clarity is crucial for addressing misconceptions and fostering trust in public health interventions.
Tetanus Vaccines: Tracking Immunization Records for Optimal Protection
You may want to see also
Explore related products






![]()
Trial Participant Demographics
The diversity of trial participant demographics is a critical factor in determining the safety and efficacy of vaccines. Clinical trials for COVID-19 vaccines, for instance, aimed to enroll participants across various age groups, racial and ethnic backgrounds, and health statuses. The Pfizer-BioNTech trial included approximately 44,000 participants, with 42% being from diverse racial and ethnic groups, while Moderna’s trial enrolled 30,000 individuals, ensuring representation from high-risk populations such as the elderly and those with comorbidities. This intentional inclusivity helps identify potential variations in immune response and side effects across different demographics.
Consider the age distribution in vaccine trials, which often mirrors the intended recipient population. For pediatric trials, participants are typically grouped into age categories such as 5–11, 12–15, and 16–17 years, with dosage adjustments made accordingly. For example, Pfizer’s pediatric trial administered a lower dose (10 µg) to children aged 5–11 compared to the 30 µg dose given to adults. This stratification ensures safety and efficacy data are tailored to specific developmental stages, addressing concerns about children’s unique immune systems.
Racial and ethnic diversity in trials is not just a moral imperative but a scientific necessity. Historically, underrepresented groups have faced disparities in healthcare access and outcomes, making their inclusion vital for equitable vaccine deployment. The AstraZeneca trial, for instance, enrolled participants from multiple countries, including Brazil and South Africa, to assess the vaccine’s effectiveness against diverse SARS-CoV-2 variants. Such global representation enhances the generalizability of trial results, ensuring vaccines work across populations with varying genetic and environmental factors.
Practical tips for ensuring diverse trial demographics include community engagement and transparent communication. Researchers must build trust with underrepresented communities by involving local leaders and addressing cultural concerns. Offering flexible trial participation options, such as mobile clinics or compensated time off, can reduce barriers to enrollment. Additionally, providing clear, multilingual information about trial procedures and potential risks fosters informed consent and encourages broader participation.
In conclusion, trial participant demographics are a cornerstone of vaccine development, influencing both scientific validity and public trust. By prioritizing diversity in age, race, ethnicity, and health status, researchers can ensure vaccines are safe and effective for all. This approach not only strengthens the scientific rigor of trials but also promotes health equity, making vaccines a truly universal tool in the fight against disease.
Antibody Infusion vs. Vaccine: Key Differences Explained Simply
You may want to see also
Explore related products






![]()
Long-Term Side Effects Monitoring
The COVID-19 vaccines underwent rigorous clinical trials to assess their safety and efficacy before emergency use authorization, but these trials primarily focused on short-term outcomes, typically spanning a few months. Long-term side effects monitoring, therefore, becomes critical to ensure ongoing safety as millions receive these vaccines globally. Post-authorization surveillance systems, such as the CDC’s Vaccine Adverse Event Reporting System (VAERS) and the FDA’s Vaccine Safety Datalink (VSD), play a pivotal role in this process. These systems rely on healthcare providers and individuals to report adverse events, enabling real-world data collection that extends beyond the clinical trial timeframe.
One challenge in long-term monitoring is distinguishing between coincidental health events and vaccine-related side effects. For instance, rare conditions like myocarditis in young males (particularly after the second dose of mRNA vaccines) were identified through post-authorization surveillance. While clinical trials included participants aged 16 and older, the long-term impact on specific age groups, such as adolescents or the elderly, requires continuous observation. Dosage adjustments, like the half-dose recommendation for children aged 5–11, further emphasize the need for tailored monitoring to ensure safety across diverse populations.
To effectively track long-term effects, passive reporting systems must be complemented by active surveillance studies. For example, the CDC’s v-safe program sends regular health check-ins to vaccine recipients via smartphone, collecting data on symptoms over time. Such proactive approaches can identify patterns that might go unnoticed in passive systems. Additionally, international collaboration, as seen in the WHO’s Global Advisory Committee on Vaccine Safety, ensures that data from various countries contribute to a comprehensive understanding of vaccine safety.
Practical tips for individuals include keeping a symptom journal after vaccination, especially if pre-existing conditions or concerns exist. Reporting any unusual symptoms promptly to healthcare providers ensures timely investigation and contributes to the broader safety database. For parents, monitoring children for signs of fatigue, chest pain, or persistent fever post-vaccination is crucial, given the rarity but seriousness of myocarditis cases. Transparency in reporting and public communication about findings builds trust and encourages continued participation in monitoring efforts.
In conclusion, long-term side effects monitoring is an essential extension of clinical trials, bridging the gap between controlled studies and real-world application. By leveraging advanced surveillance systems, fostering global collaboration, and empowering individuals to participate actively, we can ensure the ongoing safety of vaccines. This vigilance not only protects public health but also reinforces confidence in vaccination programs as a cornerstone of disease prevention.
Update Vaccine Certificate: Switch Aadhaar to Passport Easily
You may want to see also
Explore related products






![]()
Placebo Group Ethics
The use of placebo groups in vaccine clinical trials raises profound ethical questions, particularly when effective vaccines already exist. Consider the COVID-19 vaccine trials conducted in 2020, where some participants received a saline injection instead of the active vaccine. At the time, no proven vaccines were available, but the rapidly escalating global death toll heightened the moral tension. Withholding a potentially life-saving intervention, even in a controlled trial, demands rigorous justification to ensure participant safety and trial integrity.
Ethical guidelines, such as the Declaration of Helsinki, emphasize that placebo use is acceptable only when no proven intervention exists. However, this principle becomes murky in multinational trials. For instance, a COVID-19 vaccine trial conducted in a low-income country with limited access to vaccines might ethically justify a placebo group, as participants would not forgo an available treatment. In contrast, using a placebo group in a high-income country with widespread vaccine access would likely be deemed unethical. This geographic disparity underscores the need for context-specific ethical frameworks in global clinical research.
One practical solution to mitigate ethical concerns is the "active comparator" design, where participants receive an existing vaccine instead of a placebo. For example, in a trial for a new influenza vaccine, the placebo group could instead receive the current seasonal flu vaccine. This approach ensures all participants receive some protection while allowing researchers to assess the new vaccine’s efficacy. However, this method may complicate data interpretation if the comparator vaccine’s effectiveness varies significantly from the experimental one.
Critics argue that even with safeguards, placebo groups exploit vulnerable populations. In the case of the 2021 malaria vaccine trials in Africa, some participants received a placebo despite the disease’s high mortality rate among children. Proponents counter that the trials provided extensive healthcare monitoring and ensured access to treatment upon illness. Balancing scientific rigor with participant welfare requires transparent communication of risks and benefits, as well as post-trial access to the proven intervention for all participants.
Ultimately, the ethics of placebo groups in vaccine trials hinge on a delicate calculus: the urgency of the health threat, the availability of alternatives, and the trial’s potential to benefit humanity. For researchers and ethicists, the challenge lies in designing trials that advance medical knowledge without compromising moral principles. As vaccine development continues to evolve, so too must the ethical frameworks governing their testing, ensuring that scientific progress serves the greater good without sacrificing individual rights.
Vaccination: A Global Shield Against Disease, Disability, Death, and Inequity
You may want to see also
Frequently asked questions
No, the COVID-19 vaccines authorized for use by regulatory agencies like the FDA, EMA, and WHO have completed their clinical trials and have been approved or authorized for emergency use based on demonstrated safety and efficacy.
No, receiving an authorized COVID-19 vaccine does not make you part of a clinical trial. Clinical trials were conducted before the vaccines were approved or authorized, and ongoing monitoring is part of standard post-authorization safety surveillance.
No, while the COVID-19 vaccines were developed quickly, they underwent rigorous clinical trials involving tens of thousands of participants. The expedited process was made possible by global collaboration, funding, and prioritizing vaccine development without skipping safety or efficacy testing.