The distribution of vaccines in India has been a critical aspect of the country's public health strategy, particularly in the wake of the COVID-19 pandemic. As one of the world's most populous nations, India faced the monumental task of vaccinating its diverse and widespread population, which includes both urban and rural areas. The government, in collaboration with various stakeholders, implemented a phased approach to ensure equitable access to vaccines, prioritizing vulnerable groups such as healthcare workers, the elderly, and those with comorbidities. The rollout involved a combination of centralized and state-level efforts, leveraging technology for registration, monitoring, and supply chain management. Despite challenges such as vaccine hesitancy, logistical hurdles, and initial supply constraints, India's vaccination drive has made significant progress, with millions of doses administered and a notable reduction in severe cases and mortality rates. The success of this initiative underscores the importance of robust planning, public awareness, and international cooperation in addressing global health crises.
Explore related products


$3.29 $24.95

$18.99 $18.99

$29.95 $25.48


What You'll Learn
- Vaccine Types: Details on Covishield, Covaxin, Sputnik V, and other vaccines available in India
- Distribution Channels: Overview of government, private, and rural distribution networks for vaccines
- Equity Concerns: Analysis of vaccine accessibility across states, urban-rural divides, and marginalized groups
- Logistical Challenges: Issues like cold chain maintenance, transportation, and storage infrastructure for vaccines
- Public Awareness: Impact of misinformation, hesitancy, and campaigns to promote vaccine acceptance
![]()
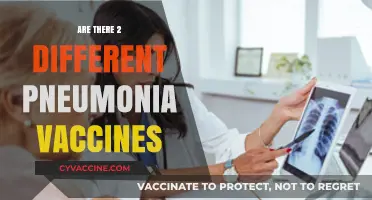
Vaccine Types: Details on Covishield, Covaxin, Sputnik V, and other vaccines available in India
India's vaccination drive has been a cornerstone of its fight against COVID-19, with multiple vaccines approved for use. Each vaccine has distinct characteristics, making it crucial for individuals to understand their options. Here’s a detailed breakdown of the primary vaccines available in India: Covishield, Covaxin, Sputnik V, and others, including their types, efficacy, dosage, and eligibility criteria.
Covishield, developed by AstraZeneca and manufactured by the Serum Institute of India, is a viral vector-based vaccine. It uses a modified version of a chimpanzee adenovirus to deliver genetic material that triggers an immune response. Administered in two doses, spaced 12–16 weeks apart, Covishield has shown an average efficacy of around 70–90% in preventing symptomatic COVID-19. It is approved for individuals aged 18 and above. A key advantage is its storage requirement of 2–8°C, making it easier to distribute in diverse climatic conditions. For optimal protection, ensure timely administration of the second dose and monitor for mild side effects like fever or fatigue.
Covaxin, India’s first indigenous COVID-19 vaccine, is developed by Bharat Biotech in collaboration with the Indian Council of Medical Research (ICMR) and the National Institute of Virology (NIV). It is an inactivated vaccine, meaning it contains killed coronavirus particles to stimulate immunity. Covaxin is administered in two doses, 4–6 weeks apart, and has demonstrated an efficacy of approximately 78% against symptomatic COVID-19. Approved for individuals aged 18 and above, it has also been extended to children aged 12–18. Its storage requirement is similar to Covishield, at 2–8°C. While side effects are generally mild, including pain at the injection site, it remains a reliable choice for those preferring a non-viral vector vaccine.
Sputnik V, developed by Russia’s Gamaleya Research Institute, is another viral vector-based vaccine. It uses two different adenoviruses (Ad26 and Ad5) for its two doses, administered 21 days apart. This unique approach aims to enhance immune response and reduce the likelihood of vector-induced immunity. Sputnik V boasts a high efficacy rate of around 91.6% against symptomatic COVID-19 and is approved for individuals aged 18 and above. Its storage requirement varies: the first dose requires -18°C, while the second dose can be stored at 2–8°C. For those seeking a vaccine with a novel delivery mechanism, Sputnik V is a compelling option.
Beyond these, India has also approved other vaccines like Moderna (an mRNA vaccine) and Johnson & Johnson (a single-dose viral vector vaccine), though their availability remains limited. Moderna, with an efficacy of around 94%, is administered in two doses, 28 days apart, and requires storage at -20°C. Johnson & Johnson, with an efficacy of around 66–72%, offers the convenience of a single dose and can be stored at 2–8°C. These vaccines provide additional choices, particularly for those with specific preferences or contraindications to other vaccines.
When choosing a vaccine, consider factors like efficacy, dosage schedule, storage requirements, and personal health conditions. For instance, individuals with a history of adenovirus-related illnesses might prefer Covaxin or Moderna. Always consult healthcare professionals for personalized advice. India’s diverse vaccine portfolio ensures accessibility and caters to varying needs, reinforcing the nation’s commitment to public health.
Debunking Myths: Are Cancer Cells Really Put in Vaccines?
You may want to see also
Explore related products






![]()
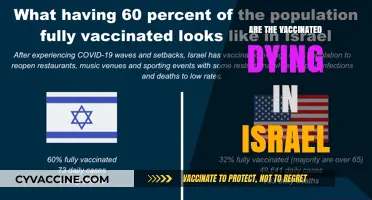
Distribution Channels: Overview of government, private, and rural distribution networks for vaccines
India's vaccine distribution network is a complex web, weaving together government initiatives, private sector involvement, and tailored strategies for rural accessibility. At its core lies the government's Universal Immunization Programme (UIP), a cornerstone of public health reaching over 26 million newborns and 29 million pregnant women annually. This program leverages a tiered system: national vaccine stores supply state-level cold chain points, which then distribute to districts, blocks, and finally, sub-centers and health facilities. This ensures a steady flow of vaccines like the pentavalent vaccine (protecting against five diseases) and the rotavirus vaccine, administered in a three-dose schedule starting at 6 weeks of age.
Rigorous cold chain management is crucial, with vaccines requiring temperatures between 2-8°C.
Private healthcare providers play a significant role, particularly in urban areas. They procure vaccines directly from manufacturers or authorized distributors, offering a wider range of vaccines, including those not covered under the UIP, such as the pneumococcal conjugate vaccine (PCV). This dual-track system allows for greater choice but can lead to disparities in access and affordability. While private providers offer convenience and potentially faster access, costs can be prohibitive for many, highlighting the importance of a robust public system.
Market dynamics also influence vaccine availability. Private providers often prioritize vaccines with higher profit margins, potentially leading to shortages of essential vaccines in the public sector.
Reaching India's vast rural population presents unique challenges. The government employs innovative strategies like mobile vaccination teams, outreach sessions in remote villages, and community health workers to bridge the gap. These teams often travel long distances, carrying vaccines in portable cold boxes, ensuring children in even the most inaccessible areas receive their measles-rubella vaccine (administered at 9-12 months and 16-24 months) or the Japanese encephalitis vaccine, crucial in endemic regions. Community engagement is vital. Local leaders and ASHA workers (Accredited Social Health Activists) play a pivotal role in educating communities, addressing vaccine hesitancy, and ensuring timely immunization.
The success of India's vaccine distribution hinges on a delicate balance between government leadership, private sector participation, and community-driven solutions. While the UIP provides a strong foundation, addressing disparities in access and affordability remains crucial. Strengthening rural infrastructure, ensuring sustainable cold chain solutions, and fostering public-private partnerships are essential for achieving universal immunization coverage and protecting the health of every Indian child.
Vaccine Antigens: Are They Excreted or Retained?
You may want to see also
Explore related products






![]()
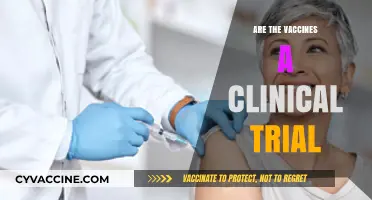
Equity Concerns: Analysis of vaccine accessibility across states, urban-rural divides, and marginalized groups
India's vaccine distribution landscape reveals stark disparities, with equity concerns looming large across states, urban-rural divides, and marginalized communities. Data from the CoWIN dashboard highlights that as of 2023, southern states like Kerala and Tamil Nadu have consistently achieved higher vaccination rates (over 80% fully vaccinated) compared to northeastern states like Nagaland and Manipur, where rates hover around 50-60%. This variation underscores systemic challenges in reaching geographically isolated regions, despite centralized vaccine procurement.
Urban centers, with their denser healthcare infrastructure, have outpaced rural areas in vaccine accessibility. For instance, while metropolitan cities like Mumbai and Delhi have administered over 100 million doses, rural districts in Bihar and Uttar Pradesh struggle with last-mile delivery. The urban-rural gap is further exacerbated by digital divides—rural populations often lack internet access or smartphones, making it difficult to navigate the CoWIN platform for slot bookings. Mobile vaccination camps, though introduced, remain insufficient to bridge this gap, leaving rural elderly and marginalized groups disproportionately underserved.
Marginalized groups, including tribal communities, Dalits, and religious minorities, face compounded barriers to vaccine access. Language barriers, misinformation, and historical distrust of government initiatives have hindered uptake. For example, in tribal areas of Chhattisgarh and Odisha, vaccine hesitancy remains high due to cultural misconceptions and lack of localized awareness campaigns. Additionally, the exclusion of these groups from digital registration systems—often requiring Aadhaar linkage—has further marginalized them. Targeted interventions, such as community health workers delivering vaccines in local languages, have shown promise but require scaling up.
To address these inequities, a multi-pronged strategy is essential. First, state-specific allocation models should account for population density, healthcare infrastructure, and socio-economic indicators. Second, rural areas need decentralized vaccination drives, leveraging anganwadis and primary health centers as hubs. Third, marginalized groups require tailored outreach, including offline registration options and culturally sensitive messaging. Finally, real-time monitoring of disparities, coupled with flexible policy adjustments, can ensure equitable distribution. Without these measures, India risks leaving behind its most vulnerable populations in the race to achieve herd immunity.
Monkeypox vs. Smallpox: Are Their Vaccines Interchangeable?
You may want to see also
Explore related products






![]()
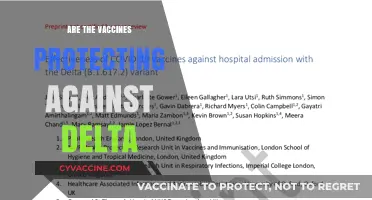
Logistical Challenges: Issues like cold chain maintenance, transportation, and storage infrastructure for vaccines
India's vaccine distribution network faces a critical challenge: maintaining the cold chain. Many vaccines, including those for COVID-19, are temperature-sensitive. The Pfizer-BioNTech vaccine, for instance, requires ultra-cold storage at -70°C, while the Oxford-AstraZeneca vaccine (Covishield) is more stable at 2-8°C. This disparity highlights the need for a flexible and robust cold chain infrastructure. India's diverse geography, from the Himalayas to tropical regions, exacerbates the problem, as temperature variations can compromise vaccine efficacy.
Consider the transportation process. Vaccines must travel from manufacturing plants to state-level stores, then to district hubs, and finally to vaccination sites. Each leg of this journey demands precise temperature control. Refrigerated trucks, cold boxes, and data loggers are essential tools, but their availability and maintenance vary widely across states. For example, rural areas often lack reliable electricity, making it difficult to power refrigeration units consistently. This inconsistency can lead to vaccine wastage, a costly and avoidable issue.
Storage infrastructure is another bottleneck. Urban centers may have well-equipped cold storage facilities, but rural and remote areas often rely on makeshift solutions. Walk-in coolers, deep freezers, and ice-lined refrigerators are not universally available. Moreover, the last-mile delivery to remote villages requires innovative solutions like solar-powered refrigerators or drone technology. Without such advancements, ensuring equitable vaccine distribution remains a daunting task.
To address these challenges, a multi-pronged approach is necessary. First, invest in upgrading cold chain infrastructure, particularly in underserved regions. Second, train healthcare workers on proper handling and storage protocols. Third, leverage technology for real-time monitoring of vaccine temperatures during transit and storage. Finally, foster public-private partnerships to mobilize resources and expertise. By tackling these logistical hurdles head-on, India can strengthen its vaccine distribution network and protect its population more effectively.
Vaccination Requirements for Army Enlistment Explained
You may want to see also
Explore related products






![]()
Public Awareness: Impact of misinformation, hesitancy, and campaigns to promote vaccine acceptance
Misinformation spreads faster than a virus, and in the context of India's vaccine distribution, its impact has been profound. False claims about vaccines causing infertility, altering DNA, or containing microchips have fueled hesitancy, particularly in rural areas where access to reliable information is limited. A 2021 study by the Indian Council of Medical Research (ICMR) revealed that 28% of respondents believed at least one myth about COVID-19 vaccines. This highlights the urgent need for targeted public awareness campaigns to counter misinformation and build trust in vaccination drives.
Hesitancy isn't just a byproduct of misinformation; it's also rooted in historical mistrust of medical systems and a lack of personalized communication. For instance, marginalized communities often face language barriers or cultural sensitivities that generic campaigns fail to address. A one-size-fits-all approach won't work. Instead, campaigns must be localized, incorporating regional languages, community leaders, and culturally relevant messaging. For example, in Kerala, health workers used folk songs and puppet shows to educate villagers about vaccine safety, achieving a 90% vaccination rate among eligible adults by early 2022.
Effective campaigns don't just debunk myths—they empower individuals with actionable knowledge. For instance, explaining that the Covishield vaccine requires a gap of 12–16 weeks between doses, while Covaxin needs 4–6 weeks, helps recipients plan and reduces confusion. Practical tips, such as scheduling reminders for second doses or informing citizens about the CoWIN portal for registration, can significantly improve uptake. Pairing this with transparent data on vaccine efficacy and side effects fosters confidence.
Comparing India's approach to global strategies reveals both strengths and gaps. While the country's use of digital platforms like WhatsApp and Aarogya Setu for awareness is innovative, it excludes those without smartphones or internet access. In contrast, Brazil's door-to-door campaigns and South Africa's community health worker programs offer lessons in inclusivity. India could bridge this gap by training ASHA workers to address specific concerns, such as clarifying that vaccines are safe for pregnant women after the first trimester, as recommended by the Ministry of Health.
Ultimately, the fight against vaccine hesitancy is a battle for minds, not just arms. Misinformation thrives in vacuums of knowledge, but well-designed campaigns can fill that void. By combining localized strategies, practical education, and lessons from global best practices, India can turn the tide on hesitancy. The goal isn't just to distribute vaccines—it's to ensure they're accepted, trusted, and embraced by every eligible citizen.
Exploring the Reported Efficacy of the BCG Vaccine: What We Know
You may want to see also
Frequently asked questions
India is primarily distributing Covishield (Oxford-AstraZeneca), Covaxin (Bharat Biotech), and Sputnik V (Gamaleya Institute) as part of its COVID-19 vaccination drive.
Vaccine distribution in India is managed through the CoWIN (COVID Vaccine Intelligence Network) platform, which coordinates vaccination drives across states and union territories, ensuring equitable access.
Yes, all vaccines distributed in India are approved by the Drugs Controller General of India (DCGI) and meet safety and efficacy standards.
Yes, vaccines are available to all eligible age groups as per government guidelines, with priority given to healthcare workers, senior citizens, and vulnerable populations.