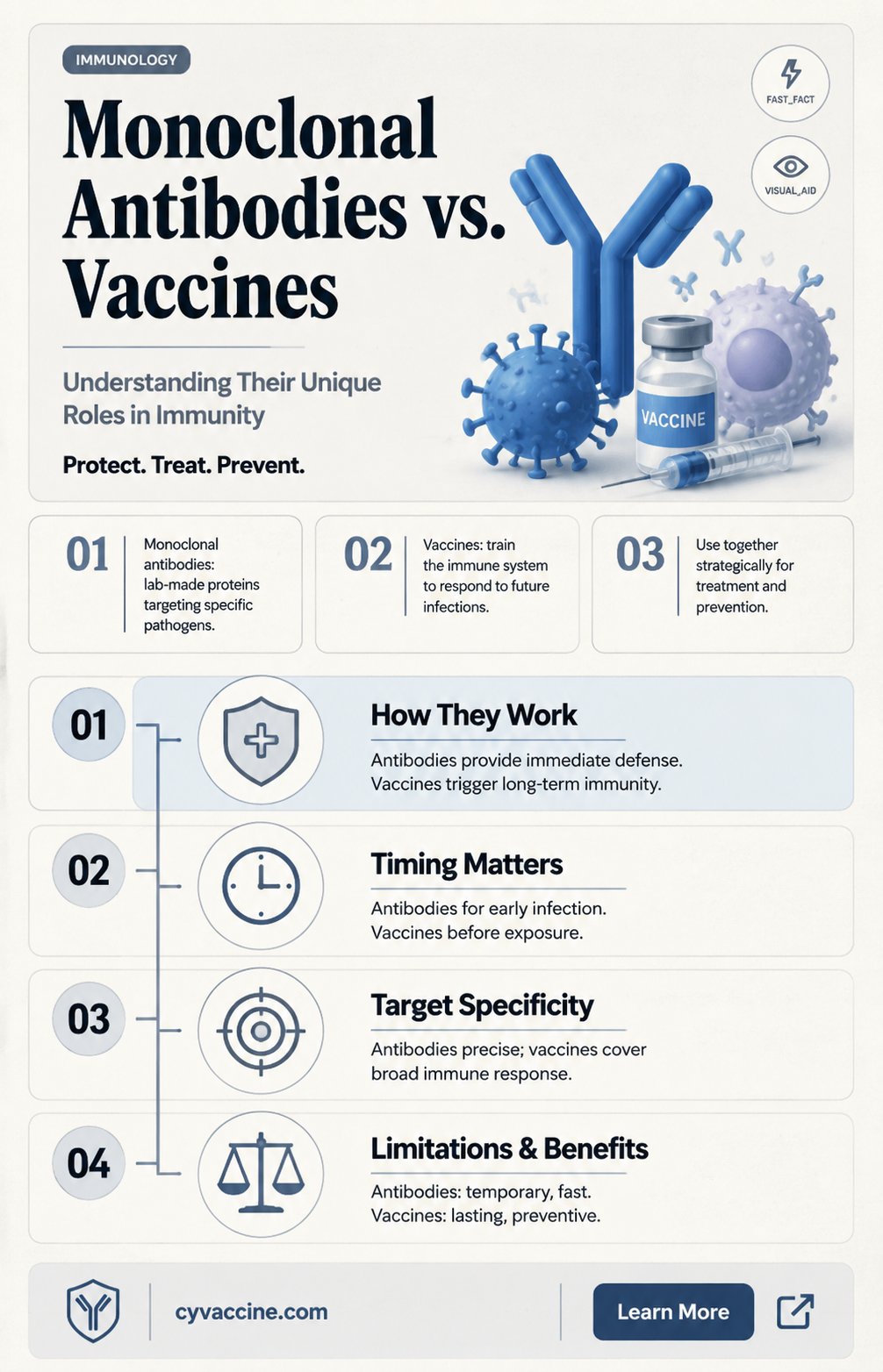
Monoclonal antibodies (mAbs) and vaccines are both powerful tools in modern medicine, but they serve distinct purposes and function through different mechanisms. While vaccines stimulate the body’s immune system to produce its own antibodies and memory cells for long-term protection against specific pathogens, monoclonal antibodies are lab-created proteins designed to directly target and neutralize a particular antigen, often providing immediate but temporary defense. Unlike vaccines, which are preventive measures administered before exposure to a disease, mAbs are typically used as treatments after infection or for specific conditions like cancer or autoimmune disorders. Though both leverage the principles of immunology, their applications, duration of effect, and modes of action highlight their complementary roles in healthcare rather than their equivalence.
Explore related products






What You'll Learn
- Mechanism of Action: How monoclonal antibodies target pathogens vs. vaccines training immune systems
- Duration of Protection: Short-term immunity from antibodies vs. long-term vaccine-induced immunity
- Administration Method: Vaccines are preventive injections; antibodies are therapeutic infusions/injections
- Immune Response: Vaccines stimulate natural immunity; antibodies provide direct pathogen neutralization
- Use Cases: Vaccines prevent diseases; antibodies treat active infections or high-risk exposures
![]()
Mechanism of Action: How monoclonal antibodies target pathogens vs. vaccines training immune systems
Monoclonal antibodies and vaccines both aim to protect against pathogens, but their mechanisms of action differ fundamentally. Monoclonal antibodies are lab-engineered proteins designed to directly neutralize or mark pathogens for destruction. They act as a rapid, targeted intervention, binding to specific antigens on viruses or bacteria to block their ability to infect cells. For instance, COVID-19 monoclonal antibody treatments like casirivimab-imdevimab are administered intravenously or subcutaneously in doses ranging from 1,200 to 2,400 mg, providing immediate protection for high-risk individuals. In contrast, vaccines train the immune system to recognize and combat pathogens by introducing a harmless piece of the pathogen (e.g., mRNA, protein, or weakened virus) to stimulate antibody production and immune memory. This process takes weeks, as seen with the COVID-19 mRNA vaccines, which require 3–4 weeks between doses for full immune response development.
Consider the analogy of a home invasion: monoclonal antibodies are like hiring a security guard to immediately tackle the intruder, while vaccines are akin to training the homeowner to defend themselves effectively in the future. Monoclonal antibodies offer instant but temporary protection, typically lasting weeks to months, depending on the treatment. Vaccines, however, provide long-term immunity, often years, by priming the immune system to respond swiftly upon pathogen exposure. For example, the flu vaccine is reformulated annually to match circulating strains, while monoclonal antibodies for influenza, such as obiltoxaximab, are used post-exposure in high-risk patients like the elderly or immunocompromised.
A critical distinction lies in their application. Monoclonal antibodies are primarily used for prophylaxis or treatment in vulnerable populations, such as those with compromised immune systems who may not mount a sufficient response to vaccines. Vaccines, on the other hand, are administered prophylactically to healthy individuals to prevent infection altogether. For instance, the Ebola monoclonal antibody cocktail Inmazeb is used to treat active infections, while the Ebola vaccine Ervebo is given to at-risk populations in outbreak zones. Dosage and administration routes also differ: monoclonal antibodies are often given as single, high-dose infusions, whereas vaccines typically require multiple lower-dose injections.
From a practical standpoint, understanding these mechanisms helps tailor interventions to specific needs. For example, a 65-year-old with diabetes might receive both a COVID-19 vaccine and monoclonal antibody treatment if exposed to the virus, combining immediate protection with long-term immunity. However, monoclonal antibodies are not a substitute for vaccination, as they do not confer lasting immunity. Conversely, relying solely on vaccines leaves a window of vulnerability before immunity is established. Clinicians must weigh factors like patient age, comorbidities, and exposure risk when deciding between these tools. For instance, a healthcare worker might prioritize vaccination for ongoing protection, while a cancer patient undergoing chemotherapy could benefit from monoclonal antibodies as a stopgap measure.
In summary, while both monoclonal antibodies and vaccines combat pathogens, their mechanisms are distinct: one acts as a direct intervention, the other as a training program for the immune system. Monoclonal antibodies provide immediate but temporary protection, ideal for high-risk scenarios, while vaccines offer durable immunity, making them a cornerstone of public health. Practical application requires balancing these strengths, considering factors like dosage, timing, and patient profile. For optimal protection, a layered approach—combining vaccination with targeted monoclonal antibody use when necessary—may be the most effective strategy.
Navigating School Enrollment for Unvaccinated Children: A Parent’s Guide
You may want to see also
Explore related products






![]()
Duration of Protection: Short-term immunity from antibodies vs. long-term vaccine-induced immunity
Monoclonal antibodies and vaccines both harness the immune system to combat pathogens, but their mechanisms and durations of protection differ significantly. While vaccines stimulate the body’s own immune response to provide long-term immunity, monoclonal antibodies offer immediate, short-term protection by directly introducing lab-created antibodies into the system. This distinction is critical for understanding their roles in prevention and treatment.
Consider the practical implications of this difference. A single dose of monoclonal antibodies, such as those used for COVID-19 treatment (e.g., casirivimab/imdevimab), provides protection for only a few weeks to months. For instance, studies show that monoclonal antibody treatments can reduce the risk of hospitalization or death in high-risk individuals for up to 90 days. However, this protection wanes rapidly, requiring repeated administrations if ongoing immunity is needed. In contrast, vaccines like the Pfizer-BioNTech or Moderna COVID-19 shots induce long-term immunity by training the immune system to produce memory cells. While booster doses may be necessary to maintain efficacy, the initial series (typically two doses) can provide robust protection for at least six months to a year, with some studies suggesting immunity lasting even longer.
The age and health of the recipient further highlight the disparity in protection duration. Monoclonal antibodies are often reserved for vulnerable populations, such as the elderly or immunocompromised, who may not mount a sufficient response to vaccines. For example, individuals over 65 or those with conditions like cancer or organ transplants may receive monoclonal antibodies as a preventive measure during outbreaks. However, this approach is not sustainable for long-term protection due to the short duration of antibody efficacy. Vaccines, on the other hand, are designed for broader populations, including healthy adults and children, and offer a more cost-effective and logistically feasible solution for sustained immunity.
From a strategic perspective, the choice between monoclonal antibodies and vaccines depends on the context. Monoclonal antibodies are invaluable for immediate protection in high-risk scenarios, such as treating active infections or preventing severe disease in exposed individuals. Vaccines, however, are the cornerstone of public health strategies, providing herd immunity and reducing disease transmission over time. For instance, during the COVID-19 pandemic, monoclonal antibodies were used as a stopgap measure for vulnerable populations, while vaccines were prioritized for mass immunization campaigns.
In conclusion, while monoclonal antibodies and vaccines both leverage the immune system, their durations of protection reflect their distinct purposes. Monoclonal antibodies offer short-term, immediate defense, making them ideal for targeted interventions. Vaccines, however, provide long-term immunity, serving as the foundation for population-wide disease prevention. Understanding this difference is essential for tailoring medical strategies to individual and public health needs.
Understanding the 5-in-1 Vaccine: Protecting Pets from Parvovirus & More
You may want to see also
Explore related products






![]()
Administration Method: Vaccines are preventive injections; antibodies are therapeutic infusions/injections
Monoclonal antibodies and vaccines serve distinct roles in healthcare, and their administration methods reflect these differences. Vaccines are primarily preventive tools, administered as injections to stimulate the immune system to recognize and combat future pathogens. For instance, the COVID-19 mRNA vaccines, such as Pfizer-BioNTech and Moderna, are given in doses of 30 µg and 100 µg, respectively, typically in a two-dose series for adults, with boosters recommended for sustained immunity. These injections are designed to train the body to produce its own antibodies, offering long-term protection against infection.
In contrast, monoclonal antibodies are therapeutic agents, delivered as infusions or injections to provide immediate immune support. Unlike vaccines, they are not preventive but rather a treatment for active infections or conditions. For example, COVID-19 monoclonal antibody treatments like Regeneron’s casirivimab and imdevimab are administered intravenously in a single dose of 1,200 mg each, or subcutaneously in a combined dose of 600 mg. These treatments are typically reserved for high-risk individuals, such as the elderly or immunocompromised, who are already infected or exposed to the virus. The goal is to neutralize the pathogen directly, rather than teaching the immune system to respond.
The timing and context of administration further highlight the differences. Vaccines are often given in controlled settings, such as clinics or pharmacies, with specific schedules (e.g., weeks apart for COVID-19 vaccines). Monoclonal antibodies, however, are administered urgently, often within days of symptom onset or exposure, to maximize their therapeutic effect. For instance, the FDA recommends COVID-19 monoclonal antibody treatment within 10 days of symptom onset for eligible patients. This urgency underscores their role as a reactive measure rather than a proactive one.
Practical considerations also differ. Vaccines are widely accessible, with mass vaccination campaigns targeting broad populations, including children as young as 6 months for some vaccines. Monoclonal antibodies, on the other hand, are resource-intensive and require specialized healthcare settings for administration, limiting their availability. Patients receiving monoclonal antibodies may need monitoring for adverse reactions, such as infusion-related symptoms, which are rare but possible. This contrasts with vaccines, where side effects are generally mild and self-limiting, such as soreness at the injection site or fatigue.
In summary, while both vaccines and monoclonal antibodies involve injections or infusions, their administration methods are tailored to their unique purposes. Vaccines are preventive, administered proactively to build immunity, while monoclonal antibodies are therapeutic, deployed reactively to combat active threats. Understanding these distinctions is crucial for healthcare providers and patients alike, ensuring appropriate use and maximizing the benefits of each intervention.
Jenny McCarthy's Role in Spreading Vaccine-Autism Misinformation
You may want to see also
Explore related products






![]()
Immune Response: Vaccines stimulate natural immunity; antibodies provide direct pathogen neutralization
Vaccines and monoclonal antibodies both aim to combat pathogens, but they operate through distinct mechanisms within the immune system. Vaccines function as trainers, preparing the body’s immune cells to recognize and neutralize future threats. When a vaccine is administered—often in doses ranging from 0.5 mL for influenza to 0.3 mL for mRNA COVID-19 vaccines—it introduces a harmless piece of the pathogen (e.g., a protein or weakened virus) to stimulate the production of memory B and T cells. These cells remain dormant until the actual pathogen is encountered, at which point they rapidly activate to produce antibodies and destroy infected cells. This process mimics natural immunity, ensuring a swift and effective response without the risk of severe disease.
In contrast, monoclonal antibodies act as immediate defenders, bypassing the need for immune training. These lab-created proteins are designed to bind directly to specific targets on a pathogen, such as the spike protein of SARS-CoV-2. Administered intravenously or subcutaneously (e.g., 500–1200 mg for COVID-19 treatments), they provide instant protection by neutralizing the pathogen or marking it for destruction by other immune cells. Unlike vaccines, which require weeks to build immunity, monoclonal antibodies offer rapid relief, making them particularly useful for high-risk individuals or during outbreaks. However, their protection is temporary, lasting only as long as the antibodies remain in the system, typically weeks to months.
The key distinction lies in their approach to immunity. Vaccines empower the body to generate its own defense, fostering long-term protection through immune memory. This is why vaccine schedules often include multiple doses (e.g., two doses of Pfizer-BioNTech COVID-19 vaccine spaced 3–4 weeks apart) to strengthen this memory. Monoclonal antibodies, on the other hand, provide a short-term solution, akin to hiring mercenaries rather than training an army. They are invaluable in emergencies but cannot replace the sustained resilience built by vaccines.
Practical considerations further highlight their differences. Vaccines are typically administered to healthy individuals as a preventive measure, often starting in childhood (e.g., the MMR vaccine at 12–15 months and 4–6 years). Monoclonal antibodies are reserved for treatment or pre-exposure prophylaxis in specific populations, such as immunocompromised patients or those exposed to high-risk pathogens. For instance, the FDA has authorized monoclonal antibodies for COVID-19 in individuals aged 12 and older weighing at least 40 kg, but only when administered within 10 days of symptom onset.
In summary, while both tools target pathogens, vaccines stimulate natural immunity by training the immune system, whereas monoclonal antibodies provide direct, immediate neutralization. Each has its role: vaccines as a long-term preventive strategy and monoclonal antibodies as a rapid intervention. Understanding these mechanisms helps tailor their use to maximize public health impact, whether through routine vaccination campaigns or targeted antibody therapies.
Nome's Diphtheria Vaccine Survival: The Science Behind Its Freeze Resistance
You may want to see also
Explore related products






![]()
Use Cases: Vaccines prevent diseases; antibodies treat active infections or high-risk exposures
Vaccines and monoclonal antibodies serve distinct but complementary roles in combating infectious diseases. Vaccines are prophylactic tools designed to prevent diseases by priming the immune system to recognize and neutralize pathogens before infection occurs. They achieve this by introducing a harmless form of the pathogen (or its components) to stimulate the production of memory cells and antibodies. For instance, the COVID-19 mRNA vaccines, administered in two doses spaced 3–4 weeks apart, teach the body to produce spike proteins, triggering an immune response that confers long-term protection. In contrast, monoclonal antibodies are therapeutic agents used to treat active infections or prevent disease in high-risk individuals after exposure. These lab-created antibodies directly target specific pathogens, providing immediate but temporary protection. For example, COVID-19 monoclonal antibody treatments like casirivimab-imdevimab are administered via intravenous infusion (typically 30-minute sessions) within 10 days of symptom onset or high-risk exposure, offering rapid relief for vulnerable populations such as the immunocompromised or elderly.
Consider the scenario of a healthcare worker exposed to a vaccine-preventable disease like influenza. If vaccinated annually, their immune system is likely prepared to fend off the virus, reducing the risk of infection and severe illness. However, if unvaccinated and exposed, monoclonal antibodies could be administered as post-exposure prophylaxis to neutralize the virus before it establishes infection. This example highlights the preventive nature of vaccines versus the reactive role of monoclonal antibodies. Vaccines are most effective when administered before exposure, often requiring weeks to build immunity, while monoclonal antibodies act within hours to days, making them ideal for urgent situations. For instance, rabies post-exposure prophylaxis combines vaccination with rabies immunoglobulin, a form of monoclonal antibody, to prevent the disease after a bite from a potentially rabid animal.
The use cases for these tools also differ in terms of target populations and administration. Vaccines are broadly recommended for entire age groups, such as the measles-mumps-rubella (MMR) vaccine for children over 12 months, or the shingles vaccine for adults over 50. Monoclonal antibodies, however, are typically reserved for specific high-risk groups or individuals with active infections. For example, palivizumab, a monoclonal antibody against respiratory syncytial virus (RSV), is given monthly during RSV season to infants born prematurely or with congenital heart disease. This targeted approach underscores the therapeutic nature of monoclonal antibodies, which are not intended for widespread use like vaccines but are invaluable in critical scenarios.
A key distinction lies in the duration of protection. Vaccines often confer long-term immunity, sometimes lifelong, as seen with the smallpox vaccine. Monoclonal antibodies, however, provide short-term protection, typically lasting weeks to months, as they are cleared from the body over time. This makes them unsuitable for prevention but highly effective in acute situations. For instance, Ebola monoclonal antibody treatments like mAb114 have been used to treat active infections during outbreaks, significantly reducing mortality rates. Conversely, Ebola vaccines like Ervebo are administered to at-risk populations in outbreak zones to prevent infection altogether.
In practice, vaccines and monoclonal antibodies can work synergistically in public health strategies. Vaccination campaigns reduce disease prevalence, while monoclonal antibodies address breakthrough infections or protect those ineligible for vaccination. For example, during the COVID-19 pandemic, vaccines were prioritized for mass immunization, while monoclonal antibodies were reserved for treating high-risk patients or preventing severe outcomes in exposed individuals. This dual approach maximizes protection across populations, leveraging the preventive strength of vaccines and the therapeutic power of monoclonal antibodies. Understanding these use cases ensures appropriate deployment of each tool, optimizing outcomes in both individual and public health contexts.
Hepatitis A Vaccine Risks: Understanding Potential Side Effects and Concerns
You may want to see also
Frequently asked questions
No, monoclonal antibodies are not the same as vaccines. Vaccines stimulate the immune system to produce its own antibodies to prevent infection, while monoclonal antibodies are lab-made proteins directly administered to treat or prevent an active infection.
Monoclonal antibodies are not a replacement for vaccines. Vaccines provide long-term immunity by training the immune system, whereas monoclonal antibodies offer temporary protection and are primarily used for treatment or short-term prevention.
Monoclonal antibodies can help prevent COVID-19 in high-risk individuals, but they do not work like a vaccine. They provide immediate but short-lived protection, whereas vaccines offer longer-lasting immunity by teaching the body to fight the virus.
Monoclonal antibodies are effective for specific uses, such as treating or preventing severe illness in certain cases, but they are not as broadly effective as vaccines. Vaccines remain the primary tool for widespread disease prevention due to their ability to induce long-term immunity.