mRNA vaccines, initially developed to combat infectious diseases like COVID-19, have emerged as a promising frontier in cancer treatment. These vaccines work by delivering genetic instructions to cells, prompting them to produce specific proteins that trigger an immune response against cancer cells. Unlike traditional vaccines, mRNA-based approaches can be tailored to target unique mutations or antigens found in an individual’s tumor, offering a highly personalized therapy. Early clinical trials have shown encouraging results, particularly in cancers like melanoma and certain types of lymphoma, where mRNA vaccines have enhanced immune responses and improved survival rates. While challenges remain, such as optimizing delivery methods and minimizing side effects, the potential of mRNA vaccines to revolutionize cancer treatment is undeniable, marking a significant shift toward precision immunotherapy.
| Characteristics | Values |
|---|---|
| Mechanism of Action | mRNA vaccines deliver genetic material that instructs cells to produce tumor-specific antigens, triggering an immune response against cancer cells. |
| Efficacy in Clinical Trials | Promising results in early-phase trials for cancers like melanoma, prostate, and lung cancer; personalized neoantigen vaccines show improved survival rates. |
| Personalization | Can be tailored to individual tumor mutations (neoantigens), enhancing specificity and efficacy. |
| Combination Therapy | Often used alongside immunotherapy (e.g., checkpoint inhibitors) to enhance anti-tumor immune responses. |
| Safety Profile | Generally well-tolerated, with mild to moderate side effects (e.g., fatigue, fever, injection site pain). |
| Durability of Response | Potential for long-term immune memory, reducing cancer recurrence in some cases. |
| Approved Vaccines | As of 2023, no mRNA cancer vaccines are FDA-approved, but several are in advanced clinical trials (e.g., BioNTech/Moderna collaborations). |
| Challenges | High production costs, variability in tumor mutational burden, and need for rapid manufacturing. |
| Future Potential | Holds promise for treating and preventing cancers, especially in combination with other therapies. |
| Research Focus | Ongoing studies to optimize delivery systems, improve antigen selection, and expand to more cancer types. |
Explore related products






What You'll Learn
![]()
mRNA vaccines' role in cancer immunotherapy
MRNA vaccines, initially celebrated for their rapid development and efficacy against COVID-19, are now at the forefront of a revolutionary approach to cancer immunotherapy. Unlike traditional vaccines that target infectious diseases, mRNA cancer vaccines are designed to train the immune system to recognize and attack cancer cells. This is achieved by delivering genetic instructions to cells, prompting them to produce tumor-specific antigens that trigger an immune response. Early clinical trials have shown promising results, particularly in cancers like melanoma and prostate cancer, where personalized mRNA vaccines have demonstrated the ability to reduce tumor growth and improve survival rates.
One of the most compelling aspects of mRNA cancer vaccines is their adaptability. Unlike conventional treatments like chemotherapy or radiation, which often have broad and harsh side effects, mRNA vaccines can be tailored to individual patients. For instance, BioNTech’s FixVac platform uses predefined mRNA sequences targeting shared cancer antigens, while their iNeSTa (individual Neoantigen Specific Therapy) approach creates personalized vaccines based on a patient’s unique tumor mutations. This precision not only enhances efficacy but also minimizes off-target effects, making it a safer option for patients, especially those in advanced stages of cancer.
However, the journey from promise to practice is not without challenges. One significant hurdle is the complexity of tumor microenvironments, which can suppress immune responses and render vaccines less effective. To address this, researchers are exploring combination therapies, such as pairing mRNA vaccines with immune checkpoint inhibitors like pembrolizumab. Early studies have shown that this approach can enhance the immune system’s ability to infiltrate and destroy tumors, particularly in cancers with high mutational burden. For example, a Phase 2 trial combining mRNA-4157 (an individualized neoantigen therapy) with pembrolizumab demonstrated a 44% objective response rate in melanoma patients, compared to 29% with pembrolizumab alone.
Practical implementation of mRNA cancer vaccines also requires careful consideration of dosage and administration. Typically, patients receive intramuscular injections of the vaccine, with dosing regimens varying based on the cancer type and stage. For instance, in clinical trials, doses ranging from 100 to 200 μg of mRNA have been administered every 3–4 weeks for up to 9 cycles. Patients must be closely monitored for adverse reactions, which are generally mild to moderate and include injection site pain, fatigue, and flu-like symptoms. Importantly, these vaccines are being tested across diverse age groups, with ongoing studies evaluating their safety and efficacy in both younger and older adults, as age-related immune decline can impact vaccine response.
In conclusion, mRNA vaccines represent a transformative tool in cancer immunotherapy, offering personalized, targeted treatment with the potential to revolutionize patient outcomes. While challenges remain, ongoing research and clinical trials continue to refine their application, paving the way for a future where cancer treatment is not only more effective but also more tailored to the individual. As this field evolves, patients and clinicians alike can look forward to a new era of precision medicine, where the power of mRNA technology is harnessed to combat one of humanity’s most formidable diseases.
Handling the Vaccine Question: Navigating Conversations with Confidence and Respect
You may want to see also
Explore related products






![]()
Potential of personalized mRNA cancer vaccines
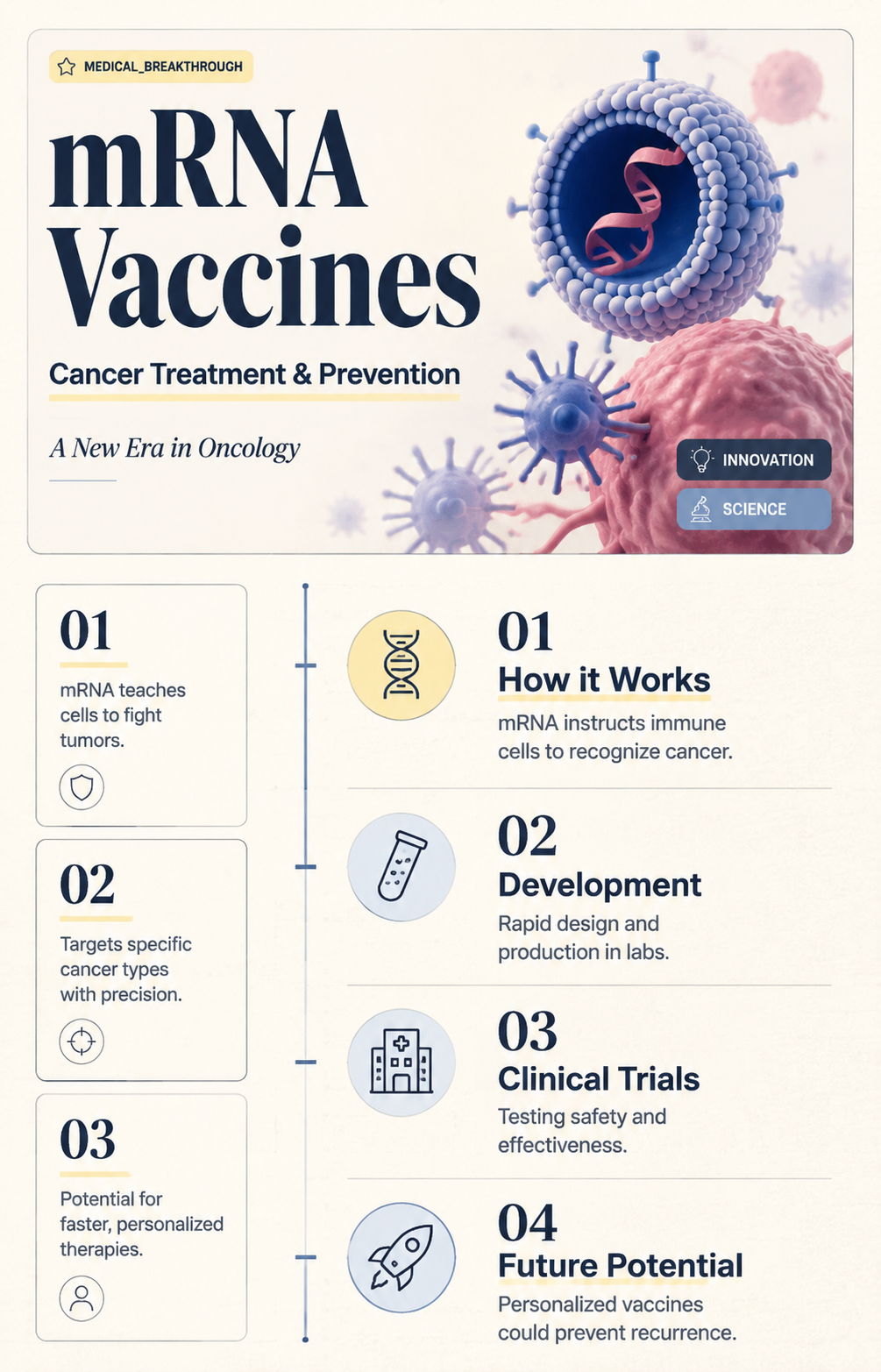
Personalized mRNA cancer vaccines represent a groundbreaking shift in oncology, leveraging the precision of mRNA technology to target individual tumor profiles. Unlike traditional vaccines, these therapies are tailored to a patient’s specific cancer mutations, using mRNA to instruct immune cells to recognize and attack tumor cells. Early clinical trials, such as those by BioNTech and Moderna, have demonstrated promising results, particularly in melanoma and colorectal cancer, with response rates ranging from 20% to 40% in combination with checkpoint inhibitors. This approach hinges on neoantigen identification—unique proteins expressed by cancer cells—which are encoded into mRNA sequences delivered via lipid nanoparticles. Dosage typically involves 80–300 µg of mRNA administered intramuscularly or intradermally every 3–4 weeks, depending on the patient’s immune response and tumor burden.
The development process for personalized mRNA vaccines is both intricate and time-sensitive. It begins with tumor sequencing to identify neoantigens, followed by computational algorithms to select the most immunogenic targets. mRNA synthesis and encapsulation in lipid nanoparticles must occur within weeks to ensure timely treatment initiation. Challenges include ensuring mRNA stability, optimizing nanoparticle delivery to lymph nodes, and minimizing off-target immune reactions. For instance, lipid nanoparticle formulations like ALC-0315 have shown improved tolerability compared to earlier versions, reducing adverse events such as injection site pain or flu-like symptoms. Patients undergoing this treatment are typically monitored via blood tests to assess immune response and tumor markers, with adjustments made based on biomarkers like CD8+ T-cell activation.
One of the most compelling advantages of personalized mRNA cancer vaccines is their adaptability. Unlike static treatments, these vaccines can be updated to address tumor evolution or recurrence, a common challenge in cancers like lung or pancreatic tumors. For example, a patient with non-small cell lung cancer (NSCLC) might receive an initial vaccine targeting 10 neoantigens, followed by a revised version if resistance mutations emerge. This dynamic approach requires ongoing tumor biopsies and sequencing, which, while resource-intensive, offers a sustained line of defense. Practical considerations include the need for cold-chain logistics to preserve mRNA stability, with storage temperatures typically ranging from -20°C to -80°C, and the importance of patient education to manage expectations and side effects.
Despite their potential, personalized mRNA cancer vaccines are not without limitations. Cost remains a significant barrier, with estimates ranging from $50,000 to $200,000 per patient, driven by the complexity of manufacturing and individualized design. Accessibility is further constrained by the need for advanced genomic infrastructure, limiting availability in low-resource settings. Additionally, not all cancers yield sufficient neoantigens for effective targeting, and some patients may develop resistance to the vaccine-induced immune response. Combining mRNA vaccines with immunotherapies like PD-1 inhibitors or CAR-T cell therapy could enhance efficacy, but this requires careful dosing to avoid immune overactivation. For instance, a phase II trial combining mRNA-4157 with pembrolizumab in melanoma patients showed a 40% response rate, compared to 20% with pembrolizumab alone.
The future of personalized mRNA cancer vaccines lies in streamlining their development and expanding their applicability. Advances in AI-driven neoantigen prediction and automated mRNA synthesis could reduce turnaround times from weeks to days, making the treatment more feasible for broader populations. Efforts to develop off-the-shelf mRNA vaccines targeting shared cancer antigens, such as those in KRAS-mutated cancers, could address the scalability issue. For patients, practical tips include maintaining a balanced diet rich in antioxidants to support immune function, staying hydrated during treatment, and reporting any unusual symptoms promptly. As research progresses, these vaccines could become a cornerstone of precision oncology, offering hope to patients with previously untreatable cancers.
Essential Adult Vaccinations: Protecting Your Health at Every Age
You may want to see also
Explore related products






![]()
mRNA vaccines vs. traditional cancer treatments
MRNA vaccines have emerged as a revolutionary approach in cancer treatment, offering a stark contrast to traditional methods like chemotherapy, radiation, and surgery. Unlike these conventional treatments, which often target cancer cells directly but can harm healthy tissues, mRNA vaccines harness the body’s immune system to identify and destroy cancer cells with precision. For instance, Moderna’s mRNA-4157, in combination with Merck’s Keytruda, has shown promising results in melanoma patients, reducing the risk of death or recurrence by 44% in clinical trials. This highlights the potential of mRNA vaccines to complement or even replace traditional treatments in certain cases.
One of the key advantages of mRNA vaccines is their ability to be personalized and rapidly developed. Traditional cancer treatments are often one-size-fits-all, with chemotherapy drugs like cisplatin or carboplatin administered in standardized doses (e.g., 100 mg/m² every 3 weeks) regardless of individual tumor characteristics. In contrast, mRNA vaccines can be tailored to target specific mutations or neoantigens unique to a patient’s cancer, as demonstrated by BioNTech’s individualized mRNA vaccine trials. This customization minimizes side effects and maximizes efficacy, a feat difficult to achieve with broad-acting chemotherapy or radiation.
However, mRNA vaccines are not without limitations. Their success relies on a robust immune response, which can vary widely among patients, particularly in older adults or those with compromised immune systems. Traditional treatments, while harsh, often provide a more immediate and direct assault on cancer cells, making them more suitable for advanced or aggressive cancers. For example, surgery remains the gold standard for localized tumors, and radiation therapy is effective for shrinking tumors before surgery (neoadjuvant therapy) or preventing recurrence (adjuvant therapy). mRNA vaccines, on the other hand, are most effective in early-stage cancers or as part of combination therapy.
Practical considerations also differentiate these approaches. Traditional treatments require frequent hospital visits—chemotherapy sessions every 2–3 weeks, radiation therapy 5 days a week for 6–8 weeks—and often cause severe side effects like nausea, hair loss, and fatigue. mRNA vaccines, typically administered in 2–4 doses over several weeks, have milder side effects, such as injection site pain, fatigue, and fever. For patients, this means a potentially less disruptive treatment experience, though long-term efficacy data for mRNA vaccines are still emerging.
In conclusion, mRNA vaccines represent a paradigm shift in cancer treatment, offering personalized, immune-driven therapy with fewer side effects than traditional methods. However, they are not a universal solution. Traditional treatments remain indispensable for many patients, particularly those with advanced disease. The future of cancer care likely lies in integrating these approaches—using mRNA vaccines for prevention, early-stage treatment, or in combination with chemotherapy or immunotherapy. As research progresses, patients and clinicians will need to weigh the unique benefits and limitations of each method to devise the most effective treatment plans.
Understanding Vaccine Reactions in Children: Causes and Concerns Explained
You may want to see also
Explore related products






![]()
Safety and efficacy in cancer patients
Cancer patients often face unique challenges when it comes to vaccinations, given their compromised immune systems and ongoing treatments. mRNA vaccines, such as those developed for COVID-19, have shown promise in this population, but their safety and efficacy require careful consideration. Clinical trials have demonstrated that mRNA vaccines are generally safe for cancer patients, with side effects similar to those in the general population—fatigue, injection site pain, and mild flu-like symptoms. However, the intensity and duration of these side effects may vary depending on the patient’s cancer type, stage, and concurrent therapies. For instance, patients undergoing chemotherapy or radiation may experience heightened fatigue, though this does not typically outweigh the benefits of vaccination.
Efficacy in cancer patients is a more nuanced issue. Studies indicate that mRNA vaccines can elicit robust immune responses in many cancer patients, particularly those with solid tumors or hematologic malignancies not actively undergoing treatment. However, patients with advanced cancers or those receiving immunosuppressive therapies, such as high-dose corticosteroids or anti-CD20 medications, may mount weaker responses. For example, a 2021 study found that only 60% of patients with hematologic cancers developed adequate antibody titers after two doses of an mRNA COVID-19 vaccine, compared to 90% in the general population. This highlights the need for tailored vaccination strategies, such as additional booster doses or timing vaccinations between treatment cycles to optimize immune response.
Practical considerations are essential for maximizing safety and efficacy in this population. Cancer patients should receive mRNA vaccines as early as possible, ideally before starting immunosuppressive treatments. For those already on treatment, vaccination should be scheduled during periods of relative immune competence, such as 1–2 weeks after chemotherapy or after completing a course of radiation. Dosage remains consistent with the general population (e.g., 30 µg for COVID-19 mRNA vaccines), but close monitoring for adverse reactions is advised. Patients and caregivers should also be educated about the potential for reduced efficacy, emphasizing the importance of continued precautions like masking and social distancing, even after vaccination.
Comparatively, mRNA vaccines offer distinct advantages over traditional vaccines for cancer patients. Their rapid development and adaptability make them ideal for addressing emerging pathogens, and their mechanism of action—stimulating cellular immunity without introducing live pathogens—reduces risks for immunocompromised individuals. For example, mRNA vaccines are being explored in cancer immunotherapy, where they encode tumor-specific antigens to activate T cells against cancer cells. This dual role—preventing infections and potentially treating cancer—positions mRNA technology as a transformative tool in oncology. However, ongoing research is needed to refine dosing, scheduling, and combination strategies to fully unlock their potential in this vulnerable population.
In conclusion, mRNA vaccines are a valuable asset for cancer patients, offering a safe and effective means of protection against infectious diseases. While their efficacy may be diminished in certain subgroups, strategic timing and additional doses can mitigate this limitation. As research progresses, these vaccines may also play a direct role in cancer treatment, further solidifying their importance in oncology. Clinicians should remain proactive in vaccinating cancer patients, balancing the unique challenges of this population with the undeniable benefits of mRNA technology.
Is Tetanus Vaccine Live? Understanding Its Composition and Safety
You may want to see also
Explore related products






![]()
mRNA technology for tumor-specific antigen targeting
MRNA technology has emerged as a transformative tool in cancer immunotherapy, particularly through its ability to target tumor-specific antigens (TSAs). Unlike traditional vaccines, mRNA vaccines encode for specific proteins or peptides unique to cancer cells, training the immune system to recognize and attack tumors with precision. This approach leverages the inherent adaptability of mRNA, allowing for rapid customization to individual tumor profiles, a critical advantage in the heterogeneous landscape of cancer.
Consider the process: mRNA molecules are synthesized to encode TSAs, encapsulated in lipid nanoparticles to protect them from degradation, and delivered to antigen-presenting cells (APCs). Once internalized, the mRNA is translated into proteins, which are then presented on the cell surface, triggering a robust immune response. This mechanism bypasses the need for whole tumor cells or proteins, offering a safer and more targeted alternative. For instance, in melanoma, mRNA vaccines encoding for antigens like MAGE-A3 or NY-ESO-1 have shown promise in clinical trials, with dosages typically ranging from 100 to 200 μg administered intramuscularly or intradermally in multiple cycles.
However, challenges persist. One major hurdle is the identification of truly tumor-specific antigens to minimize off-target effects. While some cancers express well-defined TSAs, others present a complex antigenic landscape, requiring advanced bioinformatics and sequencing technologies to pinpoint viable targets. Additionally, the immunogenicity of mRNA vaccines can vary, necessitating adjuvants or combination therapies to enhance efficacy. For example, pairing mRNA vaccines with checkpoint inhibitors has demonstrated synergistic effects, amplifying the immune response against tumors.
Practical implementation demands careful consideration of patient-specific factors. Age, immune status, and tumor burden influence vaccine efficacy, with younger patients and those with lower disease burden often responding more favorably. Dosage optimization is critical; while higher doses may enhance immunogenicity, they can also increase adverse effects like fever or injection site reactions. Clinicians must balance these factors, often starting with lower doses (e.g., 50 μg) and titrating upward based on tolerance and response.
In conclusion, mRNA technology for tumor-specific antigen targeting represents a paradigm shift in cancer treatment, offering personalized, potent immunotherapy. While technical and biological challenges remain, ongoing research and clinical trials continue to refine this approach, paving the way for its integration into standard oncology practice. For patients and providers alike, understanding the nuances of this technology—from antigen selection to dosing strategies—is essential to harnessing its full potential.
Vaccinated Travellers Quarantine-Free Entry to Australia
You may want to see also
Frequently asked questions
Yes, mRNA vaccines have shown promise in cancer treatment by training the immune system to recognize and attack cancer cells. Clinical trials for mRNA-based cancer vaccines, such as those targeting melanoma and other cancers, have demonstrated encouraging results in boosting immune responses and improving patient outcomes.
mRNA vaccines for cancer deliver genetic instructions to cells, prompting them to produce specific proteins found on cancer cells. This triggers an immune response, where the body’s immune system identifies and targets cancer cells expressing these proteins, potentially slowing tumor growth or eliminating cancer cells.
Current research indicates that mRNA cancer vaccines are generally safe, with side effects similar to those of traditional vaccines, such as fatigue, fever, or injection site pain. However, ongoing studies are refining their safety and efficacy profiles to ensure they are suitable for broader use in cancer treatment.