Live attenuated vaccines are a type of vaccine that uses a weakened (attenuated) form of the live pathogen, such as a virus or bacterium, to induce a protective immune response. Unlike inactivated or subunit vaccines, which contain only parts of the pathogen, live attenuated vaccines mimic a natural infection without causing severe disease. This close resemblance to the actual pathogen triggers a robust immune response, including the production of antibodies and the activation of both humoral and cell-mediated immunity. The immunity induced by live attenuated vaccines is often long-lasting and can provide protection against future infections, sometimes even conferring lifelong immunity. Examples of live attenuated vaccines include those for measles, mumps, rubella, and varicella. However, their use may be limited in immunocompromised individuals due to the risk of the attenuated pathogen causing disease in those with weakened immune systems.
| Characteristics | Values |
|---|---|
| Immunity Type | Active immunity |
| Mechanism of Action | Mimics natural infection, stimulates humoral and cell-mediated immunity |
| Duration of Immunity | Long-lasting, often lifelong |
| Booster Doses | Rarely needed |
| Route of Administration | Oral, nasal, or injection (depending on the vaccine) |
| Examples | Measles, Mumps, Rubella (MMR), Varicella (Chickenpox), Yellow Fever |
| Safety Profile | Generally safe, but may cause mild side effects (e.g., fever, rash) |
| Contraindications | Immunocompromised individuals, pregnant women (for some vaccines) |
| Storage Requirements | Requires refrigeration to maintain viability |
| Immune Response | Induces both systemic and mucosal immunity |
| Interference with Other Vaccines | Minimal, but may require spacing from other live vaccines |
| Reversion to Virulence | Rare, but theoretically possible |
| Cost-Effectiveness | Generally cost-effective due to long-lasting immunity |
| Global Impact | Key in eradication and control of infectious diseases |
Explore related products





What You'll Learn
![]()
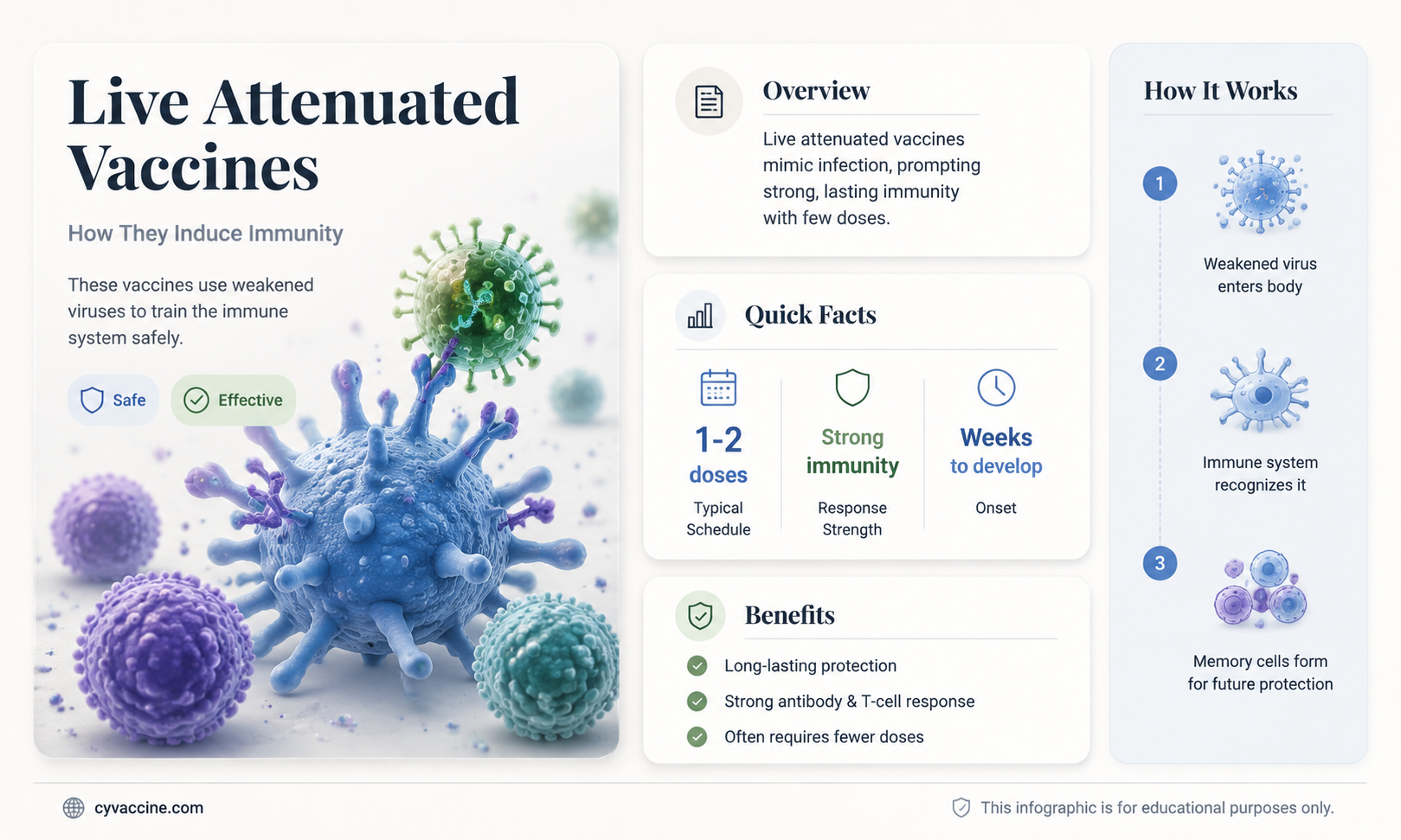
Mechanism of immune response induction by live attenuated vaccines
Live attenuated vaccines (LAVs) mimic natural infection by introducing a weakened but alive pathogen into the body. This design triggers a robust immune response akin to that of a real infection, but without causing severe disease. Unlike inactivated or subunit vaccines, LAVs replicate locally, allowing them to engage both innate and adaptive immune systems more comprehensively. This replication, though limited, ensures sustained antigen presentation, which is critical for the development of long-term immunity. For instance, the measles vaccine contains an attenuated measles virus that replicates in the respiratory tract, stimulating a systemic immune response.
The mechanism begins with the innate immune response, where pattern recognition receptors (PRRs) on antigen-presenting cells (APCs) detect pathogen-associated molecular patterns (PAMPs) on the attenuated pathogen. This detection activates APCs, such as dendritic cells, which then migrate to lymph nodes. Here, they present viral antigens to naive T cells, initiating the adaptive immune response. The attenuated nature of the pathogen ensures that this process occurs without overwhelming the host, striking a balance between immune activation and safety. For example, the yellow fever vaccine (YF-17D) induces a strong CD8+ T cell response, which is essential for viral clearance and memory formation.
One of the key advantages of LAVs is their ability to induce mucosal immunity, a critical defense mechanism against pathogens that enter through mucosal surfaces. The oral polio vaccine (OPV), for instance, is administered orally and replicates in the gut, stimulating the production of IgA antibodies in the intestinal mucosa. This local immune response, combined with systemic immunity, provides dual protection against poliovirus. However, the dosage must be carefully calibrated; too high a dose risks adverse reactions, while too low may fail to induce sufficient immunity. OPV typically contains 10^6 plaque-forming units (PFU) of each Sabin strain, ensuring effective replication without causing disease.
Despite their efficacy, LAVs require careful consideration in immunocompromised individuals, as the attenuated pathogen may revert to a virulent form or cause uncontrolled replication. For example, the varicella vaccine is contraindicated in HIV-positive individuals with CD4 counts below 200 cells/mm³. Additionally, LAVs are generally not recommended for pregnant women or those planning pregnancy within 4 weeks, due to theoretical risks of fetal infection. Practical tips for healthcare providers include storing LAVs at 2–8°C to maintain viability and administering them at the appropriate age—for instance, the MMR vaccine is given at 12–15 months and 4–6 years to ensure optimal immune response.
In conclusion, the mechanism of immune response induction by LAVs hinges on their ability to replicate and persistently present antigens, thereby engaging both innate and adaptive immunity. Their unique capacity to induce mucosal immunity and long-term memory sets them apart from other vaccine types. However, their use demands precision in dosage, storage, and patient selection to maximize benefits while minimizing risks. Understanding these mechanisms not only highlights the elegance of LAV design but also underscores the importance of tailoring vaccination strategies to individual needs.
Why Personnel and Nonhuman Primates Skip TB Vaccinations
You may want to see also
Explore related products






![]()
Duration and strength of immunity from live attenuated vaccines
Live attenuated vaccines, such as those for measles, mumps, rubella (MMR), and varicella (chickenpox), are renowned for inducing robust and long-lasting immunity. Unlike inactivated vaccines, which often require multiple doses and adjuvants to boost immune responses, live attenuated vaccines mimic natural infection, stimulating both humoral and cell-mediated immunity. This dual activation typically results in a stronger and more durable immune memory. For instance, a single dose of the MMR vaccine provides 93% protection against measles, while two doses elevate this to 97%, with immunity persisting for decades in most individuals.
The duration of immunity from live attenuated vaccines is influenced by several factors, including the vaccine’s design, the recipient’s age, and the pathogen’s characteristics. For example, the yellow fever vaccine, another live attenuated product, confers lifelong immunity after a single dose in 99% of recipients. In contrast, the oral typhoid vaccine requires a booster every 3–5 years due to waning immunity. Age also plays a role; infants vaccinated against tuberculosis with the BCG vaccine may require revaccination in adolescence, as immunity can diminish over time. Understanding these variations is critical for tailoring vaccination schedules to maximize protection.
Strength of immunity is another hallmark of live attenuated vaccines, often surpassing that of other vaccine types. This is evident in the case of the smallpox vaccine, which eradicated the disease globally despite being administered decades ago to many still-immune individuals. The mechanism behind this potency lies in the vaccine’s ability to replicate within the host, albeit at a reduced virulence, leading to a sustained immune response. However, this strength comes with a caveat: live vaccines are generally contraindicated in immunocompromised individuals, as the attenuated virus could cause severe illness in those with weakened immune systems.
Practical considerations for optimizing immunity from live attenuated vaccines include adhering to recommended dosing intervals and avoiding simultaneous administration with antiviral medications or immunoglobulins, which can interfere with viral replication. For example, the MMR vaccine should be given at least 14 days before or after receiving immunoglobulin therapy to ensure efficacy. Additionally, maintaining a healthy immune system through proper nutrition and lifestyle supports the vaccine’s ability to induce long-term immunity. For travelers receiving the yellow fever vaccine, ensuring timely administration (at least 10 days before potential exposure) is crucial for full protection.
In summary, live attenuated vaccines offer a unique advantage in terms of both duration and strength of immunity, often providing lifelong protection with minimal doses. However, their effectiveness depends on careful consideration of individual health status, vaccine-specific guidelines, and environmental factors. By understanding these nuances, healthcare providers and recipients can maximize the benefits of these powerful immunological tools, ensuring sustained protection against preventable diseases.
Administering Canine Parainfluenza Bordetella Bronchiseptica Vaccine: A Step-by-Step Guide
You may want to see also
Explore related products






![]()
Role of viral replication in immune system activation
Live attenuated vaccines (LAVs) harness the intrinsic ability of viruses to replicate, albeit at a reduced rate, to stimulate a robust and durable immune response. Unlike inactivated or subunit vaccines, LAVs mimic natural infection by undergoing limited viral replication within the host. This replication is critical because it triggers multiple arms of the immune system simultaneously. For instance, the measles vaccine, a classic LAV, replicates in the respiratory tract and local lymphoid tissues, presenting viral antigens to both innate and adaptive immune cells. This process initiates a cascade of immune activation, including the production of interferons, the recruitment of dendritic cells, and the priming of T and B lymphocytes. The result is a multifaceted immune memory that closely resembles that of a natural infection, often conferring lifelong immunity after a single dose.
Consider the mechanism of viral replication in LAVs as a controlled fire drill for the immune system. When a live attenuated virus enters the body, it begins to replicate at a low level, producing viral proteins that act as danger signals. These signals are detected by pattern recognition receptors (PRRs) on innate immune cells, such as macrophages and dendritic cells. The activation of these cells leads to the release of cytokines and chemokines, which amplify the immune response and recruit additional immune cells to the site of infection. This early innate response is crucial for shaping the subsequent adaptive immune response. For example, the yellow fever vaccine (YF-17D) replicates in the lymph nodes, where it efficiently primes CD8+ T cells and induces neutralizing antibodies, providing protection within 10–14 days of vaccination.
However, the role of viral replication in LAVs is not without challenges. The balance between sufficient replication for immune activation and preventing disease symptoms is delicate. Attenuation is achieved through serial passage of the virus in cell culture or animal hosts, reducing its virulence while preserving immunogenicity. For instance, the oral polio vaccine (OPV) contains attenuated poliovirus strains that replicate in the gastrointestinal tract, inducing mucosal immunity. Yet, in rare cases (approximately 1 in 2.7 million doses), the attenuated virus can revert to a virulent form, causing vaccine-associated paralytic polio (VAPP). This risk underscores the importance of precise attenuation and highlights why inactivated vaccines are preferred in polio eradication efforts in many regions.
Practical considerations for LAV administration further emphasize the role of viral replication. LAVs are typically administered via routes that mimic natural infection, such as oral (e.g., rotavirus vaccine) or intranasal (e.g., influenza vaccine) delivery. These routes allow the virus to replicate in the mucosal tissues, inducing local immunity that can prevent viral entry at the initial site of infection. However, LAVs are contraindicated in immunocompromised individuals, as their impaired immune systems may not control viral replication, leading to severe disease. For example, the varicella vaccine is withheld in patients with HIV or those undergoing chemotherapy, as the attenuated virus could cause disseminated varicella infection.
In conclusion, the role of viral replication in immune system activation is central to the efficacy of live attenuated vaccines. By mimicking natural infection, LAVs engage the immune system in a way that subunit or inactivated vaccines cannot, often providing superior and long-lasting immunity. However, this approach requires careful attenuation and consideration of the host’s immune status to ensure safety. Understanding this mechanism not only highlights the elegance of LAV design but also informs their appropriate use in diverse populations, from healthy children to at-risk adults. For healthcare providers, this knowledge is essential for optimizing vaccine schedules and minimizing adverse events, ensuring that the benefits of LAVs are maximized while risks are mitigated.
Navigating Illinois Vaccine Exemption Form: My Step-by-Step Process
You may want to see also
Explore related products





![]()
Comparison with inactivated vaccines in immunity induction
Live attenuated vaccines (LAVs) and inactivated vaccines represent two distinct approaches to immunity induction, each with unique mechanisms and outcomes. LAVs, such as the measles, mumps, and rubella (MMR) vaccine, use weakened but live pathogens to stimulate a robust immune response. This mimics a natural infection, triggering both humoral (antibody-mediated) and cell-mediated immunity. In contrast, inactivated vaccines, like the injectable polio vaccine (IPV), contain killed pathogens that elicit primarily a humoral response. The key difference lies in the depth and breadth of immunity: LAVs often confer long-lasting, sometimes lifelong immunity after a single or few doses, whereas inactivated vaccines typically require multiple doses and boosters to maintain protection.
Consider the dosage and administration of these vaccines. LAVs, such as the oral typhoid vaccine (Ty21a), are administered in lower doses because the live pathogens replicate within the body, amplifying the immune response. For instance, the yellow fever vaccine (YF-17D) provides lifelong immunity with just one dose. Inactivated vaccines, however, often require higher antigen concentrations and adjuvants to enhance their immunogenicity. The influenza vaccine, for example, is reformulated annually and administered in larger doses to account for the lack of pathogen replication. This highlights a practical advantage of LAVs: fewer doses mean lower costs and better compliance, particularly in pediatric populations where multiple injections can be challenging.
From a safety perspective, LAVs carry a theoretical risk of reversion to virulence, though this is exceedingly rare. The oral polio vaccine (OPV), for instance, has been associated with vaccine-derived poliovirus in immunocompromised individuals. Inactivated vaccines, on the other hand, pose no such risk since the pathogens are completely inactivated. However, their reliance on adjuvants and repeated dosing can lead to increased local reactions, such as pain and swelling at the injection site. For example, the hepatitis A vaccine (Havrix) requires two doses spaced 6–12 months apart, with potential discomfort at each administration. This trade-off between safety and convenience underscores the importance of tailoring vaccine choice to the specific needs of the population.
A critical factor in comparing these vaccines is their efficacy in different age groups. LAVs are particularly effective in young children, whose immune systems are highly responsive to live pathogens. The rotavirus vaccine (Rotarix), for instance, is administered in two doses starting at 6 weeks of age, providing over 90% protection against severe disease. Inactivated vaccines, however, may be less effective in infants due to immune system immaturity and maternal antibody interference. The pertussis vaccine (DTaP), an inactivated component of the combination vaccine, often requires a series of five doses to achieve adequate immunity. This highlights the strategic use of LAVs in early childhood immunization schedules to maximize protection during vulnerable periods.
In conclusion, the choice between live attenuated and inactivated vaccines hinges on balancing immunogenicity, safety, and practicality. LAVs offer the advantage of durable immunity with fewer doses but carry minimal risks in specific populations. Inactivated vaccines provide a safer alternative, particularly for immunocompromised individuals, though they demand more frequent administration. Understanding these nuances allows healthcare providers to optimize vaccine strategies, ensuring broad and sustained immunity across diverse populations. For instance, travelers to endemic areas might benefit from the rapid, robust protection of LAVs, while routine childhood immunizations could incorporate a mix of both types to address specific disease risks effectively.
Investigating Vaccine Deaths: A Guide to Using VAERS Data
You may want to see also
Explore related products



![2 Pack N1N Premium 10 in 1 Immune Support Supplement [10 Potent Ingredients] with Elderberry, Vitamin C, Zinc, Echinacea, Turmeric Curcumin, Garlic and Probiotics for Adults, 120 Veg Caps](https://m.media-amazon.com/images/I/81rvaoUdIqL._AC_UL320_.jpg)

![]()
Potential risks and benefits of live attenuated vaccines
Live attenuated vaccines (LAVs) are a cornerstone of modern immunology, leveraging weakened pathogens to induce robust, long-lasting immunity. Unlike inactivated vaccines, LAVs replicate in the host, mimicking natural infection without causing disease. This replication triggers a potent immune response, often requiring fewer doses for lifelong protection. For instance, the measles, mumps, and rubella (MMR) vaccine, a classic LAV, confers immunity with just two doses, typically administered at 12–15 months and 4–6 years of age. However, this very mechanism—replication of a live pathogen—introduces unique risks and benefits that demand careful consideration.
One of the most significant benefits of LAVs is their ability to stimulate both humoral and cell-mediated immunity, providing comprehensive protection. The yellow fever vaccine, for example, induces neutralizing antibodies and cytotoxic T-cell responses, offering near 100% efficacy after a single 0.5 mL dose. This dual-pronged immune activation is particularly critical for combating intracellular pathogens like viruses. However, the same live nature of these vaccines poses risks, especially in immunocompromised individuals. In rare cases, the attenuated virus can revert to a virulent form or cause severe complications, such as vaccine-associated paralytic poliomyelitis in the oral polio vaccine (OPV). Thus, LAVs are contraindicated in pregnant women, HIV-positive individuals, and those undergoing chemotherapy, highlighting the need for tailored vaccination strategies.
Another advantage of LAVs is their cost-effectiveness and ease of administration, particularly in resource-limited settings. The oral typhoid vaccine (Ty21a) requires no needles, making it ideal for mass immunization campaigns. However, this convenience comes with caveats. LAVs often require strict storage conditions, such as refrigeration, which can be challenging in low-income regions. Additionally, their live nature necessitates careful handling to prevent contamination or accidental exposure. For instance, the smallpox vaccine (Vaccinia) can cause skin infections if not applied correctly, underscoring the importance of trained healthcare personnel.
Despite these risks, LAVs remain indispensable in global health, particularly for controlling infectious diseases with high morbidity and mortality. The varicella vaccine, administered as two 0.5 mL doses, has reduced chickenpox cases by over 90% in the U.S. since its introduction. Yet, the potential for vaccine-strain shedding raises concerns, especially in household contacts of immunocompromised individuals. To mitigate this, recipients of the nasal influenza vaccine (LAIV) are advised to avoid close contact with severely immunocompromised persons for 7 days post-vaccination. Such precautions exemplify the delicate balance between harnessing LAVs' benefits and managing their risks.
In conclusion, live attenuated vaccines offer unparalleled immunological advantages but require vigilant risk management. Their ability to confer durable immunity with minimal doses makes them invaluable tools in disease prevention. However, contraindications, storage requirements, and rare adverse events necessitate careful patient selection and administration. As we advance vaccine technology, understanding and addressing these risks will be crucial to maximizing LAVs' potential while ensuring safety across diverse populations. Practical tips, such as verifying immune status before vaccination and adhering to storage guidelines, can further enhance their efficacy and safety profile.
Should School Vaccinations Be Mandatory? Exploring Pros, Cons, and Ethics
You may want to see also
Frequently asked questions
Live attenuated vaccines are vaccines that contain a weakened (attenuated) form of the live virus or bacteria, which is unable to cause severe disease but can still induce a strong immune response.
Live attenuated vaccines induce immunity by mimicking a natural infection, allowing the immune system to recognize and respond to the weakened pathogen. This response includes the production of antibodies and the activation of memory cells, providing long-lasting protection against the actual disease.
Live attenuated vaccines are often highly effective in inducing immunity because they closely resemble a natural infection, leading to a robust and long-lasting immune response. However, their effectiveness can vary depending on the specific vaccine and individual factors, such as age and immune status.






![Premium 10 in 1 Immune Support Supplement [10 Potent Ingredients] with Elderberry, Vitamin C, Echinacea, Zinc and Probiotic for Immune Support, Gut Health and Better Digestion, 60 Veg Caps](https://m.media-amazon.com/images/I/81oOkSABw-L._AC_UL320_.jpg)