The anti-vaccine movement poses a significant threat to global health by undermining decades of progress in disease prevention and eradication. Fueled by misinformation, conspiracy theories, and mistrust of scientific institutions, this movement has led to declining vaccination rates in many regions, allowing preventable diseases like measles, polio, and COVID-19 to resurge. The World Health Organization (WHO) has identified vaccine hesitancy as one of the top ten global health threats, as it not only endangers individuals but also weakens herd immunity, leaving vulnerable populations, such as the immunocompromised and unvaccinated children, at heightened risk. The spread of anti-vaccine rhetoric, amplified by social media, has created a public health crisis, challenging global efforts to control infectious diseases and achieve health equity. Addressing this threat requires a multifaceted approach, including combating misinformation, rebuilding trust in science, and strengthening healthcare systems to ensure widespread access to vaccines.
Explore related products

$9.99 $14.99





What You'll Learn
![]()
Historical Roots of Anti-Vaccine Sentiment
The anti-vaccine movement, though often portrayed as a modern phenomenon, has deep historical roots that stretch back to the very inception of vaccination. In 1796, Edward Jenner’s smallpox vaccine marked the beginning of immunization, but it also sowed the seeds of skepticism. Early objections were rooted in religious and cultural beliefs, with some viewing vaccination as a violation of divine will or natural order. For instance, in the 19th century, anti-vaccination leagues emerged in the UK, arguing that inoculation interfered with God’s design and introduced animal matter (cowpox) into the human body, a practice deemed unnatural and immoral. These early movements laid the groundwork for future resistance by framing vaccination as an intrusion on personal and spiritual autonomy.
As vaccination became more widespread in the 19th and early 20th centuries, mandatory immunization laws sparked a new wave of opposition. Governments in the UK and the U.S. began requiring smallpox vaccination for schoolchildren and travelers, leading to protests over perceived infringements on individual liberty. The 1904 Royal Commission on Vaccination in the UK highlighted public fears of vaccine side effects, such as severe skin reactions or even death, though these risks were rare. This era introduced the argument that compulsory vaccination was a form of state overreach, a narrative that resonates in today’s debates about vaccine mandates. The anti-vaccine movement of this period also capitalized on mistrust of medical authorities, particularly among marginalized communities, who had historical reasons to distrust government interventions.
The mid-20th century saw the rise of specific controversies that further fueled anti-vaccine sentiment. In the 1970s, the DPT (diphtheria, pertussis, tetanus) vaccine became a focal point of concern after reports of rare but severe side effects, including fever, seizures, and, in extremely rare cases, brain damage. A 1982 documentary, *DPT: Vaccine Roulette*, amplified these fears, leading to a surge in vaccine hesitancy and lawsuits against manufacturers. While scientific studies later debunked many of these claims, the damage was done. This period demonstrated how media and anecdotal evidence could overshadow rigorous scientific data, a pattern that continues to shape anti-vaccine discourse today.
Understanding these historical roots is crucial for addressing contemporary vaccine hesitancy. Early objections based on religion, fears of government overreach, and mistrust of medical institutions have evolved but remain central to modern anti-vaccine arguments. For example, the religious exemptions sought by some parents today echo 19th-century concerns about divine intervention. Similarly, the current debate over COVID-19 vaccine mandates mirrors historical resistance to compulsory immunization. By recognizing these patterns, public health officials can tailor strategies to address specific concerns, such as improving transparency, engaging community leaders, and communicating risks and benefits more effectively. History shows that combating anti-vaccine sentiment requires not just scientific evidence but also empathy and an understanding of the cultural and social contexts driving skepticism.
The Smallpox Vaccine: Why Baby Boomers Bear a Unique Arm Scar
You may want to see also
Explore related products






![]()
Social Media’s Role in Misinformation Spread
Social media platforms have become fertile ground for the rapid dissemination of anti-vaccine misinformation, often overshadowing evidence-based health communication. A single viral post can reach millions within hours, leveraging emotional narratives and pseudoscientific claims to sow doubt about vaccine safety and efficacy. For instance, false assertions linking vaccines to autism or infertility, despite being debunked by rigorous studies, continue to circulate widely on platforms like Facebook, Instagram, and Twitter. This phenomenon is not merely about sharing opinions; it’s about algorithmic amplification, where engagement-driven systems prioritize sensational content over factual accuracy, creating echo chambers that reinforce mistrust.
Consider the mechanics of this spread: social media algorithms are designed to maximize user engagement, often by promoting content that elicits strong emotional responses—fear, anger, or outrage. Anti-vaccine activists exploit this by framing their messages as exposés of hidden truths or calls to protect personal freedoms. For example, during the COVID-19 pandemic, hashtags like #VaccineKills trended alongside misleading videos and testimonials, outpacing public health campaigns in reach and virality. Such content often bypasses fact-checking mechanisms, as platforms struggle to balance free speech with public safety, leaving users to navigate a minefield of misinformation.
To combat this, individuals must adopt critical media literacy skills. Start by verifying the source of information—is it a reputable health organization or an unverified account? Cross-reference claims with trusted databases like the WHO or CDC. For parents, especially those of children aged 0–18, it’s crucial to discuss vaccine safety using age-appropriate language, emphasizing the benefits of immunization in preventing diseases like measles or polio. Tools like reverse image searches and fact-checking websites (e.g., Snopes or PolitiFact) can help debunk false visuals or statistics.
However, the onus cannot rest solely on users. Social media companies must take proactive steps, such as flagging unverified health claims, promoting authoritative sources, and collaborating with health agencies to disseminate accurate information. For instance, during vaccine rollouts, platforms could prioritize posts from verified health professionals or run targeted campaigns debunking common myths. Policymakers also play a role by incentivizing transparency and accountability, ensuring algorithms don’t prioritize profit over public health.
Ultimately, the interplay between social media and anti-vaccine misinformation underscores a broader challenge: balancing technological innovation with societal responsibility. While these platforms have democratized information sharing, their role in amplifying harmful narratives threatens global health initiatives. Addressing this requires a multi-faceted approach—empowering users with critical thinking skills, holding platforms accountable, and fostering collaboration between tech companies and health experts. Without such measures, the digital age risks becoming an era of misinformation-driven health crises.
Global COVID-19 Vaccination Progress: Tracking Worldwide Inoculation Numbers
You may want to see also
Explore related products



$20.46 $21.95



![]()
Impact on Herd Immunity and Outbreaks
The anti-vaccine movement poses a significant threat to herd immunity, the indirect protection that occurs when a large portion of a community becomes immune to a disease, thereby reducing the likelihood of infection for individuals who lack immunity. When vaccination rates drop below the threshold required for herd immunity—typically around 90-95% for highly contagious diseases like measles—outbreaks become more frequent and severe. This is particularly concerning for vulnerable populations, such as infants too young to be vaccinated, immunocompromised individuals, and those with vaccine contraindications. For instance, a single unvaccinated individual can reintroduce a disease into a community, sparking an outbreak that spreads rapidly among the unprotected.
Consider the 2019 measles outbreak in the United States, which saw nearly 1,300 cases across 31 states—the highest number in over 25 years. This resurgence was directly linked to declining vaccination rates in certain communities, fueled by misinformation and vaccine hesitancy. Measles, one of the most contagious viruses, requires at least 93-95% vaccination coverage to maintain herd immunity. In areas where vaccination rates fell below this threshold, the disease spread unchecked, leading to hospitalizations, complications like pneumonia and encephalitis, and even deaths. This example underscores how localized anti-vaccine sentiment can have far-reaching consequences, undermining global health security.
To mitigate the impact on herd immunity, public health strategies must focus on education, accessibility, and policy. Educating communities about the safety and efficacy of vaccines is critical, as is addressing misinformation through trusted sources like healthcare providers and scientific institutions. For example, the World Health Organization (WHO) recommends tailored communication strategies that address specific concerns, such as the debunked link between the MMR vaccine and autism. Additionally, ensuring vaccine accessibility—through affordable pricing, mobile clinics, and school-based programs—can help close immunization gaps. Policymakers should also consider measures like vaccine mandates for school entry, with exemptions limited to medical reasons, to maintain high vaccination rates.
A comparative analysis of countries with strong vaccination programs, such as Rwanda and Australia, reveals the effectiveness of these strategies. Rwanda, with its robust immunization infrastructure and community health worker networks, achieved 97% measles vaccination coverage in 2020. Australia’s "No Jab, No Pay" policy, which withholds certain welfare payments from parents who refuse to vaccinate their children, has contributed to vaccination rates above 94%. These examples demonstrate that a combination of education, accessibility, and policy enforcement can sustain herd immunity even in the face of global anti-vaccine movements.
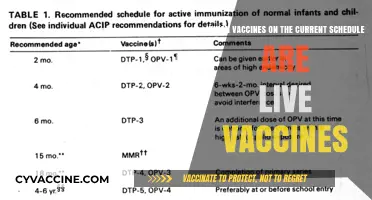
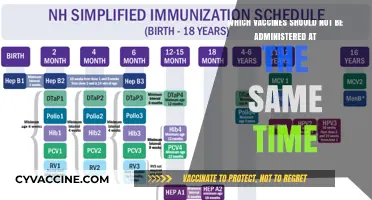
Ultimately, the erosion of herd immunity due to vaccine hesitancy creates a breeding ground for outbreaks, reversing decades of progress in disease control. Practical steps for individuals include staying informed through credible sources, adhering to recommended vaccination schedules (e.g., the CDC’s guidelines for childhood immunizations), and advocating for evidence-based policies. For healthcare providers, engaging in open, empathetic conversations with hesitant patients can help address concerns and build trust. By collectively prioritizing vaccination, societies can protect not only themselves but also the most vulnerable among us, ensuring that preventable diseases remain a relic of the past.
Add Your Vaccine Status to Apple Wallet: A Simple Guide
You may want to see also
Explore related products






![]()
Political and Religious Influences on Vaccine Refusal
Political ideologies often intersect with public health policies, creating fertile ground for vaccine refusal. In some regions, skepticism toward government mandates has been weaponized by political factions to undermine vaccination efforts. For instance, during the COVID-19 pandemic, certain political groups in the United States framed vaccine mandates as an infringement on personal liberty, leveraging this narrative to mobilize supporters against immunization. This politicization not only eroded trust in health institutions but also exacerbated vaccine hesitancy, particularly among specific demographic groups. A 2021 study published in *Nature Medicine* found that counties with higher support for political candidates who criticized vaccine mandates saw significantly lower vaccination rates, highlighting the direct impact of political rhetoric on public health outcomes.
Religious beliefs, while deeply personal, can also shape attitudes toward vaccines, sometimes leading to refusal. Historically, some religious communities have opposed vaccination based on concerns about the use of fetal cell lines in vaccine development or perceived conflicts with spiritual purity. For example, a small but vocal minority within certain Christian and Islamic groups has cited religious grounds for declining vaccines, despite assurances from religious leaders that immunization aligns with faith principles. In Nigeria, polio eradication efforts were initially hindered by rumors that the vaccine was a Western plot to sterilize Muslim populations, demonstrating how religious mistrust can be manipulated to thwart public health initiatives. Addressing these concerns requires culturally sensitive communication that respects religious values while clarifying the safety and necessity of vaccines.
The convergence of political and religious influences can amplify vaccine refusal, particularly in communities where these two forces are deeply intertwined. In India, for instance, political parties have occasionally aligned with religious leaders to spread misinformation about vaccines, such as false claims linking the measles-rubella vaccine to infertility. This dual-pronged approach not only sows doubt but also creates a sense of collective identity among those who reject vaccines, making it harder for public health campaigns to penetrate these communities. To counter this, health officials must engage local leaders—both political and religious—to build trust and disseminate accurate information, ensuring that messaging resonates with cultural and ideological norms.
Practical strategies to mitigate political and religious influences on vaccine refusal include fostering dialogue between health experts and community leaders, tailoring communication to address specific concerns, and leveraging trusted figures to endorse vaccination. For example, in Pakistan, involving imams in polio vaccination campaigns helped dispel religious misconceptions and increased vaccine acceptance. Similarly, in politically polarized regions, framing vaccination as a non-partisan issue focused on community well-being can reduce ideological barriers. By understanding the unique dynamics at play, public health efforts can navigate these complex influences more effectively, safeguarding global health against the threat of vaccine refusal.
Vaccines Save Lives: Simplifying the Science for Skeptics
You may want to see also
Explore related products






![]()
Economic and Health System Burdens from Vaccine Hesitancy
Vaccine hesitancy imposes staggering economic costs on societies, often overlooked in debates about individual choice. A single measles outbreak in the U.S. can cost up to $1 million in public health response efforts, including contact tracing, vaccination clinics, and hospital care. For instance, the 2019 measles outbreak in Washington State cost $3.4 million to contain, diverting resources from other critical health programs. Globally, the WHO estimates that vaccine hesitancy contributes to over 1.5 million preventable deaths annually, each representing not just a human tragedy but also a financial burden. When vaccination rates drop below 95%, herd immunity falters, leading to outbreaks that strain healthcare systems and economies alike.
Consider the indirect economic impacts: a child hospitalized with a vaccine-preventable disease may require weeks of intensive care, costing tens of thousands of dollars. Parents may need to take unpaid leave, reducing household income and productivity. Schools and workplaces face closures during outbreaks, further disrupting economic activity. For example, the 2017 measles outbreak in Minnesota cost the state $1.3 million in public health response, while families incurred additional costs for medical care and lost wages. These ripple effects highlight how vaccine hesitancy undermines not just public health but also economic stability.
Health systems bear the brunt of vaccine hesitancy, particularly in low-resource settings. In countries like the Philippines, the 2017 dengue vaccine controversy led to a dramatic drop in vaccine confidence, resulting in a 30% decline in childhood immunization rates. This collapse allowed diseases like measles to resurge, overwhelming hospitals and depleting medical supplies. In 2019, the Philippines recorded over 43,000 measles cases, with 570 deaths, many of them children. Such outbreaks force health systems to reallocate resources from chronic disease management and preventive care to emergency response, creating long-term inefficiencies.
To mitigate these burdens, policymakers must invest in targeted interventions. For instance, the WHO’s Tailoring Immunization Programmes (TIP) initiative uses data-driven strategies to address hesitancy, such as training healthcare workers to communicate vaccine benefits effectively. In India, the introduction of text message reminders increased vaccination rates by 12%, demonstrating the power of simple, cost-effective solutions. Governments should also prioritize economic incentives, such as tax breaks for employers who offer paid leave for vaccination or subsidies for low-income families to access vaccines. By addressing hesitancy proactively, societies can reduce the economic and health system burdens that threaten global health security.
Is Hep B Vaccine Mandatory for Colorado School Children?
You may want to see also
Frequently asked questions
The anti-vaccine movement is a group of individuals and organizations that oppose vaccination, often spreading misinformation about vaccine safety and efficacy. It is considered a threat to global health because it undermines herd immunity, leading to outbreaks of preventable diseases like measles, polio, and COVID-19, endangering vulnerable populations and straining healthcare systems.
The anti-vaccine movement disrupts global immunization efforts by eroding public trust in vaccines, leading to lower vaccination rates. This allows vaccine-preventable diseases to resurge, reversing decades of progress in disease eradication and increasing the risk of pandemics.
Social media platforms amplify anti-vaccine misinformation by providing a rapid and widespread means of dissemination. Algorithms often prioritize sensational or controversial content, making it easier for false claims to reach large audiences, even when they are debunked by scientific evidence.
The anti-vaccine movement has gained traction in various regions, including North America, Europe, and parts of Asia. Countries with high internet penetration and access to social media, such as the United States, France, and Japan, have seen significant anti-vaccine activity, impacting local and global health outcomes.
Countering the anti-vaccine movement requires a multi-faceted approach, including public education campaigns based on scientific evidence, stricter regulation of misinformation on social media, and strengthening healthcare systems to provide accurate information. Building trust in health authorities and fostering community engagement are also crucial.