The current vaccination schedule includes several types of vaccines, among which live attenuated vaccines play a crucial role in providing immunity against specific diseases. Live vaccines contain a weakened form of the virus or bacteria, which stimulates the immune system to produce a protective response without causing the disease itself. Examples of live vaccines on the current schedule include the measles, mumps, and rubella (MMR) vaccine, the varicella (chickenpox) vaccine, the rotavirus vaccine, and the intranasal influenza vaccine. These vaccines are highly effective and typically require fewer doses compared to inactivated or subunit vaccines. However, they may not be suitable for individuals with compromised immune systems or certain medical conditions, making it essential to consult healthcare providers for personalized recommendations.
Explore related products






What You'll Learn
- MMR Vaccine: Measles, Mumps, Rubella combined vaccine uses live attenuated viruses for immunity
- Varicella Vaccine: Live attenuated varicella-zoster virus prevents chickenpox effectively
- Rotavirus Vaccine: Oral vaccine with live attenuated rotavirus strains for infants
- Yellow Fever Vaccine: Live attenuated virus protects against yellow fever disease
- Shingles Vaccine: Contains live attenuated varicella-zoster virus for shingles prevention
![]()
MMR Vaccine: Measles, Mumps, Rubella combined vaccine uses live attenuated viruses for immunity
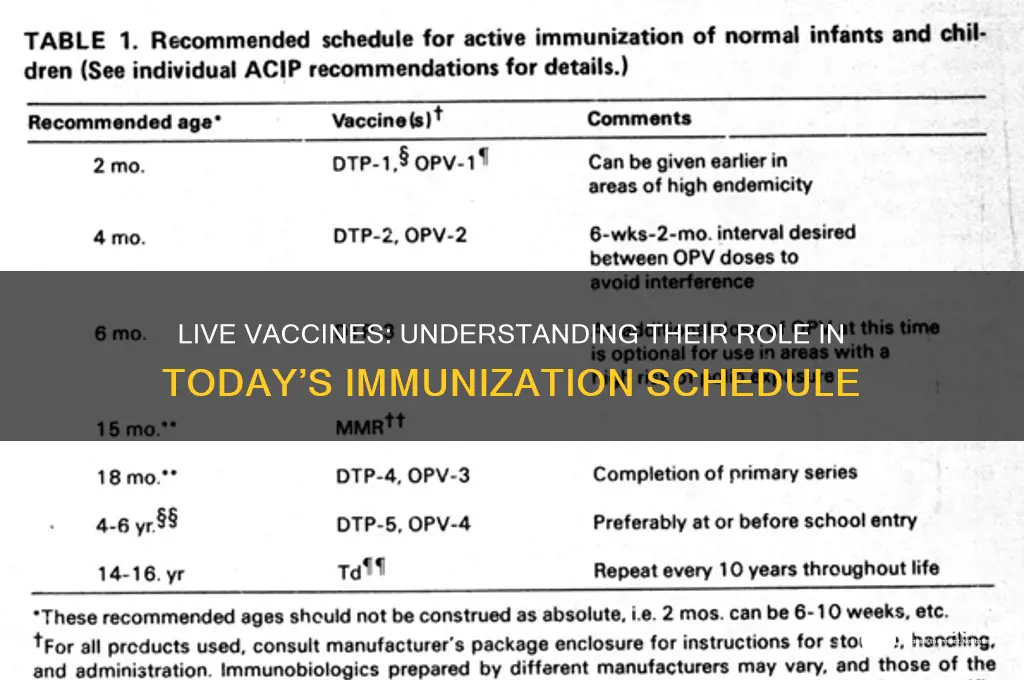
The MMR vaccine stands as a cornerstone in modern immunization, protecting against three highly contagious diseases: measles, mumps, and rubella. Unlike some vaccines that use inactivated or subunit components, the MMR vaccine employs live attenuated viruses. This means the viruses are weakened to the point where they cannot cause disease in healthy individuals but are still potent enough to trigger a robust immune response. This approach mimics a natural infection, prompting the body to produce antibodies and memory cells that confer long-lasting immunity.
Administered typically in two doses, the first dose is given at 12–15 months of age, and the second dose at 4–6 years. This schedule ensures optimal protection during childhood, when susceptibility to these diseases is highest. The vaccine’s efficacy is remarkable, with over 97% effectiveness against measles and mumps and 90% against rubella after two doses. However, it’s crucial to note that the MMR vaccine is contraindicated for individuals with severe immunodeficiency or pregnant women, as live attenuated vaccines carry a theoretical risk of harm in these populations.
One of the MMR vaccine’s unique strengths lies in its ability to prevent not just individual diseases but also their severe complications. Measles, for instance, can lead to pneumonia, encephalitis, and even death, while mumps can cause deafness and meningitis. Rubella, though mild in children, poses a grave risk to pregnant women, potentially leading to congenital rubella syndrome, which can result in miscarriages, stillbirths, or severe birth defects. By preventing these diseases, the MMR vaccine safeguards both individual health and public health by reducing disease transmission.
Practical considerations for parents and caregivers include monitoring for mild side effects, such as fever, rash, or soreness at the injection site, which typically resolve within a few days. Rarely, more serious reactions like allergic responses may occur, necessitating immediate medical attention. Storing the vaccine properly—between 2°C and 8°C—is critical for healthcare providers, as exposure to heat or light can degrade the live viruses. For those traveling to regions with measles outbreaks, ensuring MMR vaccination is up to date is essential, as measles remains a global threat despite being largely controlled in many developed countries.
In summary, the MMR vaccine’s use of live attenuated viruses exemplifies the power of immunization to prevent disease and its complications. Its dual-dose schedule, high efficacy, and broad protective benefits make it a vital component of childhood vaccination programs. By understanding its mechanism, administration guidelines, and contraindications, individuals and healthcare providers can maximize its impact, contributing to a healthier, disease-resistant population.
Preventing Tetanus Naturally: Safe Strategies for the Unvaccinated
You may want to see also
Explore related products






![]()
Varicella Vaccine: Live attenuated varicella-zoster virus prevents chickenpox effectively
The varicella vaccine, a live attenuated formulation of the varicella-zoster virus, stands as a cornerstone in preventing chickenpox, a highly contagious disease caused by this virus. Unlike inactivated vaccines, which use killed pathogens, live attenuated vaccines contain a weakened version of the virus, capable of inducing a robust immune response without causing the disease in healthy individuals. This mechanism not only confers long-lasting immunity but also mimics natural infection, stimulating both humoral and cell-mediated immunity. Administered typically in two doses—the first at 12 to 15 months of age and the second at 4 to 6 years—this vaccine has dramatically reduced the incidence of chickenpox and its complications, such as bacterial infections, pneumonia, and encephalitis.
From a practical standpoint, the varicella vaccine is a critical component of the childhood immunization schedule, yet its administration requires careful consideration. The vaccine is contraindicated in individuals with severe immunodeficiency, pregnant women, and those with a history of severe allergic reactions to its components. Mild side effects, such as soreness at the injection site, fever, or a mild rash, are common but typically resolve within a few days. A unique aspect of this live vaccine is its potential to cause a mild, localized rash resembling chickenpox in some recipients, a sign of the immune system’s response rather than a full-blown infection. Parents and caregivers should monitor children post-vaccination and consult healthcare providers if unusual symptoms arise.
Comparatively, the varicella vaccine’s efficacy underscores the broader success of live attenuated vaccines in disease prevention. Studies show that two doses provide over 90% protection against moderate to severe chickenpox and significantly reduce the risk of breakthrough infections. This contrasts with the pre-vaccine era, when nearly all children contracted chickenpox, often leading to widespread school absences and healthcare burdens. The vaccine’s impact extends beyond individual protection, contributing to herd immunity and reducing viral circulation in communities. Its inclusion in routine immunization schedules globally reflects its proven safety and effectiveness.
Persuasively, the varicella vaccine exemplifies the balance between scientific innovation and public health impact. By preventing chickenpox, it also mitigates the risk of shingles later in life, as the varicella-zoster virus can reactivate as herpes zoster in individuals who have had chickenpox. This dual benefit highlights the vaccine’s long-term value, particularly in regions with high varicella prevalence. However, vaccine hesitancy remains a challenge, fueled by misinformation about safety and efficacy. Educating the public about the rigorous testing and monitoring of live attenuated vaccines, including varicella, is essential to maintaining high vaccination rates and sustaining disease control.
In conclusion, the varicella vaccine’s role as a live attenuated preventive measure against chickenpox is a testament to its design and effectiveness. Its inclusion in the immunization schedule not only protects children from a once-common illness but also reduces the societal and economic burdens of the disease. By understanding its mechanism, administration guidelines, and broader benefits, individuals and healthcare providers can make informed decisions, ensuring continued success in varicella prevention. This vaccine remains a vital tool in the fight against infectious diseases, demonstrating the power of live attenuated technology in modern medicine.
Trump's Role in COVID-19 Vaccine Development
You may want to see also
Explore related products






![]()
Rotavirus Vaccine: Oral vaccine with live attenuated rotavirus strains for infants
The rotavirus vaccine stands out as a pivotal live vaccine in the current immunization schedule, specifically designed to protect infants from severe diarrhea and dehydration caused by rotavirus infections. Unlike many other vaccines that are injected, this one is administered orally, making it particularly convenient for young children. The vaccine contains live attenuated rotavirus strains, which are weakened versions of the virus that stimulate the immune system without causing the disease. This method of delivery mimics natural infection, leading to robust immunity in the gut, where rotavirus primarily attacks.
Administering the rotavirus vaccine requires careful timing and adherence to dosage guidelines. Typically, the vaccine is given in a series of two or three doses, depending on the brand. The first dose is recommended at 2 months of age, with subsequent doses administered at 4-month intervals, usually concluding by 6 months. It’s crucial to follow the healthcare provider’s schedule, as deviations can reduce effectiveness. The oral formulation allows for easy administration, often requiring just a few drops placed directly into the infant’s mouth. Parents should ensure the child swallows the vaccine, as spitting it out could compromise its efficacy.
One of the most compelling aspects of the rotavirus vaccine is its impact on global health. Before its introduction, rotavirus was the leading cause of severe diarrheal disease in infants and young children worldwide, resulting in hundreds of thousands of deaths annually, primarily in low-income countries. Since its inclusion in routine immunization schedules, hospitalizations and deaths related to rotavirus have plummeted by over 80% in countries with high vaccination coverage. This success underscores the vaccine’s role as a lifesaving intervention, particularly in regions with limited access to medical care.
Despite its benefits, the rotavirus vaccine is not without considerations. Mild side effects, such as temporary diarrhea, fussiness, or vomiting, may occur but are generally short-lived. Rarely, a condition called intussusception, a type of bowel blockage, has been associated with the vaccine. However, the risk is extremely low (about 1 in 20,000 to 100,000 doses) and pales in comparison to the risks posed by a rotavirus infection itself. Healthcare providers often emphasize that the vaccine’s protective benefits far outweigh these minimal risks.
Practical tips for parents include scheduling vaccinations during calm periods in the infant’s day and monitoring for any unusual symptoms post-vaccination. Keeping the child hydrated and maintaining a normal feeding routine can help mitigate minor side effects. Additionally, parents should store the vaccine properly if it is administered at home, though this is rare, as most doses are given in healthcare settings. By understanding the specifics of the rotavirus vaccine, caregivers can ensure their infants receive this critical protection during their most vulnerable months.
Leptospirosis Vaccine Coverage: How Many Strains Are Protected?
You may want to see also
Explore related products






![]()
Yellow Fever Vaccine: Live attenuated virus protects against yellow fever disease
The yellow fever vaccine stands as a cornerstone in the fight against a disease that has historically ravaged populations, particularly in tropical regions of Africa and Central and South America. Unlike inactivated vaccines, which use killed pathogens, the yellow fever vaccine is a live attenuated vaccine, meaning it contains a weakened form of the virus that still elicits a robust immune response without causing the disease. This approach has proven highly effective, offering lifelong immunity with a single dose for most individuals. Administered subcutaneously, typically in the deltoid muscle for adults and the anterolateral thigh for infants, the vaccine is recommended for individuals aged 9 months and older traveling to or living in endemic areas. Its efficacy is remarkable, with studies showing over 99% seroprotection rates within 30 days of vaccination.
From a practical standpoint, the yellow fever vaccine is not just a medical intervention but a travel requirement for many. Countries with a risk of yellow fever transmission may mandate proof of vaccination (via an International Certificate of Vaccination or Prophylaxis) for entry, particularly if travelers are arriving from endemic zones. This makes the vaccine a critical consideration for globetrotters and expatriates alike. However, it’s not without caveats. Certain groups, such as pregnant women, individuals with severe egg allergies, or those with compromised immune systems, may require careful evaluation before receiving the vaccine. For instance, pregnant women should only be vaccinated if the risk of yellow fever exposure is high and cannot be avoided, while those with egg allergies may still receive the vaccine under medical supervision due to the low egg protein content in the formulation.
Comparatively, the yellow fever vaccine’s live attenuated nature sets it apart from other vaccines on the schedule, such as the measles, mumps, and rubella (MMR) vaccine, which also uses live attenuated viruses. While both vaccines provide long-lasting immunity, the yellow fever vaccine’s single-dose regimen contrasts with the MMR’s two-dose requirement. This simplicity makes it particularly valuable in resource-limited settings, where follow-up doses can be challenging to administer. Moreover, the yellow fever vaccine’s safety profile is well-established, with rare but serious side effects such as yellow fever vaccine-associated viscerotropic disease (YEL-AVD) or neurological reactions occurring in approximately 0.3–0.4 cases per 100,000 doses. These risks, though minimal, underscore the importance of targeted vaccination strategies.
Persuasively, the yellow fever vaccine exemplifies the power of live attenuated vaccines in disease prevention. Its ability to confer lifelong immunity with a single dose not only protects individuals but also contributes to herd immunity, reducing the virus’s spread in endemic regions. For travelers, it’s a non-negotiable safeguard against a disease with a 30–60% fatality rate in severe cases. Practical tips include scheduling vaccination at least 10 days before travel to ensure immunity takes effect and storing the International Certificate of Vaccination in a secure, accessible place. Additionally, travelers should remain vigilant about mosquito bite prevention, as the vaccine, while highly effective, does not eliminate the risk of exposure to the virus.
In conclusion, the yellow fever vaccine is a testament to the ingenuity of live attenuated vaccines, offering a simple yet powerful solution to a historically devastating disease. Its unique characteristics—single-dose efficacy, travel-related mandates, and targeted precautions—make it a standout in the vaccine schedule. By understanding its specifics and adhering to guidelines, individuals can protect themselves and contribute to global efforts to control yellow fever. Whether for travel or residence in endemic areas, this vaccine remains an indispensable tool in public health.
Natural Immunity vs. Vaccines: CDC Insights on Protection and Safety
You may want to see also
Explore related products






![]()
Shingles Vaccine: Contains live attenuated varicella-zoster virus for shingles prevention
The shingles vaccine, known as Shingrix, stands out in the immunization schedule due to its unique composition: it contains a live attenuated varicella-zoster virus (VZV), the same virus responsible for both chickenpox and shingles. Unlike its predecessor, Zostavax, which was also a live vaccine but less effective, Shingrix uses a subunit of the VZV glycoprotein E combined with an adjuvant to stimulate a stronger immune response. This innovation has significantly improved shingles prevention, particularly in older adults who are most at risk. Administered in two doses, typically 2 to 6 months apart, Shingrix is recommended for individuals aged 50 and older, regardless of whether they’ve had shingles before or received Zostavax. Its efficacy rate of over 90% in preventing shingles and its complications, such as postherpetic neuralgia, makes it a cornerstone of adult vaccination strategies.
Understanding the mechanism of Shingrix is key to appreciating its role as a live vaccine. The live attenuated virus in the vaccine is weakened to the point where it cannot cause disease in healthy individuals but is still potent enough to trigger a robust immune response. This response not only prevents shingles but also reduces the severity of the disease if it does occur. However, the live nature of the vaccine means it is not suitable for everyone. Immunocompromised individuals, pregnant women, and those with a history of severe allergic reactions to vaccine components should avoid Shingrix. For eligible candidates, the vaccine’s side effects, such as arm pain, fatigue, and mild fever, are generally short-lived and far outweighed by the benefits of protection.
Comparing Shingrix to other live vaccines on the schedule, such as MMR (measles, mumps, rubella) or varicella (chickenpox), highlights its specialized purpose. While MMR and varicella vaccines target childhood diseases, Shingrix addresses a condition that predominantly affects older adults. This age-specific focus underscores the importance of tailoring vaccination strategies to different life stages. Additionally, Shingrix’s two-dose regimen differs from the single-dose approach of many childhood live vaccines, reflecting the need for a stronger immune boost in aging populations. This distinction also emphasizes the vaccine’s role in preventing a reactivation of VZV, rather than an initial infection, making it a unique tool in the fight against shingles.
Practical considerations for receiving the shingles vaccine include scheduling and cost. The CDC recommends Shingrix for all adults aged 50 and older, even if they’ve had shingles or received Zostavax previously. While the vaccine is widely available at pharmacies and healthcare providers, its cost can vary, and insurance coverage is not universal. Patients should verify their coverage or explore assistance programs to ensure affordability. Timing the doses correctly is also crucial; delaying the second dose beyond 6 months may reduce the vaccine’s effectiveness. Finally, individuals should plan for potential side effects, such as arm soreness, by scheduling the vaccine when they can rest if needed. By addressing these logistical aspects, individuals can maximize the benefits of Shingrix and take a proactive step toward shingles prevention.
The US Transition to Two MMR Vaccines: A Timeline
You may want to see also
Frequently asked questions
Live vaccines on the current schedule include MMR (Measles, Mumps, Rubella), Varicella (Chickenpox), Rotavirus, and some formulations of the Flu vaccine (nasal spray).
Live vaccines are generally safe for most people, but they may not be recommended for individuals with weakened immune systems, pregnant women, or those with certain medical conditions. Consult a healthcare provider for personalized advice.
Live vaccines use weakened (attenuated) forms of the virus or bacteria to trigger an immune response, while inactivated vaccines use killed pathogens or parts of them. Live vaccines often provide stronger, longer-lasting immunity but have more precautions.
Live vaccines can cause mild symptoms similar to the disease (e.g., a mild rash after the MMR vaccine), but they do not cause the full-blown disease in healthy individuals. Serious reactions are extremely rare.