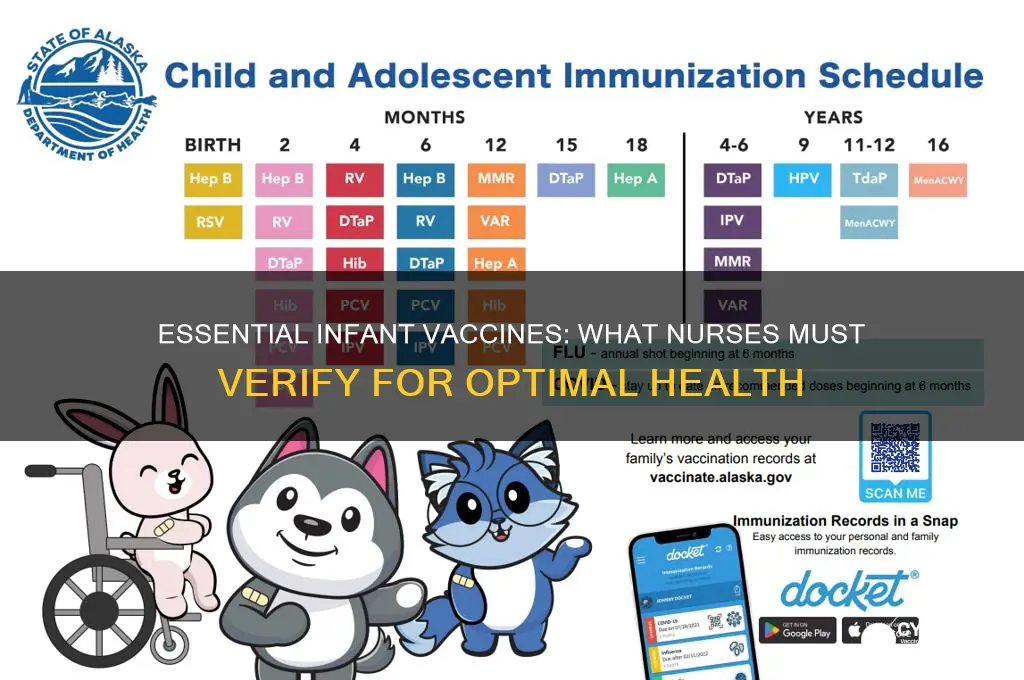
When caring for infants, it is crucial for nurses to verify that they have received the appropriate vaccinations according to the recommended immunization schedule. Key vaccines to confirm include the Hepatitis B (HepB) vaccine, typically administered at birth, followed by the first doses of DTaP (Diphtheria, Tetanus, and Pertussis), Hib (Haemophilus influenzae type b), IPV (Inactivated Poliovirus), PCV (Pneumococcal Conjugate), and RV (Rotavirus) vaccines starting at 2 months of age. Additionally, nurses should ensure the infant has received the first dose of the Influenza vaccine, if applicable, and be prepared to educate parents on the importance of timely immunizations to protect against preventable diseases.
| Characteristics | Values |
|---|---|
| Age Range | Birth to 2 years old |
| Vaccines to Verify | Hepatitis B (HepB), Rotavirus (RV), Diphtheria, Tetanus, Pertussis (DTaP), Haemophilus influenzae type b (Hib), Pneumococcal conjugate (PCV), Inactivated Poliovirus (IPV), Influenza (Flu), Measles, Mumps, Rubella (MMR) |
| Hepatitis B (HepB) | Birth dose within 24 hours, followed by 2-3 doses in the first year |
| Rotavirus (RV) | 2 or 3 doses starting at 2 months, depending on the brand |
| DTaP (Diphtheria, Tetanus, Pertussis) | 3-4 doses starting at 2 months, with boosters at 4 months and 6 months |
| Hib (Haemophilus influenzae type b) | 3-4 doses starting at 2 months, with boosters at 4 months and 6 months |
| PCV (Pneumococcal conjugate) | 3-4 doses starting at 2 months, with boosters at 4 months and 6 months |
| IPV (Inactivated Poliovirus) | 3-4 doses starting at 2 months, with boosters at 4 months and 6 months |
| Influenza (Flu) | Annual dose starting at 6 months, with 2 doses in the first year if new |
| MMR (Measles, Mumps, Rubella) | First dose at 12-15 months, second dose at 4-6 years |
| Source Guidelines | CDC (Centers for Disease Control and Prevention) Immunization Schedule |
| Verification Method | Review immunization records, parent reports, or state immunization registry |
| Importance | Ensures compliance with recommended schedule, prevents vaccine-preventable diseases |
Explore related products






What You'll Learn
![]()
Hepatitis B vaccine verification
The Hepatitis B vaccine is a critical component of an infant's immunization schedule, and its verification is a vital task for nurses to ensure timely protection against this potentially life-threatening liver infection. This vaccine is unique as it is one of the first vaccines administered to newborns, ideally within the first 12 hours of life, followed by a series of doses to establish long-term immunity.
Dosage and Schedule: The recommended schedule for the Hepatitis B vaccine is a series of three doses. The initial dose, as mentioned, is given at birth, with the second dose administered at 1-2 months of age, and the final dose at 6-18 months. This timing is crucial, as it provides the best protection during the early stages of life when the risk of infection is highest. Each dose is typically 0.5 mL, injected intramuscularly, with the deltoid muscle being the preferred site for older infants.
Verification Process: Nurses play a pivotal role in ensuring this vaccine series is completed. Upon admission or during regular check-ups, nurses should review the infant's immunization records, paying close attention to the Hepatitis B vaccine status. If the initial birth dose is missing or uncertain, it is imperative to administer it as soon as possible, even if the infant is beyond the typical newborn period. This is because the risk of Hepatitis B transmission from an infected mother to her child during birth is significant, and the vaccine is highly effective in preventing this.
A practical tip for nurses is to educate parents about the importance of this vaccine, especially if there is any hesitation or concern. Emphasizing that Hepatitis B can lead to chronic liver disease and liver cancer later in life can help parents understand the urgency and long-term benefits of this early vaccination. Additionally, nurses should be aware of the potential side effects, which are generally mild and may include soreness at the injection site, fever, or irritability, and provide appropriate advice for management.
In summary, Hepatitis B vaccine verification is a critical aspect of infant care, requiring nurses to be vigilant and proactive. By adhering to the recommended schedule and promptly addressing any gaps in vaccination, healthcare providers can significantly contribute to the prevention of Hepatitis B and its associated complications. This simple yet essential task can have a profound impact on an infant's long-term health.
Exploring Tick-Borne Disease Prevention: Is a Human Vaccine Possible?
You may want to see also
Explore related products






![]()
DTaP (Diphtheria, Tetanus, Pertussis) vaccine confirmation
Nurses play a critical role in ensuring infants receive the DTaP vaccine, a combination shot protecting against diphtheria, tetanus, and pertussis. This vaccine is administered in a series of doses, typically starting at 2 months of age, followed by additional doses at 4 months, 6 months, 15-18 months, and 4-6 years. Each dose is crucial for building immunity, as the initial shots prime the immune system, and subsequent doses strengthen the response. Verification of these doses is essential, as incomplete series leave infants vulnerable to preventable diseases.
The DTaP vaccine’s dosage schedule is precise, with each dose containing 15-20 international units (IU) of diphtheria toxoid, 5-10 IU of tetanus toxoid, and 3-5 IU of pertussis antigens. Nurses must confirm not only the timing of doses but also the specific vaccine brand used, as formulations may vary slightly. For instance, some brands include acellular pertussis components, which are safer for infants than older whole-cell versions. Documentation should reflect both the date and brand to ensure continuity of care, especially if the infant receives doses at different healthcare facilities.
One practical challenge in DTaP verification is addressing parental hesitancy or misinformation. Nurses should be prepared to explain the vaccine’s safety profile, emphasizing that side effects like mild fever or soreness are far outweighed by the risks of the diseases it prevents. For example, pertussis (whooping cough) can be life-threatening in infants, causing severe respiratory distress, while tetanus can lead to fatal muscle spasms. Clear, empathetic communication can alleviate concerns and reinforce the importance of completing the series.
In cases where an infant misses a scheduled dose, nurses must follow catch-up guidelines. The minimum interval between doses is 4 weeks, but the series can be extended without restarting. For older infants or toddlers who fall behind, the final dose should be administered by age 6, ensuring long-term immunity. Nurses should also verify that premature infants receive doses based on chronological age, not adjusted age, as per CDC recommendations. This attention to detail ensures no child slips through the cracks.
Finally, nurses should leverage immunization records and registries to streamline DTaP verification. Tools like state immunization information systems (IIS) or electronic health records (EHRs) provide a centralized view of an infant’s vaccination history. Cross-referencing these records with parental recall can help identify gaps or discrepancies. By staying organized and proactive, nurses not only confirm compliance but also build trust with families, fostering a culture of preventive care.
Understanding Australia's Whooping Cough Vaccine: What is it Called?
You may want to see also
Explore related products






![]()
Hib (Haemophilus influenzae type b) vaccine check
The Hib vaccine is a critical component of an infant's immunization schedule, protecting against Haemophilus influenzae type b, a bacterium that can cause severe infections such as meningitis, pneumonia, and epiglottitis. Nurses play a vital role in verifying that infants receive this vaccine according to the recommended schedule. The Centers for Disease Control and Prevention (CDC) advises a series of doses starting at 2 months of age, with subsequent doses at 4 months and 6 months, followed by a booster at 12-15 months. This staggered approach ensures robust immunity during the period when infants are most vulnerable to Hib-related diseases.
Verification of Hib vaccination status requires attention to detail. Nurses should confirm the exact dates of each dose, the brand of the vaccine administered (e.g., ActHIB, Hiberix, or PedvaxHIB), and any adverse reactions reported post-vaccination. Documentation should align with state immunization records and the child’s personal health record. In cases where an infant has missed a dose, nurses must consult the CDC’s catch-up schedule, which simplifies the process of getting the child back on track. For example, if the 6-month dose is delayed, a single dose is sufficient for children aged 7-11 months, while older children may require additional doses.
A persuasive argument for Hib vaccine verification lies in its proven efficacy. Before the vaccine’s introduction in the 1990s, Hib was the leading cause of bacterial meningitis in children under 5, with approximately 20,000 cases annually in the U.S. Today, incidence rates have plummeted by over 99%, demonstrating the vaccine’s transformative impact on public health. Nurses must emphasize this success story to parents, addressing hesitancy with evidence-based reassurance. Highlighting the rarity of severe side effects—typically limited to mild fever or soreness at the injection site—can further build trust.
Comparatively, the Hib vaccine stands out for its integration into combination vaccines, such as Pentacel (DTaP-IPV-Hib) or MenHibrix (MenCY-TT + Hib), which streamline the immunization process by reducing the number of injections required. Nurses should be familiar with these options, as they offer practical advantages for both healthcare providers and families. However, it’s essential to note that combination vaccines may have specific age restrictions or dosing intervals, necessitating careful planning and documentation.
In practice, nurses can enhance Hib vaccine verification by incorporating it into routine well-child visits. A descriptive approach involves creating a visual checklist for parents, clearly outlining the vaccine schedule and marking completed doses. This not only aids in verification but also empowers parents to take an active role in their child’s health. Additionally, leveraging electronic health records (EHRs) with automated reminders can reduce the likelihood of missed doses. By combining clinical rigor with patient-centered communication, nurses ensure that no infant falls through the cracks in the fight against Hib-related diseases.
Convert Your US Vaccine Passport to EU Format: A Step-by-Step Guide
You may want to see also
Explore related products






![]()
Pneumococcal conjugate vaccine (PCV) status
Pneumococcal disease, caused by the bacterium *Streptococcus pneumoniae*, poses a significant threat to infants, who are particularly vulnerable due to their developing immune systems. This disease can lead to severe conditions such as pneumonia, meningitis, and bloodstream infections, making vaccination a critical preventive measure. The Pneumococcal Conjugate Vaccine (PCV) is designed to protect against these invasive infections, and verifying an infant’s PCV status is a non-negotiable task for nurses. The Centers for Disease Control and Prevention (CDC) recommends a specific schedule for PCV administration, typically starting at 2 months of age, with additional doses at 4 months, 6 months, and a booster dose between 12 and 15 months. Ensuring adherence to this schedule is vital, as incomplete vaccination leaves infants at risk.
Analyzing the PCV schedule reveals its strategic design to maximize immunity during the first year of life, when infants are most susceptible. The initial doses at 2, 4, and 6 months build a foundation of protection, while the booster dose reinforces long-term immunity. Nurses must verify not only the receipt of these doses but also their timing, as deviations from the recommended intervals can compromise efficacy. For example, if the 6-month dose is administered too early, the immune response may be suboptimal. Practical tips for nurses include cross-referencing vaccination records with the infant’s age and confirming the specific PCV formulation used (e.g., PCV13 or PCV15), as different versions offer varying levels of protection against pneumococcal serotypes.
Persuasively, the importance of PCV cannot be overstated, especially in populations with limited access to healthcare. Pneumococcal disease disproportionately affects underserved communities, where delayed or missed vaccinations can have devastating consequences. Nurses play a pivotal role in advocating for timely PCV administration and educating caregivers about its benefits. Addressing hesitancy or misinformation requires clear communication about the vaccine’s safety and efficacy, supported by data showing a dramatic reduction in pneumococcal infections since PCV’s introduction. Emphasizing that PCV is a lifesaving intervention can motivate caregivers to prioritize their infant’s vaccination schedule.
Comparatively, PCV stands out among infant vaccines due to its broad impact on reducing hospitalizations and mortality. Unlike some vaccines that target specific diseases, PCV addresses a bacterium responsible for multiple severe conditions, making its verification a high-priority task. Nurses should contrast PCV with other vaccines in their discussions with caregivers, highlighting its unique role in preventing invasive infections. For instance, while the DTaP vaccine protects against three diseases (diphtheria, tetanus, and pertussis), PCV safeguards against a wide range of pneumococcal serotypes, underscoring its comprehensive value. This comparative perspective can help caregivers appreciate the urgency of maintaining their infant’s PCV status.
Descriptively, the process of verifying PCV status involves meticulous attention to detail. Nurses should review the infant’s immunization record, noting the dates and dosages of each PCV administration. In cases where records are incomplete or unclear, contacting previous healthcare providers or referring to state immunization registries can provide clarity. Physical examination for signs of pneumococcal infection, such as fever or respiratory distress, should prompt immediate verification of PCV status. Additionally, nurses should be prepared to administer catch-up doses if an infant has fallen behind schedule, following CDC guidelines for appropriate intervals. This thorough approach ensures that no infant is left unprotected against this preventable yet potentially deadly disease.
Fetal Cells in MMR Vaccines: Abortion's Dark Legacy
You may want to see also
Explore related products





![]()
Rotavirus vaccine administration validation
Rotavirus vaccination is a critical component of an infant's immunization schedule, yet its administration requires meticulous validation to ensure efficacy and safety. The vaccine is typically given orally in a liquid form, with the first dose administered between 6 and 15 weeks of age, followed by additional doses at 4- to 10-week intervals, depending on the brand. For instance, the RotaTeq® vaccine is given in a 3-dose series at ages 2 months, 4 months, and 6 months, while Rotarix® is a 2-dose series at ages 2 months and 4 months. Nurses must verify that the infant has received the correct brand and dosage, as mixing brands is not recommended and may compromise immunity.
Validation of rotavirus vaccine administration involves more than just checking the dose schedule. Nurses should confirm the vaccine’s storage conditions, as improper refrigeration (between 2°C and 8°C) can render it ineffective. Additionally, the vaccine must be administered orally without contamination—it should not come into contact with pacifiers, bottles, or other objects that could introduce bacteria or viruses. Practical tips include administering the vaccine before feeding to reduce the risk of spitting up and ensuring the infant is healthy at the time of vaccination, as moderate to severe illnesses may warrant a delay.
A comparative analysis highlights the importance of rotavirus vaccination in preventing severe gastroenteritis, which can lead to dehydration and hospitalization. Before the vaccine’s introduction, rotavirus was responsible for approximately 200,000 emergency room visits and 55,000 to 70,000 hospitalizations annually in the U.S. alone. Post-vaccination, these numbers have dropped dramatically, underscoring the need for rigorous administration validation. Nurses play a pivotal role in educating parents about the vaccine’s benefits and addressing concerns, such as the rare but serious risk of intussusception, which occurs in about 1 in 20,000 to 1 in 100,000 infants.
Instructively, nurses should document each dose in the infant’s immunization record, noting the brand, date, and any adverse reactions. This documentation is essential for tracking compliance with the CDC’s recommended schedule and ensuring the infant receives all required doses. If a dose is missed or delayed, nurses must follow catch-up guidelines, such as administering the final dose by 8 months of age for RotaTeq® or by 24 weeks for Rotarix®. Clear communication with parents about the importance of timely vaccination and potential side effects, like mild fever or irritability, fosters trust and adherence.
Persuasively, the validation of rotavirus vaccine administration is not just a procedural step but a lifesaving measure. By ensuring proper dosing, storage, and administration, nurses directly contribute to reducing the global burden of rotavirus-related morbidity and mortality. This vaccine’s success hinges on meticulous attention to detail, making the nurse’s role indispensable in safeguarding infant health. Through vigilance and education, healthcare providers can maximize the vaccine’s impact, protecting vulnerable populations from a preventable yet potentially devastating disease.
Delayed Vaccination Impact: Effects of a 4-Week Gap Between Doses
You may want to see also
Frequently asked questions
At the 2-month check-up, the nurse should verify the infant has received the first doses of the following vaccines: DTaP (Diphtheria, Tetanus, and Pertussis), Hib (Haemophilus influenzae type b), IPV (Inactivated Polio Vaccine), PCV13 (Pneumococcal Conjugate Vaccine), and RV (Rotavirus Vaccine).
At the 4-month visit, the nurse should verify the infant has received the second doses of DTaP, Hib, IPV, PCV13, and RV vaccines, as these are part of the routine immunization schedule.
By the 6-month check-up, the nurse should confirm the infant has received the third dose of DTaP, Hib, and RV vaccines, as well as the second dose of PCV13 and the first dose of the influenza vaccine (if flu season is ongoing and the infant is 6 months or older).