Pediatric vaccinations are a cornerstone of public health, playing a critical role in preventing serious and potentially life-threatening diseases in children. Understanding the truths about these vaccines is essential for parents, caregivers, and healthcare providers to make informed decisions. Among the various claims and misconceptions surrounding pediatric vaccinations, it is crucial to identify which statements are scientifically accurate. This includes recognizing the proven efficacy of vaccines in preventing diseases, their safety profiles based on rigorous testing and monitoring, and the importance of adhering to recommended immunization schedules to ensure optimal protection for children. By focusing on evidence-based information, we can dispel myths and promote the widespread benefits of pediatric vaccinations.
| Characteristics | Values |
|---|---|
| Purpose | Prevent childhood diseases, reduce morbidity and mortality. |
| Recommended Age Range | Birth to 18 years (varies by vaccine and country guidelines). |
| Common Vaccines | DTaP, MMR, IPV, Hib, Hepatitis B, Varicella, PCV13, Rotavirus, Flu, etc. |
| Schedule | Follows a standardized schedule (e.g., CDC, WHO) with multiple doses. |
| Safety | Rigorously tested and monitored; side effects are rare and mild. |
| Effectiveness | High efficacy in preventing targeted diseases (e.g., 97% for measles). |
| Herd Immunity | Protects vulnerable populations (e.g., infants, immunocompromised). |
| Global Impact | Reduced global disease burden (e.g., polio eradication efforts). |
| Common Side Effects | Pain at injection site, fever, fussiness, mild rash. |
| Myths Debunked | No link to autism or other serious long-term health issues. |
| Mandatory in Some Regions | Required for school entry in many countries (with exemptions). |
| Cost-Effectiveness | Saves healthcare costs by preventing diseases and complications. |
| Parental Education | Critical for informed decision-making and adherence to schedules. |
| Recent Developments | COVID-19 vaccines approved for children aged 6 months and older. |
| Challenges | Vaccine hesitancy, access disparities, supply chain issues. |
Explore related products






What You'll Learn
- Vaccine Safety: Pediatric vaccines undergo rigorous testing to ensure safety and efficacy for children
- Immunization Schedule: Following the CDC’s recommended timeline maximizes protection against preventable diseases
- Herd Immunity: High vaccination rates protect vulnerable children who cannot receive vaccines
- Common Myths: Debunking misconceptions about vaccines, such as autism links, is crucial
- Disease Prevention: Vaccines effectively prevent serious illnesses like measles, mumps, and whooping cough
![]()
Vaccine Safety: Pediatric vaccines undergo rigorous testing to ensure safety and efficacy for children
Pediatric vaccines are among the most thoroughly tested medical products available, undergoing a multi-stage evaluation process to ensure they meet stringent safety and efficacy standards. Before a vaccine is approved for use in children, it must pass through preclinical testing, three phases of clinical trials, and rigorous reviews by regulatory bodies such as the FDA and CDC. For instance, the measles, mumps, and rubella (MMR) vaccine was studied in over 1,000 children during its clinical trials, with ongoing monitoring post-approval to detect any rare side effects. This meticulous process ensures that vaccines like MMR, which is administered in two doses starting at 12 months of age, are both safe and effective for pediatric populations.
One critical aspect of vaccine safety is the careful calibration of dosages for children, who differ physiologically from adults. Pediatric vaccines are specifically formulated to account for age, weight, and developmental stage. For example, the influenza vaccine for children aged 6 months to 8 years often requires two doses in the first year of vaccination to build robust immunity. Similarly, the hepatitis B vaccine is administered in a three-dose series starting at birth, with smaller volumes used for infants compared to older children. These tailored approaches minimize risks while maximizing protection, demonstrating the precision involved in pediatric vaccine development.
Parents often wonder about the side effects of vaccines, but it’s important to distinguish between normal, mild reactions and rare, serious concerns. Common side effects, such as soreness at the injection site or low-grade fever, are signs the immune system is responding as expected. For example, after the DTaP vaccine (which protects against diphtheria, tetanus, and pertussis), about 1 in 4 children may experience redness or swelling where the shot was given. Serious adverse events, such as severe allergic reactions, are exceedingly rare, occurring in fewer than 1 in a million doses. Post-licensure surveillance systems like VAERS (Vaccine Adverse Event Reporting System) continuously monitor for such events, ensuring swift action if any safety concerns arise.
Comparing pediatric vaccines to other medical interventions highlights their exceptional safety profile. For instance, the risk of a severe allergic reaction to a vaccine is far lower than the risk of anaphylaxis from a peanut allergy or even from taking a common antibiotic like amoxicillin. Moreover, the diseases vaccines prevent—such as polio, which can cause paralysis, or measles, which can lead to pneumonia and encephalitis—pose far greater risks than the vaccines themselves. This risk-benefit analysis underscores why pediatric vaccines are a cornerstone of public health, protecting not only individual children but also vulnerable populations through herd immunity.
Practical tips for parents can further enhance the vaccine experience for children. Scheduling vaccinations during calm times of the day, using distraction techniques like singing or toys, and administering acetaminophen (as recommended by a pediatrician) can help manage discomfort. Keeping a record of vaccination dates and any reactions is also useful for future reference. By understanding the rigorous testing behind pediatric vaccines and taking proactive steps, parents can confidently protect their children’s health while contributing to broader community immunity.
Spouse Vaccination: Essential Workers' Eligibility
You may want to see also
Explore related products






![]()
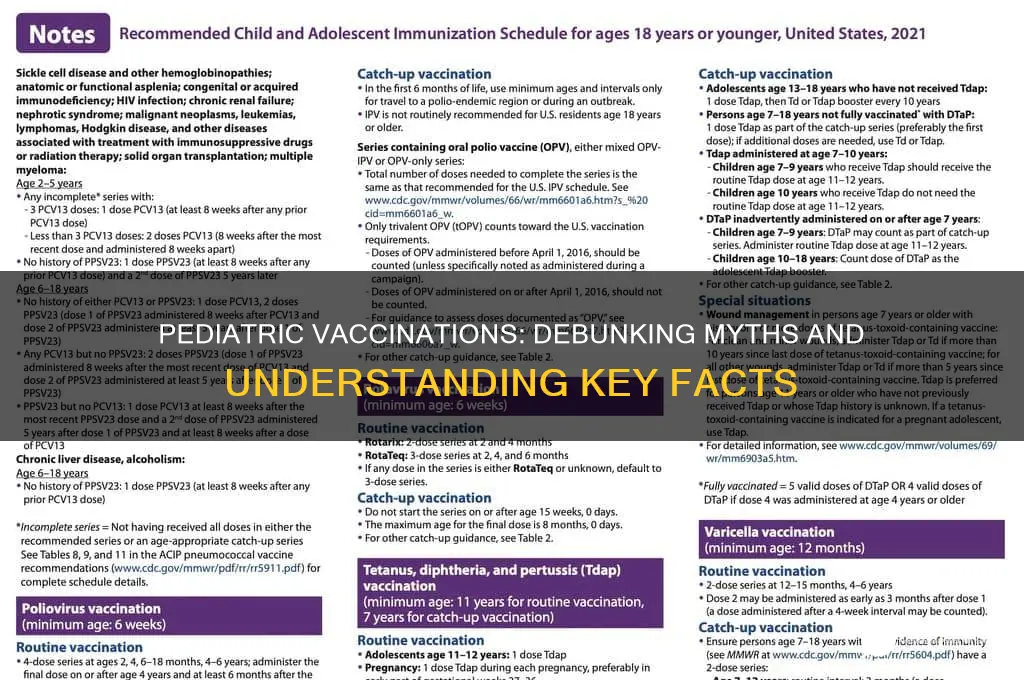
Immunization Schedule: Following the CDC’s recommended timeline maximizes protection against preventable diseases
Adhering to the CDC’s immunization schedule is not merely a bureaucratic checklist; it’s a scientifically calibrated roadmap designed to protect children when they are most vulnerable. For instance, the first dose of the measles, mumps, and rubella (MMR) vaccine is administered at 12–15 months, followed by a booster at 4–6 years. This timing aligns with the waning of maternal antibodies, ensuring the child’s immune system is primed to respond effectively. Deviating from this schedule can leave gaps in immunity, as seen in outbreaks where undervaccinated communities experience higher disease rates. The CDC’s timeline is not arbitrary—it’s the result of decades of research optimizing when a child’s immune system can best handle and respond to vaccines.
Consider the hepatitis B vaccine, which begins at birth with the first dose, followed by doses at 1–2 months and 6–18 months. This sequence is critical because infants exposed to the virus at birth face a 90% risk of chronic infection if unvaccinated. By following the CDC’s schedule, parents ensure their child is shielded during the earliest and most dangerous window of exposure. Similarly, the DTaP vaccine (diphtheria, tetanus, pertussis) is given in a series starting at 2 months, with boosters at 4, 6, and 15–18 months, followed by a final dose at 4–6 years. This staggered approach builds robust immunity layer by layer, minimizing the risk of breakthrough infections.
A common misconception is that delaying vaccines or spacing them out is safer. However, this practice contradicts immunological principles and increases the period a child remains susceptible to diseases. For example, delaying the varicella (chickenpox) vaccine from its recommended age of 12–15 months could result in a child contracting the disease during peak circulation seasons, leading to severe complications like bacterial skin infections or pneumonia. The CDC’s schedule is designed to balance the urgency of protection with the safety and efficacy of each vaccine, ensuring children are shielded during critical developmental stages.
Practical adherence to the schedule requires proactive planning. Parents should mark key milestones—such as the 6-month mark for the first influenza vaccine or the 11–12-year visit for the HPV vaccine series—and communicate openly with healthcare providers. Missed doses can often be caught up using the CDC’s catch-up schedule, which adjusts intervals to restore immunity without starting over. For families with multiple children, syncing vaccine visits with well-child checkups can streamline the process. Ultimately, the CDC’s timeline is a tool, not a trap—it empowers parents to provide their children with the fullest possible defense against preventable diseases.
Vaccine Timing: How Long Between Doses?
You may want to see also
Explore related products






![]()
Herd Immunity: High vaccination rates protect vulnerable children who cannot receive vaccines
Vaccination rates above 90% create a protective shield around communities, a concept known as herd immunity. This phenomenon is particularly crucial for vulnerable children who cannot receive vaccines due to medical conditions like severe allergies, compromised immune systems, or certain genetic disorders. When a high percentage of the population is immunized, the spread of infectious diseases is significantly reduced, minimizing the risk of exposure for these unprotected individuals. For instance, measles, a highly contagious virus, requires a vaccination rate of approximately 95% to achieve herd immunity. Falling below this threshold can lead to outbreaks that endanger those who cannot be vaccinated.
Consider the case of a child undergoing chemotherapy for leukemia. Their immune system, weakened by treatment, cannot handle live vaccines like the MMR (measles, mumps, rubella) shot. Herd immunity becomes their only defense against these diseases. Without it, a single exposure could have severe, even life-threatening, consequences. This example underscores the collective responsibility of communities to maintain high vaccination rates, not just for individual protection but for the safety of the most vulnerable among us.
Achieving herd immunity requires strategic planning and widespread participation. Vaccination schedules, such as the CDC’s recommended timeline for pediatric immunizations, are designed to build immunity early in life. For example, the first dose of the MMR vaccine is typically administered between 12 and 15 months of age, with a second dose between 4 and 6 years. Adhering to these schedules ensures that children are protected during their most susceptible years and contributes to the broader goal of herd immunity. Parents and caregivers play a pivotal role by staying informed, following medical advice, and prioritizing timely vaccinations.
Critics of herd immunity often argue that it absolves individuals of personal responsibility, but this perspective overlooks its communal benefits. While some may question the necessity of vaccinating their healthy child, the reality is that no one knows when or where they might encounter a vulnerable individual. A child with a rare immune disorder could be in the same classroom, playground, or grocery store. By vaccinating, individuals not only protect their own children but also act as a barrier to prevent diseases from reaching those who cannot be immunized. This shared responsibility is the cornerstone of public health.
In practical terms, maintaining herd immunity involves more than just getting vaccinated. It requires staying updated on booster shots, especially for diseases like pertussis (whooping cough), where immunity wanes over time. Adults, including pregnant women, should receive the Tdap vaccine to protect newborns who are too young to be vaccinated. Schools and daycare centers can enforce vaccination policies while providing exemptions only for valid medical reasons. Public health campaigns can educate communities about the importance of herd immunity, dispelling myths and fostering trust in science. Together, these efforts create a safer environment for all children, especially those who rely on the immunity of others for their survival.
Live vs. Inactive Vaccines: Understanding Active and Inactive Virus Components
You may want to see also
Explore related products






![]()
Common Myths: Debunking misconceptions about vaccines, such as autism links, is crucial
One of the most persistent myths about pediatric vaccinations is the alleged link between vaccines and autism. This misconception, fueled by a now-debunked 1998 study, has led to widespread fear and hesitancy among parents. The original study, which claimed a connection between the MMR (measles, mumps, rubella) vaccine and autism, was retracted by the journal that published it and has been discredited by numerous large-scale studies. For instance, a 2019 study involving over 650,000 children found no evidence of an increased risk of autism in vaccinated children. Despite this, the myth persists, highlighting the need for clear, evidence-based communication to correct misinformation.
To address this myth, it’s essential to understand the science behind vaccine safety. Vaccines undergo rigorous testing and monitoring before approval, with ongoing surveillance through systems like the Vaccine Adverse Event Reporting System (VAERS) in the U.S. Pediatric vaccines are administered in specific dosages tailored to age groups—for example, the MMR vaccine is typically given in two doses, the first at 12–15 months and the second at 4–6 years. These schedules are designed to maximize protection while minimizing risks. Parents should consult healthcare providers to ensure their child’s vaccinations are up to date, as delays can leave children vulnerable to preventable diseases.
A comparative analysis of vaccinated and unvaccinated populations further debunks the autism myth. Countries with high vaccination rates, such as Denmark and Finland, have not seen a corresponding rise in autism diagnoses. Conversely, outbreaks of vaccine-preventable diseases like measles have occurred in communities with low vaccination rates, underscoring the importance of herd immunity. For example, the 2019 measles outbreak in the U.S. primarily affected unvaccinated individuals, leading to over 1,200 cases—the highest number in decades. This data reinforces that vaccines protect against diseases, not cause developmental disorders.
Practical steps can help parents navigate vaccine-related concerns. First, rely on credible sources such as the Centers for Disease Control and Prevention (CDC), World Health Organization (WHO), or pediatricians for information. Second, ask specific questions about vaccine ingredients, side effects, and benefits during doctor visits. For instance, the preservative thimerosal, once falsely linked to autism, has been removed from all routine childhood vaccines except some flu shots, which contain trace amounts deemed safe by the FDA. Finally, consider the real risks of forgoing vaccines—diseases like pertussis (whooping cough) can be life-threatening for infants, while mumps can lead to complications like deafness.
In conclusion, debunking the autism myth is not just about correcting misinformation but about restoring trust in one of modern medicine’s greatest achievements. Vaccines save millions of lives annually, and their safety is supported by decades of research. By focusing on facts, parents can make informed decisions that protect their children and communities. The takeaway is clear: vaccines are a vital tool in pediatric health, and their benefits far outweigh any unfounded fears.
Hong Kong's Child Vaccination Rates: Current Statistics and Trends
You may want to see also
Explore related products






![]()
Disease Prevention: Vaccines effectively prevent serious illnesses like measles, mumps, and whooping cough
Vaccines are one of the most powerful tools in modern medicine, acting as a shield against diseases that once ravaged childhoods. Measles, mumps, and whooping cough (pertussis) are prime examples of illnesses that vaccines have transformed from common threats to rare occurrences in many parts of the world. Before the measles vaccine was introduced in 1963, for instance, the disease caused an estimated 2.6 million deaths annually worldwide. Today, thanks to widespread vaccination, global deaths have plummeted by 73% from 2000 to 2018. This dramatic reduction underscores the effectiveness of vaccines in preventing not just infection, but also the severe complications these diseases can cause, such as pneumonia, encephalitis, and lifelong disabilities.
Consider the pertussis vaccine, typically administered as part of the DTaP series (diphtheria, tetanus, and acellular pertussis) starting at 2 months of age, with booster doses given at 4 months, 6 months, 15-18 months, and 4-6 years. This vaccine not only protects the vaccinated child but also helps create herd immunity, reducing the spread of the disease to vulnerable populations, such as infants too young to be vaccinated or individuals with compromised immune systems. For example, a 2016 study in *Pediatrics* found that vaccinated siblings were 95% less likely to transmit pertussis to young infants, highlighting the dual benefit of individual and community protection.
While vaccines are highly effective, their success depends on timely administration and adherence to recommended schedules. The MMR vaccine (measles, mumps, and rubella), for instance, is given in two doses: the first at 12-15 months and the second at 4-6 years. This two-dose regimen provides 97% protection against measles, a disease so contagious that 9 out of 10 unvaccinated people exposed to it will become infected. Parents should also be aware of potential mild side effects, such as soreness at the injection site or low-grade fever, which are far outweighed by the risks of the diseases themselves. For example, measles can lead to pneumonia in 1 out of every 20 children, while mumps can cause deafness or meningitis in rare cases.
Critics often raise concerns about vaccine safety, but decades of research and billions of doses administered worldwide have consistently demonstrated their safety and efficacy. The WHO and CDC rigorously monitor vaccine safety through systems like the Vaccine Adverse Event Reporting System (VAERS) and the Vaccine Safety Datalink (VSD). For instance, a 2014 meta-analysis in *Vaccine* reviewed over 20,000 studies and found no link between the MMR vaccine and autism, debunking a long-standing myth. Such evidence reinforces the importance of relying on credible sources when making vaccination decisions.
In practical terms, parents can take proactive steps to ensure their children’s vaccinations are up to date. Keep a record of all vaccine doses, including dates and types, and use tools like the CDC’s Catch-Up Immunization Scheduler if doses are missed. Schools and daycare centers often require proof of vaccination, so staying organized can prevent last-minute hassles. Additionally, staying informed about local outbreaks—such as the 2019 measles outbreak in the U.S., which saw over 1,200 cases—can serve as a reminder of the ongoing need for vigilance. Vaccines are not just a personal health decision; they are a collective responsibility to protect the most vulnerable among us.
Super Bowl: Vaccinated or Not?
You may want to see also
Frequently asked questions
Yes, pediatric vaccinations are rigorously tested and proven safe for children. They are monitored by health organizations to ensure ongoing safety and efficacy.
No, extensive research has shown no link between pediatric vaccinations and autism. This myth has been debunked by numerous scientific studies.
No, pediatric vaccinations actually strengthen the immune system by preparing it to fight specific diseases without causing the illness itself.
Vaccination requirements vary by country and region, but many are recommended or required for school entry to protect public health.
Yes, mild illnesses like a cold usually do not prevent a child from receiving vaccinations. However, consult a healthcare provider for specific advice.