The TB vaccine, also known as the Bacillus Calmette-Guérin (BCG) vaccine, is a widely used immunization tool designed to protect against tuberculosis, a serious infectious disease caused by the bacterium Mycobacterium tuberculosis. Developed in the early 20th century, the BCG vaccine is primarily administered to infants and young children in countries with high TB prevalence to reduce the risk of severe forms of the disease, such as tuberculous meningitis. However, its effectiveness in preventing pulmonary TB in adults varies, leading to ongoing debates about its optimal use. When discussing which of the following is the TB vaccine, the answer is unequivocally the BCG vaccine, as it remains the only licensed vaccine specifically developed for tuberculosis prevention.
| Characteristics | Values |
|---|---|
| Vaccine Name | Bacille Calmette-Guerin (BCG) |
| Type | Live attenuated vaccine |
| Disease Prevention | Tuberculosis (TB) |
| Developer | Albert Calmette and Camille Guérin |
| Year of Development | 1921 |
| Administration Route | Intradermal injection |
| Target Population | Newborns, infants, and children in high-risk areas |
| Efficacy | Variable (50-80% against severe forms of TB in children) |
| Duration of Protection | 10-15 years (variable) |
| Dosage | Single dose (0.05 mL or 0.1 mL depending on region) |
| Age at Administration | Typically within the first few days of life |
| Side Effects | Local reaction (ulceration, scarring), rare systemic reactions |
| Contraindications | Severe immunosuppression (e.g., HIV/AIDS), pregnancy (if not previously vaccinated) |
| Global Usage | Widely used in TB-endemic countries, not routinely used in low-incidence countries like the U.S. |
| WHO Recommendation | Recommended for all infants in high-burden countries |
| Storage | Requires refrigeration (2-8°C) |
| Additional Uses | Investigated for potential use against other diseases (e.g., bladder cancer, leprosy) |
Explore related products






What You'll Learn
- BCG Vaccine Composition: Contains live attenuated Mycobacterium bovis, effective against severe TB forms in kids
- BCG Vaccine Efficacy: Varies widely, 0-80% protection against pulmonary TB in adults
- BCG Vaccine Administration: Typically given intradermally at birth in high-burden countries
- BCG Vaccine Side Effects: Common reactions include local ulceration, scarring, and rare disseminated infections
- BCG Vaccine Alternatives: Research ongoing for newer vaccines like M72/AS01E and VPM1002
![]()
BCG Vaccine Composition: Contains live attenuated Mycobacterium bovis, effective against severe TB forms in kids
The BCG vaccine stands as a cornerstone in the fight against tuberculosis, particularly in protecting children from its most severe forms. Its composition is both simple and ingenious: a single, live attenuated strain of *Mycobacterium bovis*, a bacterium closely related to *Mycobacterium tuberculosis*, the causative agent of TB. This attenuated form is weakened to the point where it cannot cause disease in healthy individuals but retains enough potency to stimulate a robust immune response. This unique feature makes BCG a prime example of how vaccines can harness the body’s natural defenses to prevent life-threatening infections.
Administered typically within the first few days of life, the BCG vaccine is delivered via an intradermal injection, usually on the left upper arm. The dosage is standardized at 0.05 mL for newborns, ensuring a precise and effective immune activation. While the vaccine’s primary role is to shield against disseminated TB forms like miliary TB and tuberculous meningitis, its efficacy against pulmonary TB in adults is less consistent, varying widely by region and population. This variability underscores the importance of understanding BCG’s strengths and limitations in global TB control strategies.
One of the most striking aspects of the BCG vaccine is its dual nature: a lifesaver for children in high-burden settings, yet a subject of debate in low-incidence regions. In countries where TB is endemic, BCG vaccination is non-negotiable, offering up to 80% protection against severe TB in pediatric populations. However, in areas with low TB prevalence, the risk-benefit analysis shifts, as the vaccine’s side effects, though rare, include local abscesses, lymphadenitis, and, in extremely rare cases, disseminated BCG infection in immunocompromised individuals. This highlights the need for tailored vaccination policies that consider local epidemiology and individual health status.
Practical considerations for BCG vaccination include ensuring the vaccine is administered by trained healthcare personnel, as improper technique can lead to inadequate immune response or adverse reactions. Parents should be informed about the characteristic scar that forms at the injection site, a hallmark of successful vaccination. Additionally, BCG is contraindicated in HIV-positive infants due to the risk of disseminated disease, emphasizing the importance of pre-vaccination screening in high-HIV prevalence areas. Despite its limitations, the BCG vaccine remains a vital tool in the global effort to curb TB, particularly in safeguarding the most vulnerable—children—from its deadliest forms.
Vaccines vs. Viruses: How Immunization Prevents Deadly Mutations
You may want to see also
Explore related products






![]()
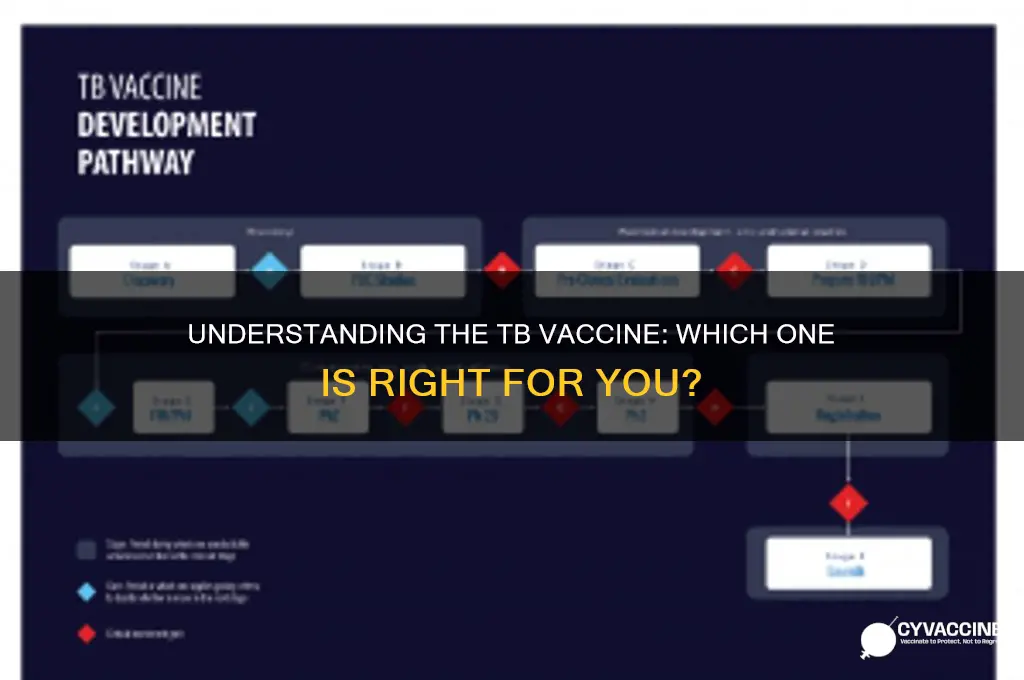
BCG Vaccine Efficacy: Varies widely, 0-80% protection against pulmonary TB in adults
The BCG vaccine, a cornerstone of tuberculosis (TB) prevention, presents a paradox: its efficacy against pulmonary TB in adults ranges dramatically from 0% to 80%. This wide variability raises critical questions about its reliability as a protective measure. Developed in the 1920s, Bacille Calmette-Guérin (BCG) is one of the most widely administered vaccines globally, yet its performance remains inconsistent. Factors such as geographic location, genetic differences, and prior exposure to environmental mycobacteria influence its effectiveness, making it a complex tool in the fight against TB.
To understand this variability, consider the vaccine’s mechanism. BCG is a live attenuated vaccine derived from *Mycobacterium bovis*, designed to stimulate an immune response against *Mycobacterium tuberculosis*. However, its protection wanes over time, and it is most effective in preventing severe forms of TB in children, such as miliary or meningeal TB. For adults, particularly those at high risk of pulmonary TB, the vaccine’s efficacy is less predictable. Studies show that while BCG can reduce the risk of pulmonary TB in some populations by up to 80%, it offers no protection in others. This inconsistency underscores the need for tailored vaccination strategies based on regional TB prevalence and individual risk factors.
Practical considerations further complicate BCG’s use. The vaccine is typically administered as a single intradermal dose of 0.05–0.1 mL in newborns, with a scar forming at the injection site as a sign of successful immunization. However, revaccination in adulthood is not recommended due to limited evidence of increased efficacy and potential adverse reactions. For adults in high-risk settings, alternative strategies such as latent TB infection screening and preventive therapy with antibiotics like isoniazid may be more effective. This highlights the importance of integrating BCG into a broader TB control framework rather than relying on it as a standalone solution.
Comparatively, the variability in BCG efficacy contrasts sharply with vaccines for other diseases, such as measles or polio, which consistently provide high levels of protection. This discrepancy has spurred research into next-generation TB vaccines, such as M72/AS01E, which has shown promising results in clinical trials. Until such vaccines become widely available, however, BCG remains a vital, if imperfect, tool. Its role is particularly crucial in regions with high TB incidence, where even partial protection can significantly reduce disease burden.
In conclusion, the BCG vaccine’s efficacy against pulmonary TB in adults is a double-edged sword—offering substantial protection in some cases but none in others. Its use requires a nuanced approach, considering local epidemiology, individual risk, and complementary preventive measures. While it is not a panacea, BCG’s ability to prevent severe TB in children and reduce adult cases in certain populations ensures its continued relevance in global TB control efforts. Understanding its limitations and strengths is key to maximizing its impact.
MMR Vaccine: Should Adults Over 60 Consider Getting It?
You may want to see also
Explore related products






![]()
BCG Vaccine Administration: Typically given intradermally at birth in high-burden countries
The BCG vaccine, a cornerstone in the fight against tuberculosis (TB), is administered intradermally, a method that sets it apart from many other vaccines. This route involves injecting a small dose of the vaccine just beneath the skin's surface, typically in the left upper arm. The technique is precise, requiring a skilled healthcare provider to ensure the vaccine is delivered correctly. In high-burden countries, where TB is endemic, this vaccine is a critical intervention, often given at birth to provide early protection against severe forms of TB, such as meningitis and miliary TB in infants.
Administering the BCG vaccine intradermally is not arbitrary; it is a strategic choice to maximize immune response while minimizing side effects. The standard dose is 0.05 mL, containing 2-8 × 10^5 colony-forming units of the attenuated *Mycobacterium bovis* strain. This method ensures the vaccine remains localized, allowing the immune system to recognize and respond effectively. For newborns, the timing is crucial—the vaccine is ideally given within the first few days of life, as delays can reduce its efficacy. In some settings, birthweight or gestational age may influence the decision to vaccinate immediately, with healthcare providers often waiting until the infant is stable if born prematurely or underweight.
While the BCG vaccine is highly effective in preventing severe TB in children, its protection against pulmonary TB in adults is variable. This limitation has sparked debates about its universal administration, particularly in low-burden countries. However, in high-burden settings, the benefits far outweigh the risks. The vaccine’s ability to prevent life-threatening TB in young children makes it an indispensable tool in public health. Parents and caregivers should be informed about potential side effects, such as a small ulcer at the injection site that may leave a scar, and rare complications like lymphadenitis or disseminated BCG infection, particularly in immunocompromised individuals.
Practical considerations for BCG administration include ensuring a sterile environment and using a fine, short needle (25-27 gauge) to achieve the correct intradermal placement. Healthcare workers must be trained to recognize and manage adverse reactions, though these are uncommon. In resource-limited settings, maintaining the vaccine’s cold chain is critical, as exposure to heat can render it ineffective. Despite these challenges, the BCG vaccine remains a cost-effective and vital intervention in high-burden countries, where it continues to save countless lives by preventing severe TB in the most vulnerable populations.
Vaccine Choice: Can I Mix and Match?
You may want to see also
Explore related products






![]()
BCG Vaccine Side Effects: Common reactions include local ulceration, scarring, and rare disseminated infections
The BCG vaccine, primarily used to protect against severe forms of tuberculosis (TB), is administered to infants and high-risk individuals in TB-endemic regions. While it is a critical tool in TB prevention, its side effects, though generally mild, warrant attention. Among the most common reactions are local ulceration and scarring at the injection site, typically the upper arm. These effects are not merely cosmetic; they serve as visible markers of the immune response triggered by the vaccine. Understanding these reactions is essential for caregivers and recipients to manage expectations and ensure proper aftercare.
Local ulceration, for instance, often appears 2–3 weeks post-vaccination and may persist for several weeks, eventually forming a scar. This process is normal and indicates the vaccine’s activation of the immune system. To minimize discomfort, keep the area clean and dry, avoiding tight clothing or excessive friction. Scarring, while permanent, is usually small and fades over time. It’s important to note that these reactions are more pronounced in individuals with weakened immune systems, such as those with HIV, where the vaccine’s live attenuated bacteria may cause prolonged or severe ulceration.
Rare but serious side effects include disseminated BCG infections, which occur when the vaccine bacteria spread beyond the injection site. This complication is more likely in immunocompromised individuals, particularly those with undiagnosed conditions like severe combined immunodeficiency (SCID). Symptoms may include persistent fever, swollen lymph nodes, or unusual fatigue. Immediate medical attention is crucial if these signs appear, as early intervention can prevent severe outcomes. For this reason, the BCG vaccine is contraindicated in individuals with known immune deficiencies.
Comparatively, the BCG vaccine’s side effects are far less severe than the risks associated with untreated TB, which can lead to life-threatening conditions like meningitis or miliary TB in children. While local reactions are common, they are a small price for the protection offered, particularly in high-burden settings. In low-incidence regions, however, the vaccine is often reserved for specific groups, such as healthcare workers or those with recent TB exposure, due to the rarity of severe TB forms and the potential for side effects.
In summary, while the BCG vaccine’s side effects—local ulceration, scarring, and rare disseminated infections—may seem concerning, they are typically manageable and outweighed by its benefits. Caregivers should monitor the injection site, maintain hygiene, and seek medical advice for unusual symptoms. For immunocompromised individuals, alternative preventive measures, such as TB screening and environmental controls, may be more appropriate. Understanding these nuances ensures the vaccine’s safe and effective use in the global fight against TB.
Broken Vaccine Vial: Emotions, Safety, and Handling the Unexpected
You may want to see also
Explore related products






![]()
BCG Vaccine Alternatives: Research ongoing for newer vaccines like M72/AS01E and VPM1002
The Bacille Calmette-Guérin (BCG) vaccine has been the cornerstone of tuberculosis (TB) prevention for over a century, yet its variable efficacy in adults underscores the urgent need for alternatives. Emerging candidates like M72/AS01E and VPM1002 represent a new frontier in TB vaccine development, each targeting different mechanisms to bolster immunity. M72/AS01E, a subunit vaccine, combines two *Mycobacterium tuberculosis* antigens with the AS01E adjuvant, while VPM1002 is a genetically modified BCG variant designed to enhance immunogenicity. These innovations aim to address BCG’s limitations, particularly in preventing pulmonary TB in adolescents and adults, where the disease is most transmissible.
Consider the clinical trial data for M72/AS01E, which demonstrated 50% efficacy in preventing TB disease in latently infected adults over three years. Administered as a two-dose regimen, 0.5 mL intramuscularly with an 8-week interval, it offers a promising tool for high-risk populations. However, its reliance on prior BCG vaccination and limited data in children highlight areas for further research. Practical implementation would require integrating it into existing TB control programs, potentially as a booster for BCG-vaccinated individuals.
In contrast, VPM1002 leverages genetic engineering to improve upon BCG’s shortcomings. By overexpressing the listeriolysin protein, it enhances antigen presentation and immune response. Early-phase trials show superior safety and immunogenicity compared to BCG, particularly in newborns, where it could replace BCG as a primary vaccine. A single 0.05 mL intradermal dose in neonates mirrors BCG’s administration route, ensuring ease of adoption in low-resource settings. Its ability to induce both cellular and humoral immunity positions it as a dual-purpose vaccine for TB prevention and immunotherapy.
While these alternatives show promise, challenges remain. Scaling up production, ensuring affordability, and conducting large-scale efficacy trials are critical steps. For instance, M72/AS01E’s complex formulation may increase costs, whereas VPM1002’s genetic modification requires stringent regulatory approval. Public health strategies must also address vaccine hesitancy and ensure equitable access, particularly in TB-endemic regions.
In summary, M72/AS01E and VPM1002 exemplify the evolving landscape of TB vaccines, offering tailored solutions to BCG’s limitations. Their development underscores the importance of innovation in global health, but success hinges on addressing practical and logistical hurdles. As research progresses, these vaccines could revolutionize TB prevention, moving us closer to the WHO’s goal of ending TB by 2030.
Understanding Haemophilus Influenzae Type B: Vaccine Type and Importance
You may want to see also
Frequently asked questions
The TB vaccine is known as the Bacille Calmette-Guérin (BCG) vaccine.
Yes, the BCG vaccine is currently the only licensed vaccine for tuberculosis (TB), though research is ongoing to develop more effective alternatives.
The BCG vaccine is primarily recommended for infants and children in countries with high TB prevalence. It is usually administered shortly after birth to provide early protection against severe forms of TB.