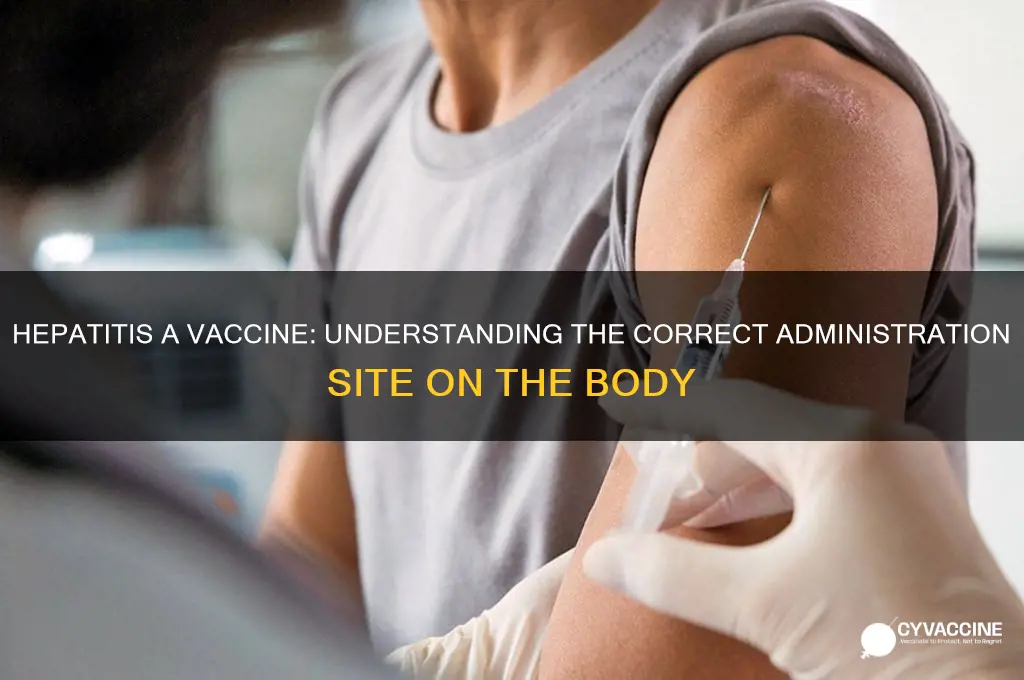
The hepatitis A vaccine is typically administered as an intramuscular injection, meaning it is delivered directly into the muscle tissue. The preferred site for this vaccination is the deltoid muscle, located in the upper arm, specifically the outer aspect of the arm, roughly two to three finger-widths below the acromion process (the bony tip of the shoulder). This location is chosen for its accessibility and the muscle's ability to effectively absorb the vaccine, ensuring optimal immune response. Proper administration technique is crucial to minimize discomfort and potential side effects, making the deltoid muscle the standard and recommended site for hepatitis A vaccine injection.
| Characteristics | Values |
|---|---|
| Administration Site | Deltoid muscle (upper arm) for adults and older children |
| Alternative Site | Anterolateral thigh muscle for infants and young children (aged 1-16) |
| Injection Route | Intramuscular (IM) injection |
| Needle Length | 1-inch (25 mm) for adults; 5/8-inch (16 mm) for children |
| Injection Angle | 90-degree angle for IM administration |
| Dose Volume | 0.5 mL for adults and children |
| Pain Management | Apply a cold compress or numbing cream if needed |
| Post-Injection Care | Avoid massaging the injection site; monitor for adverse reactions |
| Vaccine Schedule | Two doses, 6-18 months apart, depending on the vaccine brand |
| Common Side Effects | Soreness, redness, or swelling at the injection site |
| Contraindications | Severe allergic reaction to a previous dose or vaccine components |
| Special Populations | Safe for pregnant women and immunocompromised individuals (consult a healthcare provider) |
Explore related products


$13.98 $15.99

$13.98 $15.99



What You'll Learn
- Injection Site: Hepatitis A vaccine is typically administered in the deltoid muscle of the upper arm
- Alternative Locations: For infants or those with arm issues, the anterolateral thigh may be used
- Intramuscular Delivery: The vaccine is given intramuscularly to ensure proper absorption and immune response
- Avoiding Subcutaneous: Incorrect subcutaneous administration can reduce the vaccine's effectiveness and protection
- Post-Injection Care: Mild soreness at the injection site is normal; apply a cold compress if needed
![]()
Injection Site: Hepatitis A vaccine is typically administered in the deltoid muscle of the upper arm
The Hepatitis A vaccine is most commonly administered in the deltoid muscle of the upper arm, a site chosen for its accessibility and the muscle’s ability to efficiently absorb and process the vaccine. This injection site is standard for adults and children aged 11 and older, ensuring optimal immune response. The deltoid muscle is a large, sturdy muscle that allows for easy injection and minimizes discomfort compared to other potential sites. For this reason, healthcare providers are trained to target this area, making it the go-to location for intramuscular vaccines like Hepatitis A.
Administering the Hepatitis A vaccine in the deltoid muscle involves specific steps to ensure safety and efficacy. The typical dosage for adults and children aged 1 and older is 0.5 mL, injected deeply into the muscle. The injection site should be cleaned with an alcohol swab before administration to reduce the risk of infection. After injection, gentle pressure may be applied if there is minor bleeding, but rubbing the area should be avoided to prevent discomfort. Proper technique is crucial, as incorrect placement can lead to reduced vaccine effectiveness or unnecessary pain.
While the deltoid muscle is the preferred site, it’s important to note that alternative locations may be considered in specific circumstances. For example, individuals with limited upper arm mobility or those with significant deltoid muscle atrophy might receive the vaccine in the vastus lateralis muscle of the thigh. However, this is less common and typically reserved for cases where the deltoid is not a viable option. For the majority of recipients, the upper arm remains the most practical and effective choice, aligning with global vaccination guidelines.
Practical tips can enhance the experience of receiving the Hepatitis A vaccine in the deltoid muscle. Wearing loose-fitting clothing that allows easy access to the upper arm can simplify the process. After vaccination, keeping the arm active through gentle movement can help reduce soreness, though strenuous activity should be avoided for a few days. Applying a cold compress to the injection site can also alleviate discomfort. If pain persists or worsens, over-the-counter pain relievers like acetaminophen or ibuprofen may be used, but aspirin should be avoided in children and teenagers due to the risk of Reye’s syndrome.
In summary, the deltoid muscle of the upper arm is the primary injection site for the Hepatitis A vaccine, offering a balance of convenience and effectiveness. Adhering to proper administration techniques and following post-vaccination care tips can ensure a smooth experience. While exceptions exist, this site remains the standard for most individuals, underscoring its importance in global vaccination practices. Understanding these specifics empowers both recipients and providers to approach the process with confidence and clarity.
Supreme Court Rulings on Vaccines: Legal Insights and Implications
You may want to see also
Explore related products






![]()
Alternative Locations: For infants or those with arm issues, the anterolateral thigh may be used
The anterolateral thigh emerges as a viable alternative site for administering the hepatitis A vaccine, particularly for infants and individuals with arm-related challenges. This location, situated on the front outer side of the thigh, offers a practical solution when traditional arm administration is not feasible. For infants, whose arm muscles are still developing, the anterolateral thigh provides a larger, more accessible area for injection. Similarly, individuals with arm injuries, limited mobility, or conditions like lymphedema can benefit from this alternative site, ensuring they receive essential vaccinations without discomfort or complications.
When using the anterolateral thigh, healthcare providers must adhere to specific guidelines to ensure safety and efficacy. The injection should be administered into the muscle (intramuscularly) for optimal absorption, typically using a needle length of 5/8 to 1 inch for infants and 1 to 1.5 inches for older children or adults. The site is located in the middle of the thigh, roughly 2-3 finger widths below the top of the hip bone, avoiding areas with visible blood vessels or excessive fat. Proper positioning of the patient—lying down or seated with the leg relaxed—can help minimize pain and ensure accurate placement.
One of the key advantages of the anterolateral thigh site is its reduced risk of local adverse reactions compared to the arm, especially in populations with sensitive skin or prior injection-related issues. For infants, this site is less likely to interfere with their natural movements, allowing them to remain comfortable post-vaccination. Additionally, for individuals with arm issues, this alternative eliminates the need to navigate around injuries or prosthetics, streamlining the vaccination process. However, it’s crucial to monitor the site for redness, swelling, or tenderness, as these reactions, though rare, can still occur.
Practical considerations for caregivers and healthcare providers include ensuring the thigh area is clean and dry before administration. For infants, distracting them with gentle rocking or feeding during the injection can help ease the experience. In older individuals, explaining the process and reassuring them about the site’s safety can reduce anxiety. While the anterolateral thigh is not the standard location for hepatitis A vaccination, its use in specific cases highlights the flexibility of immunization practices, ensuring that no one is left behind due to physical limitations or developmental stages.
Global Vaccination Leader: Which Country Tops the Immunization Chart?
You may want to see also
Explore related products




![]()
Intramuscular Delivery: The vaccine is given intramuscularly to ensure proper absorption and immune response
The hepatitis A vaccine is administered intramuscularly, typically in the deltoid muscle of the upper arm for adults and older children, or the vastus lateralis muscle of the thigh for infants and younger children. This method ensures the vaccine reaches muscle tissue, where it can be effectively absorbed and trigger a robust immune response. Unlike subcutaneous injections, which deliver medication into the fatty layer beneath the skin, intramuscular delivery bypasses this layer, allowing for faster uptake by the bloodstream and subsequent activation of the immune system.
Intramuscular administration is crucial for the hepatitis A vaccine because it contains inactivated virus particles. These particles need to be presented to the immune system in a way that mimics a natural infection, stimulating the production of antibodies without causing the disease itself. Muscle tissue, being highly vascularized, provides an ideal environment for this process. The vaccine’s antigens are rapidly taken up by immune cells in the muscle, transported to lymph nodes, and processed to initiate an immune response. This response includes the production of memory cells, offering long-term protection against hepatitis A.
For optimal results, healthcare providers follow specific guidelines when administering the hepatitis A vaccine intramuscularly. The recommended dose for adults and children aged 1 year and older is 0.5 mL. In adults, the deltoid muscle is the preferred site, with the injection given at a 90-degree angle. For children aged 12 months to 3 years, the mid-thigh (vastus lateralis) is used, as the deltoid muscle is not yet sufficiently developed. Proper needle length is critical to ensure the vaccine reaches the muscle tissue without causing injury. For example, a 1-inch needle is typically used for adults, while a 5/8-inch needle is appropriate for young children.
While intramuscular delivery is highly effective, it’s essential to follow post-injection care to minimize discomfort. Applying a cold compress to the injection site can reduce pain and swelling. Avoiding strenuous activity with the vaccinated arm or leg for a few hours can also prevent soreness. Mild side effects, such as redness, swelling, or tenderness at the injection site, are common and usually resolve within a few days. If severe pain or persistent symptoms occur, consulting a healthcare provider is advisable.
In comparison to other vaccine delivery methods, such as oral or subcutaneous administration, intramuscular injection offers distinct advantages for the hepatitis A vaccine. Oral vaccines, while convenient, may not provide consistent immune responses due to variability in gastrointestinal absorption. Subcutaneous injections, on the other hand, are less effective for inactivated vaccines like hepatitis A because they do not deliver the antigen directly to muscle tissue, where immune activation is most efficient. Intramuscular delivery, therefore, remains the gold standard for ensuring proper absorption and a strong, lasting immune response against hepatitis A.
Hepatitis B Vaccine Ingredients: A Comprehensive Breakdown of Components
You may want to see also
![]()
Avoiding Subcutaneous: Incorrect subcutaneous administration can reduce the vaccine's effectiveness and protection
The hepatitis A vaccine is typically administered intramuscularly, most often in the deltoid muscle of the upper arm for adults and older children, or the vastus lateralis muscle of the thigh for infants and younger children. This precise delivery method ensures optimal absorption and immune response. However, confusion can arise, leading to incorrect subcutaneous administration—a mistake that significantly compromises the vaccine’s effectiveness. Subcutaneous injection places the vaccine in the fatty tissue just beneath the skin, where it is absorbed more slowly and less efficiently, potentially reducing the body’s ability to mount a robust immune defense against hepatitis A.
Consider the dosage and age-specific guidelines for the hepatitis A vaccine. For adults and children over 18 months, a standard dose of 0.5 mL is administered intramuscularly. In younger children (12–23 months), the dose is often reduced to 0.25 mL, but the route remains intramuscular. When administered subcutaneously, even the correct dosage may fail to elicit the intended immune response. For instance, studies have shown that subcutaneous administration can result in lower antibody titers compared to intramuscular delivery, leaving individuals more vulnerable to infection. This risk underscores the importance of adhering to the recommended injection technique.
To avoid subcutaneous administration, healthcare providers must carefully select the injection site and use proper technique. For the deltoid muscle, the needle should be inserted at a 90-degree angle, while for the vastus lateralis, a 90-degree angle is also recommended, ensuring the vaccine reaches the muscle tissue. Practical tips include palpating the muscle to confirm the correct location and using the appropriate needle length—typically 1 inch for adults and 5/8 inch for children. For infants, a 5/8 inch needle is often sufficient, but the injection should be given in the anterolateral thigh muscle. These details may seem minor, but they are critical to ensuring the vaccine’s full protective effect.
The consequences of incorrect administration extend beyond individual protection. In settings like travel clinics or mass vaccination campaigns, where hepatitis A vaccines are frequently administered, systemic errors in technique could lead to widespread underprotection. This not only increases the risk of outbreaks but also erodes public trust in vaccination programs. For example, a 2015 study found that subcutaneous administration of a similar vaccine resulted in a 30% reduction in seroprotection rates compared to intramuscular delivery. Such findings highlight the need for rigorous training and adherence to protocols in all healthcare settings.
In conclusion, while the hepatitis A vaccine is a powerful tool in preventing infection, its effectiveness hinges on proper administration. Avoiding subcutaneous injection is not merely a technical detail—it is a critical step in ensuring the vaccine’s full potential is realized. By understanding the specific requirements for dosage, injection site, and technique, healthcare providers can safeguard both individual and community health. This precision in practice transforms a simple injection into a robust shield against hepatitis A.
Pregnant Women: Vaccines and Testing
You may want to see also
![]()
Post-Injection Care: Mild soreness at the injection site is normal; apply a cold compress if needed
The hepatitis A vaccine is typically administered in the deltoid muscle of the upper arm for adults and older children, while infants and younger children may receive it in the vastus lateralis muscle of the thigh. Regardless of the location, experiencing mild soreness at the injection site is a common and expected reaction. This localized discomfort is your body’s natural response to the vaccine as it begins to build immunity. While it’s usually mild and resolves within a few days, understanding how to manage this soreness can enhance your post-vaccination experience.
For those who find the soreness bothersome, applying a cold compress to the injection site can provide relief. Use an ice pack wrapped in a thin cloth to avoid direct contact with the skin, and apply it for 10–15 minutes at a time, several times a day as needed. Avoid heat, as it can increase inflammation and worsen discomfort. Additionally, gently moving or using the arm or leg where the vaccine was administered can help reduce stiffness and improve circulation, aiding in faster recovery.
It’s important to note that while mild soreness is normal, severe pain, redness, or swelling that persists or worsens should prompt a consultation with a healthcare provider. These could be signs of an uncommon but more serious reaction. For most individuals, however, the discomfort is minimal and manageable with simple at-home care. Remember, this temporary soreness is a small price for the long-term protection the hepatitis A vaccine provides against a potentially severe liver infection.
Practical tips include wearing loose-fitting clothing to avoid irritation at the injection site and avoiding strenuous activity involving the vaccinated limb for the first 24–48 hours. Over-the-counter pain relievers like acetaminophen can be considered if the soreness interferes with daily activities, but consult a healthcare provider before taking any medication, especially in children or individuals with underlying health conditions. By following these simple post-injection care steps, you can minimize discomfort and focus on the benefits of vaccination.
Understanding Vaccination Law Exemptions: Key Provisions and Requirements Explained
You may want to see also
Frequently asked questions
The Hepatitis A vaccine is typically administered as an intramuscular injection into the deltoid muscle of the upper arm for adults and older children, or into the anterolateral aspect of the thigh for infants and young children.
While it is possible to administer the Hepatitis A vaccine in the gluteal (buttock) muscle, it is not the preferred site. The deltoid muscle in the arm is the recommended location for adults and older children.
The Hepatitis A vaccine is administered intramuscularly, meaning it is injected directly into the muscle tissue, not under the skin (subcutaneously).
Yes, the injection site differs by age. For adults and older children, the vaccine is given in the deltoid muscle of the upper arm, while for infants and young children, it is administered in the anterolateral thigh muscle.