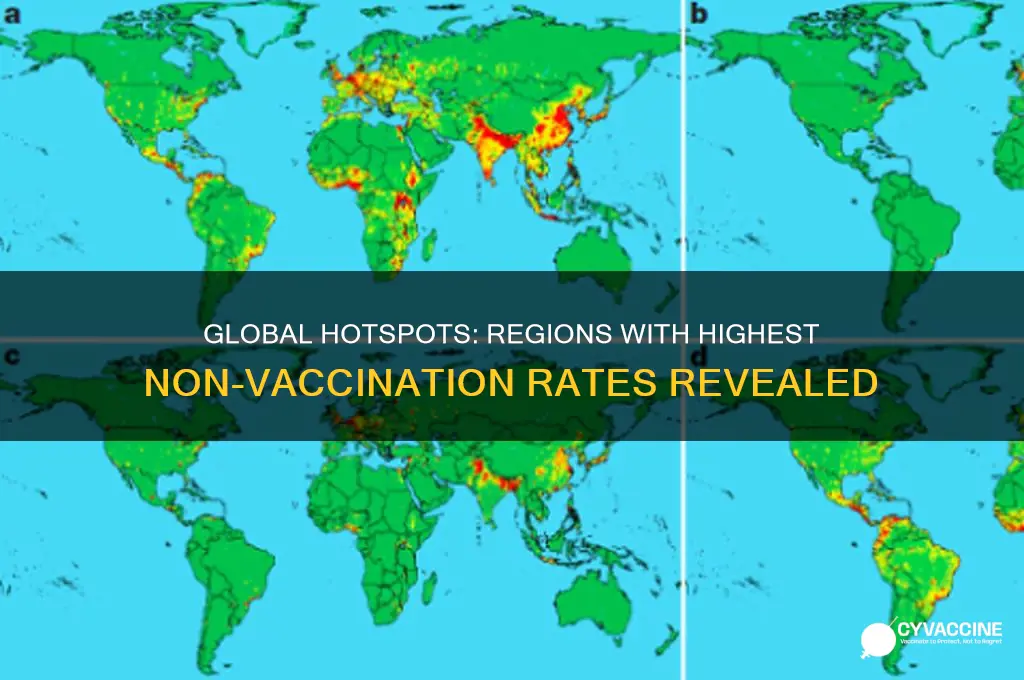
The issue of non-vaccination rates varies significantly across regions, with certain areas reporting the largest percentages of unvaccinated populations. Factors such as socioeconomic status, access to healthcare, cultural beliefs, and misinformation play a critical role in these disparities. Developing countries often face higher non-vaccination rates due to limited healthcare infrastructure and resource constraints, while in some developed nations, vaccine hesitancy driven by misinformation and distrust in medical institutions has led to pockets of low vaccination coverage. Identifying these regions is essential for targeted public health interventions to improve immunization rates and prevent the spread of preventable diseases.
Explore related products





What You'll Learn
![]()
Regional disparities in vaccine access
The global distribution of vaccines reveals stark regional disparities, with low-income countries often bearing the brunt of limited access. For instance, as of 2023, Africa accounted for less than 5% of global COVID-19 vaccine doses administered, despite being home to 17% of the world’s population. This imbalance is not unique to COVID-19; it mirrors historical patterns in vaccine access for diseases like measles and polio. Supply chain challenges, including refrigeration requirements for certain vaccines (e.g., mRNA vaccines needing ultra-cold storage), exacerbate these disparities, particularly in regions with unreliable electricity or infrastructure.
Consider the logistical hurdles in rural areas of sub-Saharan Africa or Southeast Asia, where transporting vaccines over long distances can be prohibitively expensive. In these regions, a single dose of a vaccine might cost the same as in high-income countries, but the indirect costs—transport, storage, and administration—skyrocket. For example, the Pfizer-BioNTech COVID-19 vaccine requires storage at -70°C, a standard nearly impossible to meet in areas without advanced medical facilities. This creates a vicious cycle: without infrastructure, vaccines remain inaccessible, and without access, there’s little incentive to build infrastructure.
To address these disparities, global initiatives like COVAX aimed to distribute 2 billion vaccine doses to low-income countries by 2022. However, by mid-2022, only 1.4 billion doses had been delivered, falling short of the target. Wealthier nations’ vaccine hoarding and patent restrictions on vaccine production further widened the gap. For instance, while high-income countries secured booster doses for their populations, many low-income countries struggled to administer even a single dose to high-risk groups like healthcare workers and the elderly.
A comparative analysis highlights the contrast between regions. In North America and Europe, vaccination rates for diseases like measles exceed 90%, while in parts of Africa and Asia, they hover below 60%. This disparity isn’t just a health issue—it’s an economic one. Unvaccinated populations are more susceptible to outbreaks, which can cripple local economies and strain global health systems. For example, a measles outbreak in the Democratic Republic of Congo in 2019 infected over 300,000 people, overwhelming healthcare facilities and diverting resources from other critical areas.
Practical solutions exist, but they require global cooperation. Waiving vaccine patents, as proposed by India and South Africa, could enable local production in low-income countries. Investing in cold-chain infrastructure and developing heat-stable vaccines (like the oral polio vaccine) would reduce reliance on expensive storage solutions. Additionally, community-based vaccination campaigns, leveraging local leaders and mobile clinics, have proven effective in reaching remote populations. For instance, in Ethiopia, health workers on motorcycles delivered vaccines to rural villages, increasing coverage by 20% in just one year.
In conclusion, regional disparities in vaccine access are a solvable problem, but they demand urgent, coordinated action. By addressing logistical, economic, and political barriers, the global community can ensure that vaccines reach those who need them most, regardless of where they live.
Vaccines for Your Pet: Filing an Insurance Claim
You may want to see also
Explore related products






![]()
Impact of misinformation on vaccination rates
Misinformation spreads like a virus, infecting communities with doubt and fear, particularly when it comes to vaccinations. In regions where non-vaccination rates are highest—such as parts of the United States, Eastern Europe, and certain African countries—misinformation campaigns often exploit cultural, religious, or political vulnerabilities. For instance, false claims linking vaccines to autism or infertility have taken root in communities with limited access to reliable health information. These myths, amplified by social media, create a cycle of mistrust that undermines public health efforts. The result? Outbreaks of preventable diseases like measles and polio persist, disproportionately affecting children under five, who are most vulnerable to complications.
Consider the role of social media algorithms in this crisis. Platforms designed to maximize engagement inadvertently prioritize sensational, often false, content over factual health information. A study found that anti-vaccine posts receive 50% more engagement than pro-vaccine content, ensuring misinformation reaches a wider audience. In countries like the Philippines, where vaccine confidence plummeted after a dengue vaccine controversy, social media played a pivotal role in spreading fear. Health authorities struggled to counteract the narrative, even as measles cases surged by 500% in 2019. This highlights the urgent need for digital literacy programs that teach users to critically evaluate online information.
To combat misinformation, public health campaigns must adapt to local contexts. In Somalia, where polio remains endemic, vaccine hesitancy is fueled by rumors of foreign interference. Successful initiatives have involved partnering with religious leaders to endorse vaccination, aligning health messaging with cultural values. Similarly, in the U.S., community-based programs in states like Oregon and Idaho have used peer educators to address concerns about vaccine safety. These efforts emphasize transparency—acknowledging rare side effects while stressing the overwhelming benefits of immunization. For example, the MMR vaccine is 97% effective after two doses, yet misinformation often obscures this critical fact.
Finally, policymakers must address systemic issues that amplify misinformation’s impact. In low-income regions, inadequate healthcare infrastructure leaves populations reliant on unverified sources for health advice. Investing in accessible, trusted healthcare services is essential. Additionally, regulatory measures to hold social media platforms accountable for disseminating harmful content are overdue. Until these steps are taken, misinformation will continue to erode vaccination rates, leaving communities vulnerable to preventable diseases. The fight against misinformation is not just about correcting falsehoods—it’s about rebuilding trust in science and institutions.
Adacel Tdap Vaccine: Effective Protection Against Whooping Cough?
You may want to see also
Explore related products






![]()
Economic barriers to vaccine distribution
Low-income countries face a stark reality: vaccine distribution often hinges on affordability, not just availability. The COVID-19 pandemic exposed this brutally. While wealthier nations secured doses through advance purchase agreements, many low-income countries relied on COVAX, a global vaccine-sharing initiative. However, COVAX struggled to compete with wealthy nations' buying power, leading to delayed deliveries and insufficient supply. This disparity highlights how economic barriers create a two-tiered system, leaving vulnerable populations at higher risk.
A single dose of the Pfizer-BioNTech COVID-19 vaccine, for instance, cost roughly $20 in 2021. For a country with a GDP per capita of $500, vaccinating even a fraction of its population becomes an insurmountable financial burden. This price tag doesn't include the cold chain infrastructure required for storage and transportation, further exacerbating the challenge.
Beyond the initial cost of vaccines, weak healthcare infrastructure in many low-income countries creates additional economic hurdles. Training healthcare workers, establishing distribution networks, and maintaining cold chains require significant investment. Countries already struggling with limited resources are forced to divert funds from other essential health services, creating a vicious cycle of underinvestment.
Imagine a rural clinic in sub-Saharan Africa. Even if vaccines arrive, the lack of reliable electricity for refrigeration or trained personnel to administer doses renders them useless. This logistical complexity underscores the need for comprehensive solutions that address not just vaccine procurement but also the underlying economic and infrastructural deficiencies.
Breaking down economic barriers requires a multi-pronged approach. Wealthy nations must prioritize equitable vaccine distribution through initiatives like COVAX, ensuring fair pricing and timely deliveries. Debt relief and increased foreign aid can provide low-income countries with the financial flexibility to invest in healthcare infrastructure. Additionally, technology transfer and local vaccine production can reduce costs and increase accessibility in the long term.
Avoid These Foods Post-Yellow Fever Vaccine for Optimal Recovery
You may want to see also
Explore related products






![]()
Cultural and religious beliefs affecting uptake
In regions like Nigeria, Pakistan, and Afghanistan, cultural and religious beliefs significantly influence vaccine hesitancy, often overshadowing public health campaigns. For instance, in northern Nigeria, rumors that polio vaccines were part of a Western plot to sterilize Muslim children led to widespread refusal, allowing polio to persist long after global eradication efforts began. This mistrust, rooted in historical colonialism and religious interpretations, highlights how cultural narratives can override scientific evidence, even when vaccines are free and accessible.
Consider the role of religious leaders in shaping vaccine uptake. In Orthodox Jewish communities in New York and Israel, some leaders have questioned the safety of vaccines, citing concerns over ingredients or perceived interference with divine will. Similarly, in parts of Indonesia, the misconception that vaccines contain haram (forbidden) substances like pork gelatin has deterred uptake, despite halal-certified alternatives being available. Engaging religious authorities as allies, rather than adversaries, could bridge this gap—for example, by emphasizing the Islamic principle of preserving life or the Jewish mandate to heal (pikuach nefesh).
A comparative analysis reveals that cultural beliefs often intersect with socioeconomic factors. In Japan, historically low MMR vaccine uptake (around 1-2% in the 1990s) was driven by government mistrust after a 1989 court ruling linked the vaccine to adverse effects, not religious objections. Contrast this with Somalia, where Al-Shabaab militants blocked polio vaccination drives, framing them as Western interference in Muslim affairs. These examples underscore that while cultural and religious beliefs are powerful, their impact is amplified or mitigated by political instability, misinformation, and state policies.
To address this, public health strategies must be culturally sensitive and context-specific. In India, for example, the introduction of the measles-rubella vaccine faced resistance in some Hindu communities due to rumors it was a population control measure. Local health workers countered this by involving village elders and using culturally relevant messaging, such as linking vaccination to protecting the community’s future. Similarly, in Ethiopia, Orthodox Christian leaders were trained to dispel myths about the HPV vaccine, framing it as a tool to prevent cervical cancer, a leading cause of death among women.
Ultimately, understanding the interplay between cultural, religious, and historical factors is crucial for tailoring interventions. For instance, in Haiti, Vodou practitioners have been enlisted to promote vaccines by aligning them with spiritual protection. Such approaches require humility, patience, and a willingness to listen to communities’ concerns. By respecting cultural and religious beliefs while providing accurate, actionable information, public health efforts can build trust and increase vaccine uptake, even in the most hesitant populations.
Emergency Approval for Vaccines: What It Means and Why It Matters
You may want to see also
Explore related products






![]()
Logistical challenges in remote or conflict zones
In remote or conflict zones, the cold chain—the temperature-controlled supply chain essential for vaccine viability—often collapses. Solar-powered refrigerators, a lifeline in such areas, require consistent sunlight, which is unreliable in regions like the Democratic Republic of Congo or South Sudan. A single break in the cold chain can render an entire batch of vaccines ineffective, wasting resources and leaving populations unprotected. For instance, the measles vaccine loses potency above 8°C, yet in many remote areas, temperatures fluctuate wildly, and backup power systems are nonexistent.
Consider the delivery of vaccines to a village in Afghanistan’s mountainous terrain. Roads are unpaved, if they exist at all, and armed checkpoints delay or block access. Drones have been piloted in Rwanda and Ghana to bypass these obstacles, but their range is limited, and they cannot carry bulk shipments. Ground transport remains the default, yet vehicles risk ambush or breakdown. Each trip becomes a gamble, with drivers risking their lives to deliver doses that may expire en route.
Conflict zones add another layer of complexity: insecurity. In Syria, for example, warring factions often target medical facilities, viewing them as strategic assets. Vaccination teams must negotiate safe passage, sometimes paying bribes or coordinating with multiple armed groups. Even when access is granted, mistrust runs deep. Rumors spread that vaccines are weapons of foreign powers, discouraging participation. Building trust requires local leaders as advocates, but even they may be displaced or threatened.
Practical solutions exist but demand creativity and funding. Pre-filled auto-disable syringes reduce waste and ensure accurate dosing, critical when trained health workers are scarce. Mobile clinics, often operated by NGOs like Médecins Sans Frontières, bring vaccines directly to communities, though they too face security risks. Cash incentives for vaccinators and community health workers can improve retention, but sustained funding is rare. Donors prioritize emergencies over long-term infrastructure, leaving gaps that hinder progress.
The takeaway is clear: addressing non-vaccination in these zones requires more than vaccines. It demands resilient systems tailored to local realities. Investments in solar cold chains, drone networks, and community-based trust-building are not optional—they are essential. Without them, remote and conflict-affected populations will remain the hardest to reach, perpetuating cycles of preventable disease.
How to Verify Your Meningococcal B (MenB) Vaccination Status Easily
You may want to see also
Frequently asked questions
The largest percentage of non-vaccinations is often found in low-income countries, particularly in sub-Saharan Africa and parts of Asia, due to limited access to healthcare infrastructure, vaccine supply shortages, and logistical challenges.
In the United States, states with higher rates of non-vaccination are often found in the Pacific Northwest, parts of the Midwest, and certain rural areas, where vaccine hesitancy, lack of access, and exemptions for personal beliefs contribute to lower vaccination rates.
Rural areas generally have a larger percentage of non-vaccinations due to limited healthcare access, lower population density, and fewer vaccination clinics compared to urban areas.
Developing countries typically have the largest percentage of non-vaccinations due to poverty, inadequate healthcare systems, and challenges in distributing vaccines, whereas developed countries face non-vaccination issues primarily due to hesitancy or misinformation.