The smallpox vaccine, one of the most groundbreaking achievements in medical history, originated from the pioneering work of Edward Jenner in the late 18th century. In 1796, Jenner observed that milkmaids who had contracted cowpox, a mild disease, were subsequently immune to smallpox, a devastating and often fatal illness. Building on this insight, he inoculated an eight-year-old boy with material from a cowpox lesion, demonstrating that this procedure could protect against smallpox. This method, known as vaccination (derived from *vacca*, the Latin word for cow), laid the foundation for the global eradication of smallpox, which was officially declared by the World Health Organization in 1980. Jenner’s discovery not only saved countless lives but also marked the beginning of modern vaccinology.
| Characteristics | Values |
|---|---|
| Origin of Smallpox Vaccine | The smallpox vaccine originated from the use of cowpox virus (Vaccinia virus). |
| Discovery | Edward Jenner discovered in 1796 that milkmaids who had cowpox were immune to smallpox. |
| Vaccine Development | Jenner developed the first smallpox vaccine using material from cowpox lesions. |
| Vaccine Type | Live attenuated virus (Vaccinia virus, related to but distinct from cowpox). |
| Eradication of Smallpox | The World Health Organization (WHO) declared smallpox eradicated in 1980 due to global vaccination efforts. |
| Vaccine Mechanism | Induces immunity by exposing the immune system to a related, less harmful virus. |
| Historical Significance | First successful vaccine, paving the way for modern vaccinology. |
| Current Use | No longer routinely administered, except for high-risk groups (e.g., lab workers). |
| Storage Requirements | Freeze-dried vaccine is stable at room temperature for extended periods. |
| Side Effects | Mild fever, soreness at injection site, rare severe reactions (e.g., post-vaccinial encephalitis). |
| Global Impact | Saved millions of lives and remains a landmark achievement in public health. |
Explore related products






What You'll Learn
- Edward Jenner’s Cowpox Discovery: Jenner observed milkmaids resistant to smallpox after cowpox exposure, inspiring vaccination
- First Smallpox Vaccine: Jenner developed the vaccine in 1796 using cowpox material from a milkmaid
- Global Vaccination Campaigns: WHO led efforts in the 1960s-70s to eradicate smallpox through mass vaccination
- Cowpox vs. Smallpox Viruses: Cowpox, a milder virus, provided immunity to smallpox, forming the vaccine basis
- Eradication of Smallpox: Last natural case in 1977; declared eradicated in 1980 due to vaccination success
![]()
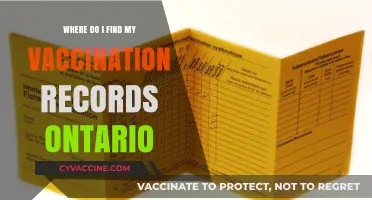
Edward Jenner’s Cowpox Discovery: Jenner observed milkmaids resistant to smallpox after cowpox exposure, inspiring vaccination
In the late 18th century, a curious phenomenon caught the attention of Edward Jenner, an English physician. He noticed that milkmaids who had contracted cowpox, a mild disease affecting cattle, seemed to be immune to the far more deadly smallpox. This observation sparked a groundbreaking idea: could exposure to cowpox protect against smallpox? Jenner’s methodical inquiry into this question laid the foundation for the world’s first vaccine. By deliberately inoculating an 8-year-old boy, James Phipps, with material from a cowpox lesion and later exposing him to smallpox, Jenner demonstrated that cowpox conferred immunity. This experiment, conducted in 1796, marked the birth of vaccination, a term derived from *vacca*, the Latin word for cow.
To replicate Jenner’s approach, one would need to follow a precise yet risky procedure by 18th-century standards. First, collect fluid from a cowpox blister, ideally from a dairy worker with a recent infection. Using a lancet, make a small incision on the arm of the recipient—typically a child, as they were less likely to have been exposed to smallpox. Introduce a small amount of the cowpox fluid into the wound, ensuring it is enough to trigger an immune response but not cause severe illness. After 6–8 weeks, when the cowpox symptoms (mild fever, pustules) subside, expose the individual to smallpox via variolation (a practice of the time). If successful, the recipient would show no signs of smallpox, proving immunity. Modern readers must note: this method is obsolete and dangerous by today’s standards, replaced by safer, lab-developed vaccines.
Jenner’s discovery was revolutionary not only for its immediate impact but also for its broader implications. It challenged the prevailing practice of variolation, which carried a 2–3% mortality rate, by offering a safer alternative. His work also introduced the concept of cross-protection, where one disease could shield against another. This principle became a cornerstone of immunology, influencing the development of vaccines for polio, measles, and other diseases. However, Jenner’s success was not without controversy. Skepticism and fear of the “animal disease” being introduced into humans led to resistance, a reminder that scientific breakthroughs often face societal hurdles.
For those interested in the practical legacy of Jenner’s work, the smallpox vaccine evolved significantly over the centuries. By the 20th century, the vaccine used a virus called vaccinia, a relative of cowpox, administered via a bifurcated needle. The dosage was standardized: 0.0025 mL applied through 15 jabs on the upper arm, creating a localized infection that triggered immunity. This method, combined with global vaccination campaigns, led to smallpox’s eradication in 1980. Today, vaccination remains a cornerstone of public health, and Jenner’s cowpox discovery serves as a testament to the power of observation and experimentation in solving humanity’s greatest challenges.
Meningo vs. Meningitis Vaccine: Clearing Up the Confusion
You may want to see also
Explore related products






![]()
First Smallpox Vaccine: Jenner developed the vaccine in 1796 using cowpox material from a milkmaid
The origins of the smallpox vaccine trace back to a groundbreaking observation in 1796, when Edward Jenner, an English physician, noticed that milkmaids who contracted cowpox, a milder disease, were subsequently immune to smallpox. This insight led Jenner to develop the first smallpox vaccine using material from a cowpox lesion on a milkmaid’s hand. His method involved inoculating an 8-year-old boy, James Phipps, with cowpox pus, then exposing him to smallpox to test immunity. The experiment succeeded, marking the birth of modern vaccination.
Jenner’s approach was both innovative and risky by 18th-century standards. Unlike the dangerous practice of variolation (deliberately infecting individuals with smallpox to induce mild cases), his vaccine used a related but safer virus. The cowpox material was harvested from lesions, often on the hands of milkmaids, and introduced into the skin via a shallow scratch. This method, known as arm-to-arm transfer, became the standard until the development of laboratory-cultured vaccines in the 19th century.
The success of Jenner’s vaccine relied on its ability to stimulate cross-immunity between cowpox and smallpox, both caused by orthopoxviruses. A single dose provided lifelong protection for most recipients, though later research refined the process to ensure consistency and safety. By the mid-20th century, global vaccination campaigns, using freeze-dried vaccines and bifurcated needles for precise delivery (0.0025 mL per dose), eradicated smallpox by 1980.
Practical implementation of Jenner’s vaccine faced challenges, including skepticism and logistical hurdles in distributing the live virus. Early vaccination efforts required a chain of infected individuals to maintain the cowpox material, as it could not be preserved long-term. Despite these limitations, Jenner’s work laid the foundation for immunology and inspired future vaccine development. His method remains a testament to the power of observation and the transformative potential of scientific curiosity.
Today, Jenner’s vaccine serves as a historical benchmark, reminding us of the importance of understanding disease ecology and leveraging natural immunity. While smallpox is eradicated, his principles continue to guide vaccine research, emphasizing the need for safety, efficacy, and accessibility. The story of the milkmaid’s cowpox lesion is not just a footnote in history but a practical guide to how simple observations can lead to monumental breakthroughs.
Booster Shot vs. Original Vaccine: Key Differences Explained
You may want to see also
Explore related products





![]()
Global Vaccination Campaigns: WHO led efforts in the 1960s-70s to eradicate smallpox through mass vaccination
The World Health Organization's (WHO) smallpox eradication campaign in the 1960s and 1970s stands as a monumental achievement in global health, demonstrating the power of coordinated international efforts. This initiative, which aimed to eliminate a disease that had plagued humanity for centuries, was built upon the foundation of the smallpox vaccine, a tool that had been refined over decades. The vaccine's origins can be traced back to the late 18th century, when Edward Jenner developed the concept of vaccination using cowpox material, a less virulent relative of smallpox. This breakthrough laid the groundwork for the creation of a safe and effective vaccine, which was further improved upon by scientists like Louis Pasteur and others who contributed to its large-scale production and distribution.
The WHO's strategy for smallpox eradication involved a multi-pronged approach, combining mass vaccination campaigns with surveillance, containment, and ring vaccination. The vaccine used during this period was the lymph-derived smallpox vaccine, produced from the New York City Board of Health (NYCBOH) strain. This vaccine was administered using a bifurcated needle, which allowed for the delivery of a precise dose (approximately 0.0025 mL) just below the skin's surface. The target population for vaccination included individuals of all ages, with a particular focus on children and young adults, as they were more susceptible to the disease. In areas with active transmission, the vaccine was often given to everyone, regardless of age, to create a "firebreak" around the infection.
One of the critical challenges faced by the WHO was ensuring the vaccine's potency and safety in diverse environmental conditions. The smallpox vaccine needed to be stored at temperatures between 2-8°C (36-46°F) to maintain its efficacy, which posed significant logistical hurdles in regions with limited refrigeration infrastructure. To address this, the WHO implemented a system of vaccine distribution that included the use of cold boxes, vaccine carriers, and other innovative solutions to maintain the cold chain. Additionally, health workers were trained to administer the vaccine correctly, ensuring that the proper dosage and technique were used to maximize immunity and minimize adverse reactions.
A key aspect of the WHO's campaign was its emphasis on community engagement and education. Local health workers, often volunteers, played a vital role in disseminating information about the vaccine, addressing misconceptions, and encouraging participation. This grassroots approach was essential in overcoming cultural barriers and building trust in the vaccination program. For instance, in some communities, traditional leaders were involved in promoting the vaccine, while in others, schools and religious institutions served as vaccination sites. By tailoring their strategies to local contexts, the WHO was able to achieve high vaccination coverage rates, even in remote and hard-to-reach areas.
The success of the WHO's smallpox eradication campaign offers valuable lessons for contemporary global health initiatives. It underscores the importance of international collaboration, innovative problem-solving, and community-centered approaches in tackling complex health challenges. The campaign's legacy extends beyond the eradication of smallpox, serving as a model for subsequent efforts to combat diseases like polio, measles, and, more recently, COVID-19. As we reflect on the origins of the smallpox vaccine and the WHO's historic campaign, we are reminded of the transformative potential of vaccines and the critical role of global cooperation in safeguarding public health. Practical tips from this era, such as the use of bifurcated needles and cold chain management, continue to inform vaccination strategies today, ensuring that the lessons learned from smallpox eradication remain relevant and applicable in the modern context.
Understanding Meningitis Vaccine: Shots Required for Full Protection
You may want to see also
Explore related products





![]()
Cowpox vs. Smallpox Viruses: Cowpox, a milder virus, provided immunity to smallpox, forming the vaccine basis
The discovery of the smallpox vaccine is a testament to the power of observation and the interplay between human and animal health. In the late 18th century, English physician Edward Jenner noticed that milkmaids who contracted cowpox, a mild disease in humans, were subsequently immune to smallpox, a devastating and often fatal illness. This observation laid the foundation for the world’s first vaccine, revolutionizing medicine and public health.
Cowpox and smallpox, though distinct viruses, share a critical similarity: they belong to the *Orthopoxvirus* genus, allowing the immune system to recognize and combat both. Cowpox, primarily affecting cattle and occasionally humans, causes localized lesions and mild symptoms, whereas smallpox induces severe systemic illness, including high fever, widespread rash, and significant mortality rates. Jenner’s insight was to harness cowpox’s mild nature to induce immunity against smallpox. By inoculating a young boy, James Phipps, with material from a cowpox lesion in 1796, Jenner demonstrated that exposure to cowpox prevented smallpox infection—a breakthrough that would eventually lead to smallpox eradication.
The process of creating the smallpox vaccine, known as vaccination (derived from *vacca*, Latin for cow), involved extracting lymph fluid from cowpox lesions on infected cows and introducing a small dose into the skin of a human recipient. This method, while rudimentary by modern standards, stimulated a protective immune response without causing severe illness. Over time, the vaccine evolved, with purified forms of the vaccinia virus (a related but distinct virus) replacing cowpox material. Standardized dosages, typically administered via a bifurcated needle, ensured consistent immunity, with a single dose providing protection for 3–5 years and a booster extending immunity for decades.
Comparing cowpox and smallpox highlights the elegance of Jenner’s approach. Cowpox’s mildness made it an ideal candidate for a live-virus vaccine, as it posed minimal risk while conferring robust immunity. In contrast, smallpox’s virulence necessitated a safer alternative, which cowpox provided. This natural cross-immunity exemplifies how understanding viral relationships can lead to innovative solutions. For instance, modern vaccines often use attenuated or related viruses to mimic infection without causing disease, a principle directly descended from Jenner’s work.
Practical implementation of the smallpox vaccine required careful consideration of age and health status. Vaccination was typically administered to children over 1 year old, as younger infants retained maternal antibodies that could interfere with immune response. Side effects, such as fever or localized soreness, were generally mild but warranted monitoring. The vaccine’s success in eradicating smallpox by 1980 underscores its efficacy, though it is no longer routinely administered due to the virus’s extinction in the wild. For those at risk (e.g., lab workers handling smallpox), the vaccinia-based vaccine remains available, with precautions for immunocompromised individuals to avoid adverse reactions. This historical and scientific interplay between cowpox and smallpox continues to inspire vaccine development, reminding us of the enduring impact of Jenner’s observation.
Understanding Meningococcal Vaccine Blood Titer Testing: What You Need to Know
You may want to see also
Explore related products





![]()
Eradication of Smallpox: Last natural case in 1977; declared eradicated in 1980 due to vaccination success
The last natural case of smallpox occurred in 1977, marking a pivotal moment in medical history. This achievement was the culmination of a global vaccination campaign led by the World Health Organization (WHO), which systematically targeted high-risk areas and implemented ring vaccination strategies. Unlike mass vaccination, ring vaccination focused on immunizing close contacts of infected individuals, effectively containing outbreaks. The vaccine used, derived from the vaccinia virus, was administered via a bifurcated needle, delivering a precise 0.0025 mL dose into the skin’s superficial layers. This method ensured immunity with minimal adverse effects, proving both practical and cost-effective for widespread use.
Analyzing the success of smallpox eradication reveals the critical role of international collaboration and public health infrastructure. The campaign’s effectiveness hinged on surveillance systems that rapidly identified cases and mobilized response teams. Vaccination teams often worked in remote, resource-limited settings, requiring adaptability and resilience. For instance, in Ethiopia and Somalia, health workers traveled on foot or by camel to reach isolated communities, demonstrating the lengths taken to ensure no one was left unvaccinated. This effort underscores the importance of accessibility and community engagement in public health initiatives.
From a practical standpoint, the smallpox vaccine’s administration required specific training. Health workers were instructed to dip the bifurcated needle into the vaccine solution, ensuring it held the correct dose, then puncture the skin 15 times in a small area, typically on the upper arm. The resulting “take”—a localized lesion—indicated a successful immune response. While the vaccine was generally safe, precautions were taken for individuals with compromised immune systems or skin conditions, highlighting the need for tailored approaches in vaccination programs.
Comparing smallpox eradication to ongoing efforts against diseases like polio or COVID-19 reveals both similarities and challenges. While smallpox had no animal reservoir and a highly effective vaccine, diseases like polio require continuous vaccination due to persistent transmission. The smallpox campaign’s success was also facilitated by its visible symptoms, allowing for easier case identification. In contrast, asymptomatic transmission in diseases like COVID-19 complicates containment. Nonetheless, the smallpox model provides a blueprint for global health strategies, emphasizing surveillance, vaccination, and international cooperation.
The eradication of smallpox stands as a testament to the power of vaccination and collective action. It serves as a reminder that even the most devastating diseases can be overcome with sustained effort and innovation. For public health practitioners today, the lessons from smallpox include the importance of equitable vaccine distribution, community trust, and adaptive strategies. As we face new health challenges, the smallpox story remains a guiding example of what is possible when science and solidarity converge.
Is RSV Vaccine Free for Seniors in Australia? What You Need to Know
You may want to see also
Frequently asked questions
The smallpox vaccine originated from the work of Edward Jenner in 1796. Jenner observed that milkmaids who contracted cowpox, a milder disease, were immune to smallpox. He developed the vaccine by using material from cowpox lesions to inoculate humans, providing protection against smallpox.
Earlier smallpox prevention methods, such as variolation, involved deliberately infecting individuals with smallpox to induce a milder form of the disease and subsequent immunity. However, this method carried a risk of severe illness or death. Jenner's vaccine, derived from cowpox, was safer and more effective, as it provided immunity without exposing individuals to smallpox itself.
The World Health Organization (WHO) played a pivotal role in the global eradication of smallpox through its intensified vaccination campaigns in the 1960s and 1970s. Led by figures like Donald Henderson, the WHO coordinated efforts to vaccinate populations in affected areas, monitor outbreaks, and contain the virus. Smallpox was officially declared eradicated in 1980.