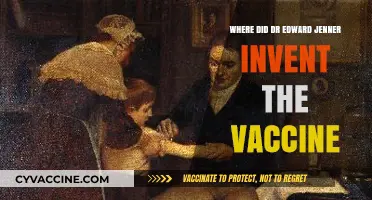
In the 1970s, Armenia, then part of the Soviet Union, implemented widespread tuberculosis (TB) vaccination campaigns as part of its public health strategy. The Bacillus Calmette-Guérin (BCG) vaccine, developed in the early 20th century, was administered to newborns and young children across the country to combat the prevalence of TB, which was a significant health concern in the region. Vaccinations were typically carried out in maternity hospitals, pediatric clinics, and local healthcare facilities, ensuring broad accessibility. This systematic approach reflected the Soviet Union's emphasis on preventive medicine and public health, leaving a lasting impact on Armenia's efforts to control TB.
| Characteristics | Values |
|---|---|
| Country | Armenia |
| Vaccine Type | BCG (Bacillus Calmette-Guérin) |
| Target Population | Newborns and infants |
| Vaccination Period | 1970s |
| Administration Site | Typically in hospitals or maternity wards |
| Coverage | High, as part of the Soviet Union's universal BCG vaccination program |
| Purpose | Prevention of tuberculosis (TB) |
| Historical Context | Part of the Soviet Union's public health initiatives during the 1970s |
| Current Status | BCG vaccination remains part of Armenia's national immunization program |
| Effectiveness | Provides moderate protection against severe forms of TB, especially in children |
| Side Effects | Generally mild, such as a small scar at the injection site or localized infection |
| Global Comparison | Similar to other Soviet republics and many low-to-middle-income countries during that era |
Explore related products






What You'll Learn
- Vaccination Locations: Hospitals, clinics, and schools were primary sites for TB vaccinations in Armenia during the 1970s
- Vaccine Type: BCG vaccine was widely administered to newborns and children to prevent tuberculosis
- Government Campaigns: State-led health initiatives ensured widespread TB vaccination coverage across Armenian populations
- Urban vs. Rural Access: Urban areas had better access, while rural regions faced logistical challenges in vaccination
- Health Records: Vaccination data was documented in medical records, often linked to school enrollment systems
![]()
Vaccination Locations: Hospitals, clinics, and schools were primary sites for TB vaccinations in Armenia during the 1970s
In the 1970s, Armenia's tuberculosis (TB) vaccination campaigns were a cornerstone of public health, with hospitals, clinics, and schools serving as the primary hubs for administering the Bacille Calmette-Guérin (BCG) vaccine. These locations were strategically chosen to maximize accessibility and ensure widespread coverage. Hospitals, equipped with medical professionals and sterile environments, were ideal for vaccinating infants shortly after birth, as recommended by the World Health Organization (WHO). Clinics, often located in urban and rural areas, provided convenient access for follow-up doses or for those who missed initial vaccinations. Schools, on the other hand, became crucial sites for mass vaccination drives, targeting children aged 6–14, a demographic particularly vulnerable to TB. This multi-pronged approach ensured that the BCG vaccine, typically administered as a single 0.05 mL intradermal dose, reached the majority of the population, significantly reducing TB incidence rates over time.
The choice of schools as vaccination sites was particularly innovative, leveraging the existing infrastructure to reach a large number of children efficiently. School-based vaccinations were often conducted during health weeks or special campaigns, with teachers and healthcare workers collaborating to organize the process. Parents were typically informed in advance, and consent forms were required, ensuring transparency and trust. For children, the experience was often routine, with minimal discomfort from the small needle used for the BCG vaccine. This method not only streamlined the vaccination process but also raised awareness about TB prevention among students and their families, fostering a culture of health consciousness.
Hospitals and clinics played a complementary role, offering more personalized care and addressing specific needs. In hospitals, newborns were vaccinated within the first few days of life, a critical window for immunity development. Clinics, especially those in remote areas, provided essential services for families without immediate access to hospitals. These facilities also served as centers for education, where parents could learn about TB symptoms, transmission, and the importance of vaccination. For instance, healthcare workers would emphasize that the BCG vaccine, while not 100% effective against all forms of TB, significantly reduces the risk of severe disease in children, particularly TB meningitis and miliary TB.
Despite the success of these vaccination sites, challenges existed. Logistical issues, such as vaccine supply chain management and cold storage requirements, occasionally disrupted campaigns. Additionally, ensuring consistent participation, especially in rural areas, required ongoing community engagement and outreach efforts. However, the dedication of healthcare workers and the strategic use of hospitals, clinics, and schools as vaccination hubs were instrumental in making Armenia's TB vaccination program one of the most effective in the region during the 1970s.
In retrospect, the focus on hospitals, clinics, and schools as vaccination locations highlights a practical and community-oriented approach to public health. This model not only facilitated the widespread administration of the BCG vaccine but also laid the groundwork for future immunization programs. For those interested in replicating such strategies, key takeaways include the importance of leveraging existing institutions, ensuring community involvement, and addressing logistical challenges proactively. By studying Armenia's experience, other countries can gain valuable insights into designing effective vaccination campaigns tailored to their unique contexts.
Meningitis Vaccine Cost in Houston, TX: What You Need to Know
You may want to see also
Explore related products






![]()
Vaccine Type: BCG vaccine was widely administered to newborns and children to prevent tuberculosis
In the 1970s, the BCG (Bacillus Calmette-Guérin) vaccine was a cornerstone of public health efforts in Armenia, as in many other countries, to combat tuberculosis (TB). Administered primarily to newborns and young children, this vaccine was a critical preventive measure in a time when TB was a significant health threat. The BCG vaccine is unique in that it is typically given as a single dose, usually within the first few days of life, to ensure early protection. This practice was particularly important in Armenia, where TB prevalence was high, and early intervention was key to reducing the disease’s impact on the population.
The BCG vaccine works by exposing the immune system to a weakened strain of Mycobacterium bovis, which is closely related to the bacterium that causes TB in humans. This exposure primes the immune system to recognize and combat the TB bacterium more effectively if encountered later in life. For Armenian newborns, the vaccine was typically administered intradermally—a small dose injected just beneath the skin, often on the upper arm. This method ensures a localized immune response and leaves a characteristic scar, which became a common mark among those vaccinated during this period. The dosage for infants was standardized at 0.05 mL, a precise amount that balanced efficacy with safety.
While the BCG vaccine is highly effective in preventing severe forms of TB in children, such as TB meningitis, its protection against pulmonary TB in adults is variable. This limitation meant that while the vaccine was a vital tool in protecting Armenian children, it was part of a broader public health strategy that included early detection, treatment, and public awareness campaigns. Parents were often instructed to monitor their children for any signs of adverse reactions, such as fever or swelling at the injection site, though these were rare. The vaccine’s widespread administration in the 1970s reflects a proactive approach to public health, prioritizing prevention in a resource-constrained setting.
Comparatively, the BCG vaccine’s role in Armenia during the 1970s highlights the global disparities in TB control. In wealthier nations, declining TB rates led to the discontinuation of universal BCG vaccination, but in Armenia and other high-burden countries, it remained a necessity. This contrast underscores the importance of tailoring public health interventions to local disease patterns. For Armenian families, the BCG vaccine was not just a medical procedure but a symbol of hope—a small but significant step toward safeguarding their children’s health in a challenging environment.
Practically, the administration of the BCG vaccine in Armenia during the 1970s required careful planning and execution. Health workers were trained to handle the vaccine properly, ensuring it was stored at the correct temperature and administered using sterile techniques. Parents were educated about the vaccine’s benefits and potential side effects, fostering trust in the healthcare system. This period also saw the integration of BCG vaccination into routine immunization schedules, making it accessible to even the most remote communities. The legacy of this effort is evident in the reduced TB burden among those vaccinated, though ongoing challenges remain in achieving full TB eradication.
Essential Kids' Vaccination Schedule: A Parent's Guide to Immunizations
You may want to see also
Explore related products






![]()
Government Campaigns: State-led health initiatives ensured widespread TB vaccination coverage across Armenian populations
In the 1970s, Armenia, then part of the Soviet Union, implemented a rigorous state-led health initiative to combat tuberculosis (TB), a disease that had historically plagued the region. The government’s campaign was characterized by its systematic approach, ensuring that vaccination coverage reached even the most remote populations. At the heart of this effort was the Bacille Calmette-Guérin (BCG) vaccine, administered to newborns within the first few days of life. This early intervention was critical, as the BCG vaccine provided a foundational immunity against severe forms of TB, particularly in children. The campaign’s success hinged on the integration of vaccination into routine healthcare services, with maternity hospitals and local clinics serving as primary delivery points.
The Soviet healthcare system’s centralized structure played a pivotal role in the campaign’s effectiveness. Mandatory vaccination policies were enforced through a network of polyclinics and rural health posts, ensuring that no demographic was overlooked. Health workers were trained to administer the BCG vaccine, which required a single intradermal dose of 0.05–0.1 ml. Parents were educated on the importance of timely vaccination, and vaccination records were meticulously maintained to track compliance. This bureaucratic rigor, while sometimes criticized for its inflexibility, guaranteed that TB vaccination became a universal practice across Armenian populations, regardless of socioeconomic status or geographic location.
A key aspect of the campaign was its adaptability to local conditions. In rural areas, mobile health teams were deployed to vaccinate infants in villages lacking permanent medical facilities. These teams often combined TB vaccination with other health services, such as maternal and child health check-ups, to maximize efficiency. Urban centers, meanwhile, relied on well-established healthcare infrastructure, with vaccinations typically administered in maternity wards immediately after birth. This dual approach ensured that the campaign’s reach was both broad and deep, addressing the unique challenges of Armenia’s diverse landscape.
Despite its successes, the campaign was not without challenges. Supply chain issues occasionally disrupted vaccine availability, particularly in remote regions. Additionally, public trust in state-led initiatives varied, with some families skeptical of the vaccine’s safety or efficacy. To address these concerns, the government launched educational campaigns through radio, television, and community meetings, emphasizing the vaccine’s proven track record and the risks of TB if left unchecked. These efforts, combined with the tangible decline in TB cases, gradually solidified public confidence in the program.
The legacy of Armenia’s 1970s TB vaccination campaign is evident in the country’s continued low incidence of severe TB today. While the global health landscape has evolved, the principles of this initiative—universal access, systematic delivery, and community engagement—remain relevant. For modern health campaigns, whether in Armenia or elsewhere, the lesson is clear: state-led initiatives, when executed with precision and adaptability, can achieve remarkable public health outcomes. Practical takeaways include the importance of integrating vaccination into existing healthcare systems, leveraging mobile health services for hard-to-reach populations, and prioritizing transparent communication to build trust.
Preventable Tragedies: Infant Mortality Linked to Lack of Vaccinations
You may want to see also
Explore related products


![]()
Urban vs. Rural Access: Urban areas had better access, while rural regions faced logistical challenges in vaccination
In the 1970s, Armenia’s tuberculosis (TB) vaccination campaigns highlighted stark disparities between urban and rural access. Urban centers, such as Yerevan, benefited from centralized healthcare facilities, trained medical staff, and reliable cold chain systems to preserve the BCG vaccine’s efficacy. Rural regions, however, faced logistical hurdles: limited transportation networks, sporadic electricity for refrigeration, and fewer healthcare workers per capita. While urban children often received the standard 0.1 mL intradermal dose within the first month of life, rural infants sometimes faced delays or missed vaccinations due to these challenges.
Consider the practical implications of these disparities. In urban areas, parents could visit nearby clinics or participate in school-based vaccination drives, ensuring timely immunization. Rural families, on the other hand, often had to travel long distances to reach the nearest health post, with no guarantee of vaccine availability. For instance, a family in a remote village might wait weeks for a mobile health team to arrive, only to find the vaccine supply depleted. This inconsistency not only delayed protection but also increased the risk of TB transmission in underserved communities.
To address these gaps, health authorities implemented strategies tailored to rural contexts. Mobile vaccination units, equipped with portable cold storage, were deployed to reach isolated villages. Community health workers were trained to administer the BCG vaccine, reducing reliance on distant clinics. However, these measures were not without challenges. Fuel shortages, rough terrain, and harsh weather conditions often disrupted schedules, leaving rural populations vulnerable. In contrast, urban areas maintained steady vaccination rates, reinforcing the divide in healthcare accessibility.
The takeaway is clear: while urban Armenians benefited from systemic advantages, rural communities required innovative, context-specific solutions. For modern TB control programs, this historical lesson underscores the importance of equitable resource allocation and flexible delivery models. Rural regions, even today, demand targeted interventions—such as drone-delivered vaccines or solar-powered refrigeration—to overcome persistent logistical barriers. Bridging this urban-rural gap is not just a matter of health equity but a critical step toward eradicating TB globally.
Lost Vaccine Passport? Quick Steps to Replace and Restore Access
You may want to see also
![]()
Health Records: Vaccination data was documented in medical records, often linked to school enrollment systems
In the 1970s, Armenian children received the Bacille Calmette-Guérin (BCG) vaccine, typically administered within the first few days of life, often before hospital discharge. This early vaccination was a standard practice in the Soviet healthcare system, which Armenia was part of at the time. The BCG vaccine, delivered as a single 0.1 mL intradermal injection, left a distinctive scar, serving as an informal record of immunization. However, formal documentation of this vaccination was systematically recorded in medical records, which were often cross-referenced with school enrollment systems to ensure compliance with public health mandates.
The linkage between health and educational systems was a practical solution to track vaccination rates and maintain herd immunity. School enrollment forms frequently required proof of BCG vaccination, alongside other routine immunizations. Parents were instructed to bring their child’s medical record, known as the "meditsinskaya kartochka," to school registrars. This document, maintained by local polyclinics, included details such as the vaccine batch number, date of administration, and the healthcare provider’s signature. Failure to provide this proof could delay enrollment, though exemptions were rarely granted for medical reasons, such as severe immune deficiencies.
From an analytical perspective, this system highlights the intersection of public health and education policy. By tying vaccination records to school enrollment, authorities ensured high immunization rates while streamlining administrative processes. However, this approach also raised privacy concerns, as medical data became accessible to non-healthcare personnel. Additionally, the reliance on physical records made the system vulnerable to loss or tampering, though such instances were rare due to the centralized nature of Soviet record-keeping.
For those researching historical vaccination records today, understanding this linkage is crucial. Start by locating the "meditsinskaya kartochka" or its equivalent in family archives. If missing, contact the polyclinic in the individual’s birthplace, as these facilities often retained records for decades. For school-aged Armenians in the 1970s, cross-referencing enrollment documents with health records can provide a comprehensive immunization history. Practical tips include verifying the BCG scar’s presence, which, while not definitive proof, can corroborate documented evidence.
In conclusion, the documentation of TB vaccination data in medical records, linked to school enrollment systems, was a cornerstone of Armenia’s public health strategy in the 1970s. This system ensured widespread immunization while creating a lasting record of individual health histories. For researchers and individuals alike, understanding this mechanism provides valuable insights into both historical healthcare practices and personal medical backgrounds.
Step-by-Step Guide: Uploading Your Vaccination Proof to VeriFLY
You may want to see also
Frequently asked questions
In the 1970s, Armenians were typically vaccinated for TB in public health clinics, hospitals, and schools as part of the Soviet Union's widespread tuberculosis prevention program.
The Bacille Calmette-Guérin (BCG) vaccine was the primary TB vaccine administered to Armenians during the 1970s, as it was the standard vaccine used across the Soviet Union.
Yes, TB vaccinations were mandatory for Armenians in the 1970s as part of the Soviet Union's public health policies aimed at controlling the spread of tuberculosis.