The pertussis vaccine, designed to protect against whooping cough, was first introduced in the 1940s as part of the whole-cell pertussis (wP) vaccine. This early formulation was combined with diphtheria and tetanus toxoids to create the DTP vaccine, which became widely administered to children in the United States and other countries. However, due to concerns about side effects associated with the whole-cell vaccine, an acellular pertussis (aP) vaccine was developed in the 1980s and 1990s, leading to the introduction of the DTaP vaccine for children and Tdap for adolescents and adults. By the mid-1990s, the aP vaccine had largely replaced the wP vaccine in many countries, marking a significant evolution in pertussis immunization efforts.
| Characteristics | Values |
|---|---|
| First Pertussis Vaccine Developed | 1914 (Whole-cell Pertussis Vaccine, but not widely used initially) |
| Introduction of DTP Vaccine | 1948 (Combined Diphtheria, Tetanus, and Pertussis vaccine introduced) |
| Widespread Use in the U.S. | 1940s-1950s (Routine childhood immunization programs began) |
| Acellular Pertussis Vaccine (DTaP) | 1991 (Safer acellular version introduced in the U.S.) |
| Global Adoption | 1980s-1990s (Widespread adoption in many countries) |
| Current Recommendations | Routine vaccination for infants and children, with boosters for teens and adults (Tdap) |
| WHO Endorsement | Included in the WHO's Expanded Programme on Immunization (EPI) since 1974 |
| Impact on Disease | Significant reduction in pertussis cases globally since widespread use |
Explore related products






What You'll Learn
- First Pertussis Vaccine Development: Developed in the 1920s, early pertussis vaccines were whole-cell formulations
- Introduction in the US: Routine pertussis vaccination began in the United States in the 1940s
- Combination Vaccines: DTP (diphtheria, tetanus, pertussis) vaccine introduced in the 1940s for widespread use
- Acellular Vaccine Shift: Safer acellular pertussis vaccines replaced whole-cell versions in the 1990s
- Global Adoption Timeline: Pertussis vaccination expanded globally in the mid-20th century, varying by country
![]()
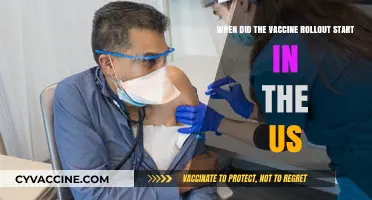
First Pertussis Vaccine Development: Developed in the 1920s, early pertussis vaccines were whole-cell formulations
The first pertussis vaccines, developed in the 1920s, marked a pivotal moment in the fight against whooping cough, a highly contagious respiratory disease that had ravaged populations, particularly young children. These early vaccines were whole-cell formulations, meaning they contained entire killed Bordetella pertussis bacteria. This approach aimed to stimulate the immune system by exposing it to the full array of bacterial components, triggering a broad immune response. While groundbreaking, these vaccines were not without challenges. Their efficacy varied, and side effects such as fever, pain at the injection site, and, in rare cases, more severe reactions, were reported. Despite these limitations, whole-cell pertussis vaccines represented a significant step forward, reducing mortality and morbidity rates dramatically in the decades that followed.
Administering these early vaccines typically began in infancy, with the first dose given at 2 months of age, followed by additional doses at 4 and 6 months. A booster was often recommended between 12 and 18 months to ensure sustained immunity. The dosage for infants and young children was carefully calibrated to balance efficacy and safety, usually ranging from 10 to 20 micrograms of pertussis antigen per dose. Parents were advised to monitor their children for common side effects and consult healthcare providers if symptoms persisted or worsened. This vaccination schedule laid the foundation for modern immunization practices, emphasizing the importance of early and consistent protection against pertussis.
The development of whole-cell pertussis vaccines was a testament to the scientific community’s determination to combat infectious diseases. Researchers like Jules Bordet and Octave Gengou, who isolated the pertussis bacterium in 1906, paved the way for vaccine development. By the 1930s, large-scale trials demonstrated the vaccine’s effectiveness, leading to its widespread adoption. However, the whole-cell formulation’s side effects spurred ongoing research into safer alternatives, eventually leading to the creation of acellular pertussis vaccines in the 1980s and 1990s. This evolution highlights the iterative nature of medical advancements, where early innovations serve as stepping stones for future improvements.
Practical considerations for administering whole-cell pertussis vaccines included proper storage and handling to maintain vaccine efficacy. Healthcare providers were trained to use sterile techniques during injection and to educate parents about the vaccine’s benefits and potential risks. Public health campaigns played a crucial role in promoting vaccination, addressing hesitancy, and ensuring high uptake rates. For families, understanding the vaccine’s importance and adhering to the recommended schedule were key to protecting vulnerable populations, particularly infants too young to be vaccinated. This collaborative effort between scientists, healthcare providers, and communities underscored the vaccine’s impact on public health.
In retrospect, the introduction of whole-cell pertussis vaccines in the 1920s was a turning point in disease prevention, saving countless lives and reducing the burden of whooping cough globally. While newer acellular vaccines have largely replaced whole-cell formulations due to their improved safety profile, the early vaccines remain a critical chapter in medical history. They demonstrated the power of immunization and set the stage for ongoing innovations in vaccine technology. For those interested in the history of vaccines or public health, studying the development and administration of the first pertussis vaccines offers valuable insights into the challenges and triumphs of scientific progress.
Synthetic Vaccine Production: Yeast Cells' Role in Lab-Made Immunization
You may want to see also
Explore related products






![]()
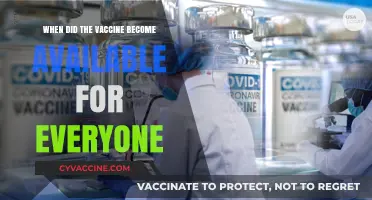
Introduction in the US: Routine pertussis vaccination began in the United States in the 1940s
The 1940s marked a pivotal shift in public health with the introduction of routine pertussis vaccination in the United States. Before this, whooping cough was a pervasive and often deadly threat, particularly to infants and young children. The development of the whole-cell pertussis vaccine, combined with diphtheria and tetanus toxoids (the DTP vaccine), offered the first line of defense against this highly contagious respiratory disease. This era laid the foundation for what would become a cornerstone of childhood immunization schedules, drastically reducing the incidence of pertussis nationwide.
Analyzing the rollout of the pertussis vaccine in the 1940s reveals both its successes and challenges. Initially, the vaccine was administered in a series of three doses, typically starting at 2 months of age, followed by boosters at 4 and 6 months. This schedule aimed to build immunity during the period when children were most vulnerable. However, the whole-cell vaccine was not without drawbacks; it often caused mild to moderate side effects, such as fever, soreness, and irritability, which led to hesitancy among some parents. Despite these concerns, the vaccine’s effectiveness in preventing severe disease and death outweighed its risks, cementing its place in routine pediatric care.
From a practical standpoint, the introduction of the pertussis vaccine in the 1940s required significant public health infrastructure. Clinics and schools became key sites for vaccination campaigns, and healthcare providers were trained to administer the vaccine safely. Parents were educated on the importance of completing the full series to ensure lasting immunity. This period also highlighted the need for ongoing research, as scientists began to explore ways to improve the vaccine’s safety and efficacy, setting the stage for future advancements like the acellular pertussis vaccine.
Comparatively, the 1940s pertussis vaccine rollout serves as a historical benchmark for modern immunization efforts. While today’s vaccines are more refined and have fewer side effects, the early program demonstrated the power of widespread vaccination in controlling infectious diseases. It also underscored the importance of public trust and clear communication, lessons that remain relevant in addressing vaccine hesitancy today. The legacy of the 1940s pertussis vaccine is a testament to the enduring impact of early public health interventions.
In conclusion, the introduction of routine pertussis vaccination in the United States during the 1940s was a transformative moment in the fight against whooping cough. It not only saved countless lives but also established a model for future vaccination programs. For parents today, understanding this history reinforces the value of timely immunizations and the role they play in protecting both individual children and the broader community. The story of the pertussis vaccine is a reminder that progress in public health often begins with bold, evidence-based action.
Did Fetal Cells End Polio? Salk's Vaccine Legacy
You may want to see also
Explore related products






![]()
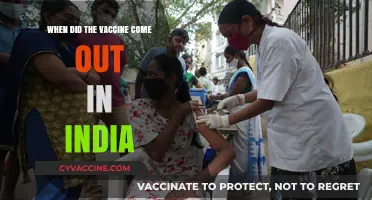
Combination Vaccines: DTP (diphtheria, tetanus, pertussis) vaccine introduced in the 1940s for widespread use
The DTP vaccine, a groundbreaking combination of diphtheria, tetanus, and pertussis antigens, emerged in the 1940s as a cornerstone of pediatric immunization. This innovation marked a pivotal shift from single-disease vaccines to a multi-pronged approach, streamlining administration and boosting compliance. Prior to its introduction, parents faced the logistical challenge of scheduling separate shots for each disease, often leading to incomplete immunization. The DTP vaccine addressed this by consolidating protection into a single series, typically administered at 2, 4, 6, and 15–18 months of age, with a booster at 4–6 years. This regimen not only simplified the process but also ensured children received timely protection against three potentially fatal diseases.
From an analytical perspective, the DTP vaccine’s success lies in its ability to maximize efficiency without compromising efficacy. Each component—diphtheria toxoid, tetanus toxoid, and inactivated pertussis bacteria—was carefully calibrated to elicit a robust immune response. For instance, the pertussis component, derived from whole-cell bacteria, provided broad immunity despite occasional side effects like fever or irritability. While later iterations (e.g., DTaP with acellular pertussis) reduced adverse reactions, the original DTP vaccine’s impact on disease reduction was undeniable. Diphtheria cases in the U.S. plummeted from 200,000 annually in the 1920s to fewer than 10 by the year 2000, a testament to its effectiveness.
Instructively, administering the DTP vaccine required adherence to strict protocols to ensure safety and potency. Healthcare providers were trained to store vials at 2–8°C, avoiding freezing, and to administer the 0.5 mL dose intramuscularly, typically in the deltoid or thigh muscle depending on the child’s age. Parents were advised to monitor for common reactions, such as soreness at the injection site or mild fever, and to seek medical attention for severe symptoms like persistent crying or seizures. These guidelines, though basic by today’s standards, were critical in building public trust and minimizing risks during the vaccine’s early years.
Persuasively, the DTP vaccine’s introduction in the 1940s was not just a medical achievement but a societal one. By bundling three vaccines into one, it democratized access to life-saving prevention, particularly in resource-limited settings. Its widespread adoption underscored the power of combination vaccines to address multiple public health threats simultaneously. Critics of early formulations often pointed to side effects, but the alternative—uncontrolled outbreaks of diphtheria, tetanus, and pertussis—was far more devastating. The DTP vaccine’s legacy endures in modern formulations like DTaP and Tdap, which build on its foundation while addressing safety concerns.
Comparatively, the DTP vaccine’s rollout in the 1940s contrasts sharply with today’s vaccine landscape, characterized by mRNA technology and global distribution networks. Yet, its core principle—combining antigens for efficiency and compliance—remains a gold standard. While newer vaccines offer improved safety profiles, the DTP vaccine’s impact on disease eradication cannot be overstated. It paved the way for combination vaccines like MMR (measles, mumps, rubella) and Pentavalent vaccines, proving that innovation in immunization often lies in consolidation rather than isolation. For historians and healthcare providers alike, the DTP vaccine serves as a reminder of how bold, practical solutions can transform public health.
Israel's Vaccination Success: Current Percentage and Global Impact
You may want to see also
Explore related products


![]()
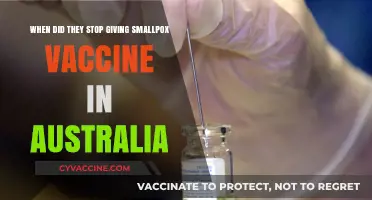
Acellular Vaccine Shift: Safer acellular pertussis vaccines replaced whole-cell versions in the 1990s
The pertussis vaccine has undergone significant transformations since its inception, with one of the most pivotal changes occurring in the 1990s. This era marked the transition from whole-cell pertussis vaccines to acellular versions, a shift driven by the need for safer immunization options. Whole-cell vaccines, introduced in the 1940s, effectively reduced pertussis cases but were associated with side effects such as fever, irritability, and, in rare instances, more severe reactions like seizures. These concerns prompted researchers to develop acellular pertussis (DTaP) vaccines, which contain purified components of the *Bordetella pertussis* bacterium, minimizing adverse reactions while maintaining efficacy.
From an analytical perspective, the acellular vaccine shift exemplifies how medical advancements prioritize both safety and public trust. Acellular vaccines reduced the incidence of mild to moderate side effects by up to 50% compared to their whole-cell predecessors. For instance, fever rates dropped from 20-30% in whole-cell recipients to 5-10% in those receiving the acellular version. This improvement was particularly crucial for parents hesitant to vaccinate their children due to fear of side effects. The transition also maintained high efficacy, with studies showing that DTaP provided 80-85% protection against pertussis in the first year after completion of the primary series, typically administered at 2, 4, and 6 months of age, followed by booster doses at 15-18 months and 4-6 years.
Instructively, the shift to acellular vaccines also necessitated changes in vaccination protocols. Healthcare providers had to educate parents about the new vaccine’s benefits and potential side effects, which were generally milder but still included soreness at the injection site and low-grade fever. The dosage remained consistent, with each dose containing 20-25 µg of pertussis toxin and 2-3 µg of filamentous hemagglutinin, key antigens in the acellular formulation. Parents were advised to monitor their children for 24-48 hours post-vaccination and administer acetaminophen if fever or discomfort occurred, though this was far less common than with whole-cell vaccines.
Persuasively, the acellular vaccine shift underscores the importance of continuous improvement in public health interventions. By addressing safety concerns, health authorities not only enhanced vaccine acceptance but also sustained high immunization rates, critical for herd immunity. For example, in the United States, pertussis cases declined dramatically after the introduction of whole-cell vaccines in the mid-20th century, but the transition to acellular versions in the 1990s helped maintain this progress while reducing vaccine-related hesitancy. This balance between efficacy and safety remains a cornerstone of modern vaccination strategies, ensuring that pertussis remains a preventable disease rather than a recurring threat.
Comparatively, the acellular vaccine shift highlights the evolution of vaccine technology and its impact on global health. While whole-cell vaccines were a groundbreaking achievement in their time, acellular versions represent a refinement that aligns with contemporary expectations of medical interventions—minimizing risks without compromising outcomes. This progression mirrors advancements in other vaccines, such as the move from oral to inactivated polio vaccines, demonstrating how iterative improvements can transform public health landscapes. For parents and healthcare providers, understanding this history reinforces the value of evidence-based innovations in safeguarding communities against preventable diseases.
Pneumococcal Vaccine PPSV23: Indicated Patient Populations and Benefits
You may want to see also
![]()
Global Adoption Timeline: Pertussis vaccination expanded globally in the mid-20th century, varying by country
The global rollout of the pertussis vaccine in the mid-20th century was a pivotal moment in public health, yet its adoption varied widely across countries, influenced by factors like economic development, healthcare infrastructure, and political will. The first whole-cell pertussis vaccine was introduced in the 1940s, but its integration into national immunization programs occurred in waves. High-income countries like the United States and the United Kingdom began routine administration in the late 1940s and early 1950s, targeting infants starting at 2 months of age with a series of three doses. These early adopters saw dramatic declines in pertussis cases, setting a precedent for other nations.
Middle-income countries, such as Brazil and India, followed suit in the 1960s and 1970s, though their implementation was often slower and more fragmented. In Brazil, the vaccine was incorporated into the Expanded Program on Immunization (EPI) in 1973, administered in a 3-dose schedule at 2, 4, and 6 months of age. India, facing logistical challenges in its vast rural areas, began nationwide pertussis vaccination in the late 1970s, often combining it with diphtheria and tetanus (DTP) vaccines. These countries achieved significant reductions in pertussis mortality, though coverage remained uneven due to resource constraints.
Low-income countries faced the steepest barriers to adoption, with many not introducing the pertussis vaccine until the 1980s or even 1990s. In sub-Saharan Africa, for instance, the vaccine was often rolled out as part of broader initiatives like the World Health Organization’s EPI in the 1980s. However, cold chain requirements and limited healthcare access hindered consistent delivery. Even today, some regions struggle to achieve full coverage, with doses typically administered at 6, 10, and 14 weeks of age, following WHO guidelines.
The shift from whole-cell to acellular pertussis vaccines in the 1990s further complicated global timelines. Developed in response to safety concerns, acellular vaccines were first introduced in Japan in 1981 and later adopted in high-income countries like the U.S. and Europe in the 1990s. However, their higher cost delayed adoption in low- and middle-income countries, where whole-cell vaccines remain the standard. This disparity highlights the ongoing challenges in achieving equitable global immunization.
Practical tips for healthcare providers in regions still using whole-cell vaccines include ensuring proper storage at 2–8°C and administering doses intramuscularly. For acellular vaccines, providers should be aware of the 5-dose schedule (2, 4, 6, 15–18 months, and 4–6 years) in some countries, though this varies. Monitoring for adverse reactions, such as fever or local redness, is crucial regardless of the vaccine type. The global timeline of pertussis vaccination underscores the interplay of innovation, economics, and policy in shaping public health outcomes.
New Vaccine for Seniors Over 65: Benefits and Availability
You may want to see also
Frequently asked questions
The pertussis vaccine, initially developed as a whole-cell vaccine, became available in the 1940s.
Widespread administration of the pertussis vaccine in the United States began in the late 1940s, as part of the diphtheria, tetanus, and pertussis (DTP) combination vaccine.
The acellular pertussis vaccine (DTaP), which is less likely to cause side effects than the whole-cell version, was introduced in the United States in the mid-1990s.
The pertussis vaccine became part of routine childhood immunization schedules in the United States in the 1940s, with the DTP vaccine, and was updated to DTaP in the 1990s.
The Tdap booster vaccine, which includes protection against tetanus, diphtheria, and pertussis, became available in the United States in 2005 for adolescents and adults.