The COVID-19 vaccine rollout in the United States began on December 14, 2020, marking a pivotal moment in the nation's fight against the pandemic. The first doses of the Pfizer-BioNTech vaccine were administered to healthcare workers and long-term care facility residents, following the U.S. Food and Drug Administration's (FDA) emergency use authorization issued just days earlier. This initial phase prioritized high-risk populations, including frontline healthcare workers and the elderly, to mitigate the virus's most severe impacts. The rollout expanded rapidly in subsequent months, with Moderna's vaccine receiving emergency approval shortly after, and Johnson & Johnson's single-dose vaccine joining the effort in early 2021. This coordinated effort, led by Operation Warp Speed and later the Biden administration, aimed to distribute vaccines equitably and efficiently, ultimately paving the way for widespread immunity and a gradual return to normalcy.
| Characteristics | Values |
|---|---|
| Start Date of Vaccine Rollout | December 14, 2020 |
| First Vaccine Authorized | Pfizer-BioNTech COVID-19 Vaccine (Emergency Use Authorization by FDA) |
| First Vaccinations Administered | Healthcare workers and long-term care facility residents |
| Initial Daily Vaccination Rate | Approximately 1 million doses per day (early 2021) |
| Peak Daily Vaccination Rate | Over 3 million doses per day (April 2021) |
| Total Doses Administered (as of Oct 2023) | Over 670 million doses |
| Fully Vaccinated Population (as of Oct 2023) | Approximately 68% of the U.S. population |
| Booster Rollout Start | September 2021 |
| Vaccines Authorized in the U.S. | Pfizer, Moderna, Johnson & Johnson (J&J), Novavax |
| Current Vaccination Focus | Booster shots, pediatric vaccinations, and global distribution |
Explore related products






What You'll Learn
![]()
First COVID-19 vaccine administered in the U.S
The first COVID-19 vaccine administered in the U.S. marked a pivotal moment in the nation’s battle against the pandemic. On December 14, 2020, Sandra Lindsay, a critical care nurse in Queens, New York, received the Pfizer-BioNTech vaccine live on television. This event symbolized hope and resilience, as healthcare workers on the frontlines became the first to receive protection against the virus. The vaccine, administered in a two-dose regimen with a 21-day interval, required ultra-cold storage at -94°F, presenting logistical challenges that underscored the complexity of the rollout.
Analyzing the significance of this moment reveals a strategic prioritization of high-risk groups. The Centers for Disease Control and Prevention (CDC) recommended that healthcare workers and long-term care facility residents receive the vaccine first, given their heightened exposure and vulnerability. Sandra Lindsay’s vaccination was not just a medical procedure but a public statement of trust in science and a call to action for others to follow. Her willingness to be vaccinated publicly helped combat hesitancy and encouraged widespread acceptance of the vaccine.
From a practical standpoint, the rollout required meticulous planning. Vaccination sites had to adhere to strict protocols, including monitoring recipients for 15–30 minutes post-injection to detect rare allergic reactions. The Pfizer vaccine’s 95% efficacy rate, determined in clinical trials, offered robust protection, but its storage requirements limited accessibility in rural or under-resourced areas. Moderna’s vaccine, approved shortly after, provided a more flexible alternative with storage at standard freezer temperatures, broadening distribution possibilities.
Comparing the U.S. rollout to global efforts highlights both achievements and challenges. While the U.S. was among the first nations to administer vaccines, disparities in access emerged, particularly in underserved communities. Lessons from this phase emphasized the need for equitable distribution, clear communication, and community engagement. For individuals, staying informed about eligibility, scheduling appointments promptly, and following dosage instructions were critical steps in contributing to herd immunity.
In conclusion, the first COVID-19 vaccine administered in the U.S. was more than a medical milestone—it was a beacon of hope and a testament to scientific achievement. Sandra Lindsay’s vaccination set the stage for millions to follow, illustrating the power of collective action in overcoming a global crisis. As the rollout expanded, it became clear that success depended not just on the vaccine itself, but on the infrastructure, trust, and cooperation of the public. This moment remains a reminder of what can be achieved when science, policy, and humanity align.
US Vaccine Progress: How Close Are We to a Solution?
You may want to see also
Explore related products






![]()
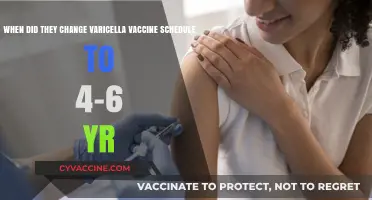
Initial priority groups for vaccination
The COVID-19 vaccine rollout in the United States began on December 14, 2020, with healthcare workers and long-term care facility residents receiving the first doses. This marked the beginning of a phased approach to vaccination, prioritizing those most at risk of severe illness and death. The initial priority groups were carefully selected based on data and recommendations from the Centers for Disease Control and Prevention (CDC) and the Advisory Committee on Immunization Practices (ACIP).
Phase 1a: Protecting the Most Vulnerable
The first phase, 1a, targeted healthcare personnel and residents of long-term care facilities. Healthcare workers, including doctors, nurses, and support staff, were prioritized due to their high risk of exposure and their critical role in maintaining the healthcare system. Long-term care facility residents, particularly those in nursing homes, were identified as one of the most vulnerable populations, accounting for a disproportionate number of COVID-19 deaths. This phase ensured that those on the frontlines and those most likely to suffer severe outcomes were protected first. For example, a 90-year-old nursing home resident in New York became one of the first Americans to receive the Pfizer-BioNTech vaccine, symbolizing hope and urgency in the fight against the pandemic.
Phase 1b and 1c: Expanding Access Strategically
As vaccine supply increased, Phase 1b expanded to include frontline essential workers, such as teachers, grocery store employees, and emergency responders, alongside adults aged 75 and older. This phase recognized the broader societal impact of protecting essential workers while continuing to shield the elderly. Phase 1c further broadened eligibility to include individuals aged 65–74, those with high-risk medical conditions (e.g., cancer, heart disease, or diabetes), and other essential workers like transportation and food service employees. This tiered approach balanced ethical considerations with practical logistics, ensuring equitable distribution while maximizing public health impact.
Practical Tips for Priority Groups
For those in priority groups, staying informed was key. Local health departments and pharmacies often provided specific instructions, such as scheduling appointments through online portals or calling dedicated hotlines. For instance, some states required proof of employment for essential workers, while others prioritized individuals with specific medical conditions verified by a doctor’s note. Additionally, understanding the recommended dosage—typically two doses for Pfizer and Moderna, spaced 3–4 weeks apart—helped ensure full protection. Practical tips included dressing in loose clothing for easy access to the injection site and scheduling vaccinations at times when side effects (e.g., fatigue or mild fever) would cause minimal disruption.
Comparative Analysis: Balancing Speed and Equity
The U.S. approach to prioritizing groups differed from some countries, which focused solely on age-based rollouts. By including essential workers and high-risk individuals alongside the elderly, the U.S. aimed to reduce both mortality and community transmission. However, this strategy faced challenges, such as ensuring equitable access for marginalized communities and managing vaccine hesitancy among priority groups. For example, targeted outreach campaigns were necessary to address concerns among healthcare workers and minority populations. This comparative perspective highlights the complexity of balancing speed, fairness, and public trust in a historic vaccination effort.
Easy Steps to Register for Your Vaccine at H-E-B
You may want to see also
Explore related products






![]()
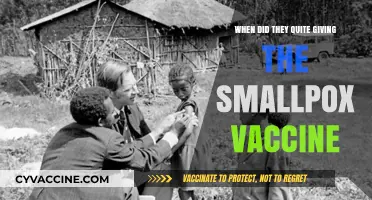
Timeline of vaccine approvals (Pfizer, Moderna, etc.)
The first COVID-19 vaccine in the U.S. was administered on December 14, 2020, just days after the Pfizer-BioNTech vaccine received emergency use authorization (EUA) from the FDA. This marked the beginning of a phased rollout that prioritized healthcare workers and long-term care facility residents, groups deemed most vulnerable to severe illness. The Pfizer vaccine, requiring two doses administered 21 days apart, was the first to be approved for individuals aged 16 and older. Its rapid development and authorization were a testament to unprecedented global collaboration and scientific innovation, setting the stage for subsequent vaccine approvals.
Moderna’s mRNA-1273 vaccine followed closely behind, receiving EUA on December 18, 2020. Like Pfizer’s, Moderna’s vaccine required two doses, but with a longer interval of 28 days between shots. It was initially approved for individuals aged 18 and older, offering another critical tool in the fight against the pandemic. Both Pfizer and Moderna vaccines demonstrated high efficacy rates—around 94-95%—in preventing symptomatic COVID-19, providing hope for a path out of the crisis. Their mRNA technology, though novel, proved safe and effective, paving the way for broader public confidence in vaccination efforts.
Johnson & Johnson’s single-dose viral vector vaccine received EUA on February 27, 2021, offering a simpler administration process and easier storage requirements compared to the mRNA vaccines. Approved for individuals aged 18 and older, it provided flexibility for populations with limited access to healthcare or those hesitant about a two-dose regimen. However, its rollout was temporarily paused in April 2021 due to rare but serious blood clot concerns, highlighting the importance of ongoing safety monitoring. Despite this setback, it resumed distribution with updated guidelines, playing a vital role in reaching underserved communities.
Vaccine approvals expanded to younger age groups as clinical trials progressed. In May 2021, Pfizer’s vaccine was authorized for adolescents aged 12-15, followed by approval for children aged 5-11 in October 2021. Moderna’s vaccine was later authorized for adolescents aged 12-17 in June 2022. These expansions were critical in protecting school-aged children and reducing community transmission. Dosage adjustments were made for younger age groups, with Pfizer administering a lower dose (10 micrograms for 5-11-year-olds vs. 30 micrograms for older individuals) to balance efficacy and safety.
Booster shots became a key component of the vaccine timeline as concerns about waning immunity and emerging variants arose. In September 2021, the FDA authorized Pfizer booster doses for certain high-risk groups, followed by broader eligibility for all adults in November. Moderna boosters were approved shortly after, with half the dose of the initial series (50 micrograms). Johnson & Johnson recipients were advised to receive a booster dose two months after their initial shot. These recommendations evolved as data on variant-specific boosters, such as those targeting Omicron, became available, underscoring the dynamic nature of vaccine strategy in response to the pandemic’s challenges.
Essential Puppy Vaccination Schedule: A Complete Guide for New Owners
You may want to see also
Explore related products






![]()
State-by-state rollout variations and challenges
The COVID-19 vaccine rollout in the United States began in December 2020, but the pace and approach varied significantly across states. While the federal government provided guidelines, individual states had considerable autonomy in determining distribution strategies, eligibility criteria, and logistical execution. This decentralization led to a patchwork of rollout timelines and challenges, reflecting each state’s unique demographics, infrastructure, and political priorities.
Consider the example of New York and Florida, two states with contrasting approaches. New York initially prioritized healthcare workers and nursing home residents, aligning closely with CDC recommendations. However, the state faced early challenges with vaccine supply shortages and a cumbersome appointment system, leaving many eligible residents frustrated. In contrast, Florida focused on vaccinating seniors aged 65 and older from the outset, a decision driven by its large elderly population. While this strategy protected a vulnerable group, it sparked criticism for excluding essential workers in younger age brackets. These variations highlight how state-specific decisions directly impacted access and equity.
Logistical challenges further exacerbated these differences. States like Alaska and West Virginia faced unique hurdles due to their rural populations and limited healthcare infrastructure. Alaska relied on partnerships with tribal health organizations to distribute vaccines to remote communities, while West Virginia’s early success was attributed to its use of local pharmacies and a centralized registration system. Meanwhile, densely populated states like California struggled with scaling distribution to millions of residents, leading to long lines and confusion over eligibility. Such disparities underscore the importance of tailoring rollout strategies to local contexts.
Another critical factor was political influence. Some states, like Texas, emphasized personal choice and resisted mandates, which impacted public trust and uptake rates. Others, like Massachusetts, implemented stricter eligibility phases and invested heavily in public education campaigns, resulting in higher vaccination rates among eligible populations. These political differences not only affected rollout speed but also shaped public perception of the vaccine, creating a divide in community engagement and compliance.
Practical tips for navigating these variations include staying informed about your state’s specific eligibility criteria and registration process, often found on local health department websites. For those in rural areas, inquiring about mobile vaccination clinics or partnering pharmacies can improve access. Additionally, leveraging community organizations and local leaders can help address misinformation and encourage vaccine confidence. Understanding these state-by-state nuances is essential for individuals and policymakers alike to ensure a more equitable and efficient rollout.
Jenny McCarthy's Vaccine Views: A Change of Heart?
You may want to see also
Explore related products





![]()
Impact of Operation Warp Speed on distribution
The COVID-19 vaccine rollout in the United States began on December 14, 2020, with healthcare workers and long-term care facility residents receiving the first doses. This rapid deployment was largely due to Operation Warp Speed (OWS), a public-private partnership launched in May 2020 to accelerate vaccine development and distribution. OWS invested $18 billion in vaccine candidates, manufacturing, and logistics, ensuring that doses were ready for distribution as soon as emergency use authorization was granted. Without this initiative, the timeline for vaccine availability could have extended well into 2021, delaying the nation’s path to immunity.
One of the most significant impacts of Operation Warp Speed was its ability to compress the typical vaccine development timeline from years to months without compromising safety. For instance, Pfizer-BioNTech and Moderna’s mRNA vaccines, which typically take a decade to develop, were authorized within a year. This was achieved by running clinical trials concurrently, scaling up manufacturing in advance of approval, and streamlining regulatory processes. By December 2020, OWS had secured 100 million doses of Pfizer’s vaccine and 200 million doses of Moderna’s, ensuring immediate availability for priority groups. This proactive approach allowed the U.S. to administer over 20 million doses by early January 2021, a pace unmatched by most other countries.
However, the success of OWS in development did not immediately translate to seamless distribution. Initial rollout faced challenges such as limited supply, logistical bottlenecks, and confusion over prioritization. States struggled with allocating doses to hospitals, pharmacies, and community centers, often leading to unused vials and inequitable access. For example, the Pfizer vaccine required ultra-cold storage (-70°C), complicating distribution to rural areas. Moderna’s vaccine, stored at -20°C, was more accessible but still faced supply chain hurdles. OWS’s focus on development meant that distribution planning received less attention, highlighting the need for a balanced approach in future public health initiatives.
Despite these challenges, OWS laid the groundwork for a distribution system that scaled rapidly in early 2021. By March, the U.S. was administering over 3 million doses daily, thanks to partnerships with pharmacies like CVS and Walgreens, mass vaccination sites, and mobile clinics. The initiative’s funding also supported the development of easy-to-use tools like the CDC’s Vaccine Administration Management System (VAMS), which streamlined scheduling and tracking. By May 2021, eligibility expanded to all adults, and by July, over 50% of the U.S. population was fully vaccinated. OWS’s legacy is evident in the infrastructure it created, which continues to support vaccination campaigns, including booster shots and pediatric doses for children aged 5 and older.
In retrospect, Operation Warp Speed’s impact on vaccine distribution was a double-edged sword. While its focus on development ensured doses were available sooner than expected, inadequate planning for distribution led to early inefficiencies. Practical tips for future initiatives include integrating distribution planning from the outset, investing in local healthcare infrastructure, and ensuring clear communication between federal and state authorities. OWS demonstrated that speed in development is only as valuable as the system’s ability to deliver doses effectively. Its lessons will shape how the U.S. responds to future pandemics, emphasizing the need for a holistic approach to vaccine deployment.
Is the Coronavirus Vaccine a One-Time Shot? What You Need to Know
You may want to see also
Frequently asked questions
The COVID-19 vaccine rollout in the United States officially began on December 14, 2020, with the first doses of the Pfizer-BioNTech vaccine administered to healthcare workers and long-term care facility residents.
The Pfizer-BioNTech COVID-19 vaccine was the first to receive emergency use authorization (EUA) from the FDA on December 11, 2020, and was the first to be distributed starting December 14, 2020.
The Moderna vaccine received EUA on December 18, 2020, and distribution began shortly after. The Johnson & Johnson (Janssen) vaccine received EUA on February 27, 2021, and its rollout started in early March 2021.






![Pandemic Pandemic [DVD]](https://m.media-amazon.com/images/I/81dZDU9gUpL._AC_UL320_.jpg)
![Pandemic [DVD]](https://m.media-amazon.com/images/I/51vChb09XaL._AC_UL320_.jpg)
![Pandemic [DVD]](https://m.media-amazon.com/images/I/81G1z+AOoNL._AC_UL320_.jpg)

![PANDEMIC [Blu-ray]](https://m.media-amazon.com/images/I/71xlZkgPU4L._AC_UL320_.jpg)