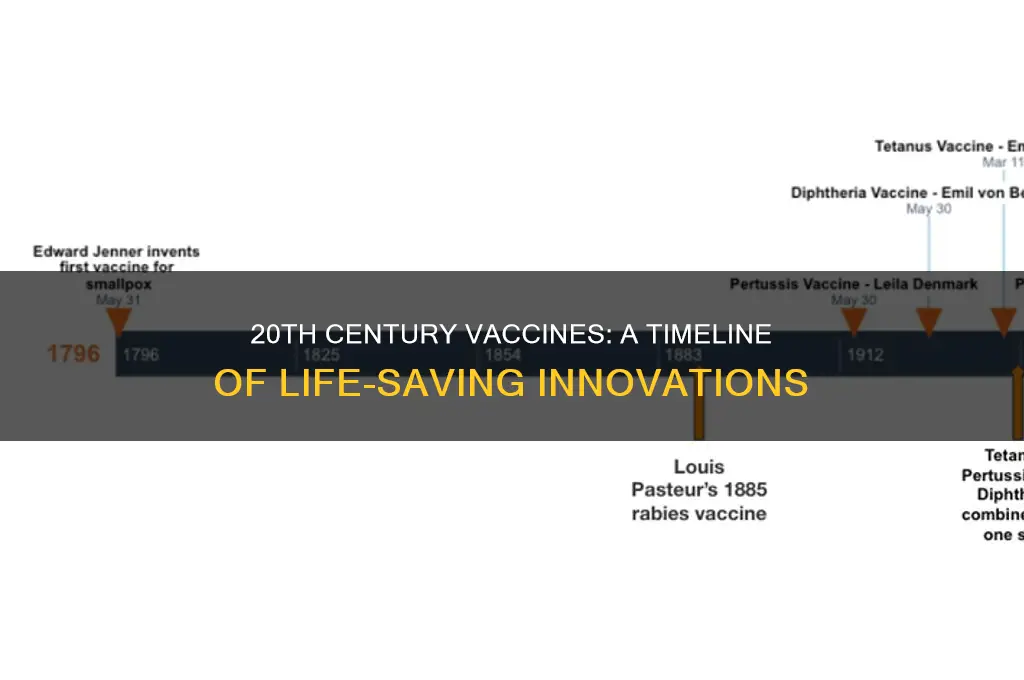
The 20th century marked a transformative era in medical history, witnessing the development of numerous vaccines that revolutionized public health and saved millions of lives. Among the most notable were the vaccines for diphtheria, tetanus, and pertussis (DTaP), which were combined into a single shot in the 1940s, followed by the creation of the polio vaccine in the 1950s, effectively eradicating a once-feared disease. The measles vaccine emerged in 1963, drastically reducing global cases, while the mumps and rubella vaccines followed in the late 1960s, leading to the widespread use of the MMR vaccine. Additionally, the hepatitis B vaccine in the 1980s and the varicella (chickenpox) vaccine in the 1990s further expanded the arsenal of preventive measures. These advancements not only controlled infectious diseases but also laid the foundation for modern vaccinology, shaping the course of global health in the 21st century.
Explore related products






What You'll Learn
- Smallpox Vaccine (1960s-1970s): Global eradication achieved through widespread vaccination campaigns
- Polio Vaccine (1955): Salk’s inactivated vaccine and Sabin’s oral vaccine reduced cases drastically
- Measles Vaccine (1963): Prevented millions of deaths and complications annually worldwide
- Mumps Vaccine (1967): Included in MMR vaccine, significantly lowered mumps-related complications
- Rubella Vaccine (1969): Prevented congenital rubella syndrome, protecting unborn children from severe defects
![]()
Smallpox Vaccine (1960s-1970s): Global eradication achieved through widespread vaccination campaigns
The smallpox vaccine stands as a monumental achievement in medical history, marking the first and only time a human disease has been completely eradicated through vaccination. Developed in the late 18th century by Edward Jenner, the vaccine’s true global impact came in the 20th century, particularly during the 1960s and 1970s, when the World Health Organization (WHO) launched an intensive campaign to eliminate smallpox worldwide. This effort relied on a lyophilized (freeze-dried) vaccine that was stable in tropical climates, administered via a bifurcated needle to create a localized skin lesion, ensuring effective immunization with minimal vaccine usage.
The strategy behind the smallpox eradication campaign was twofold: surveillance and containment. Teams of health workers systematically identified cases, isolated patients, and vaccinated everyone in the surrounding area to prevent further spread. This method, known as “ring vaccination,” proved highly effective in breaking the chain of transmission. The vaccine itself required a single dose for adults and children over one year of age, with a booster recommended after 3–5 years for continued immunity. Notably, the vaccine was contraindicated for pregnant women, individuals with compromised immune systems, and those with certain skin conditions, highlighting the need for careful screening during mass vaccination drives.
One of the most striking aspects of the smallpox campaign was its global coordination. Over 80% of the world’s population was vaccinated, with a focus on high-risk regions like Africa and Asia. The cost-effectiveness of the vaccine—estimated at just $0.30 per dose—made it accessible even in resource-limited settings. By 1977, the last natural case of smallpox was recorded in Somalia, and in 1980, the WHO officially declared smallpox eradicated. This success demonstrated the power of international collaboration and the critical role of vaccines in public health.
Comparing the smallpox vaccine to modern vaccination efforts reveals both similarities and lessons. Unlike today’s vaccines, which often require multiple doses and sophisticated storage, the smallpox vaccine’s simplicity and durability were key to its success. However, the campaign’s reliance on meticulous surveillance and community engagement underscores principles still relevant in combating diseases like polio or COVID-19. The smallpox story serves as a reminder that eradication is possible—but only with unwavering commitment, strategic planning, and equitable access to vaccines.
For those studying public health or involved in vaccination programs, the smallpox eradication campaign offers practical takeaways. First, prioritize community trust; local leaders and health workers were instrumental in overcoming skepticism and ensuring participation. Second, adapt strategies to local contexts; the bifurcated needle, for instance, was chosen for its ease of use in remote areas. Finally, maintain vigilance even after success; the WHO continues to monitor for potential smallpox reemergence, a cautionary tale for ongoing vaccine-preventable diseases. The smallpox vaccine’s legacy is not just in its eradication but in the blueprint it provides for future global health victories.
Are Truck Drivers Required to Get Vaccinated? Legal Insights
You may want to see also
Explore related products






![]()
Polio Vaccine (1955): Salk’s inactivated vaccine and Sabin’s oral vaccine reduced cases drastically
The 20th century witnessed a revolution in vaccine development, with numerous life-saving immunizations introduced to combat deadly diseases. Among these, the polio vaccine stands out as a landmark achievement, marking a turning point in the battle against a crippling and often fatal illness. In 1955, Jonas Salk's inactivated polio vaccine (IPV) was licensed for use, followed by Albert Sabin's oral polio vaccine (OPV) in the early 1960s. These two vaccines, developed through distinct approaches, played a pivotal role in drastically reducing polio cases worldwide.
Salk's IPV, administered through injection, contains inactivated (killed) poliovirus, making it impossible for the virus to cause disease. The recommended schedule for IPV typically involves a series of doses, starting at 2 months of age, followed by additional doses at 4 months, 6-18 months, and a booster shot at 4-6 years. This vaccine is particularly effective in inducing humoral immunity, providing protection against all three poliovirus types. However, it does not induce mucosal immunity, which is crucial for preventing viral transmission. This limitation paved the way for Sabin's OPV, a live-attenuated vaccine administered orally, often on a sugar cube or in liquid form.
The oral polio vaccine, developed by Sabin, revolutionized polio prevention by inducing both humoral and mucosal immunity. This dual protection not only safeguards individuals from developing paralytic polio but also reduces viral transmission, contributing to herd immunity. OPV is typically administered in multiple doses, starting at 6 weeks of age, followed by additional doses at 10-12 weeks, 14-16 weeks, and a booster at 12-23 months. The ease of administration and low cost made OPV the preferred choice for mass vaccination campaigns, particularly in developing countries. However, the use of OPV is associated with a rare risk of vaccine-associated paralytic polio (VAPP), occurring in approximately 1 in 2.7 million birth doses.
A comparative analysis of IPV and OPV highlights their complementary roles in polio eradication. While IPV provides individual protection without the risk of VAPP, OPV offers the added benefit of reducing viral transmission. In recent years, many countries have adopted a sequential vaccination schedule, utilizing both vaccines to maximize immunity and minimize risks. This approach, known as the "IPV-OPV switch," involves administering IPV in the initial doses to reduce the risk of VAPP, followed by OPV to boost mucosal immunity. Practical tips for healthcare providers include ensuring proper storage and handling of vaccines, maintaining a consistent vaccination schedule, and educating caregivers about the importance of completing the full vaccine series.
The impact of Salk's and Sabin's vaccines on global polio incidence is nothing short of remarkable. In the United States, annual polio cases plummeted from over 57,000 in 1952 to fewer than 100 in 1965. Globally, the number of polio cases has decreased by over 99% since 1988, from an estimated 350,000 cases to a few hundred cases in 2023. This dramatic reduction is a testament to the power of vaccination and the tireless efforts of healthcare workers, researchers, and public health officials. As we continue to strive for polio eradication, the lessons learned from the development and deployment of these vaccines serve as a guiding light, informing strategies for tackling other vaccine-preventable diseases.
Ebola Vaccine for Swine: Current Research and Developments Explained
You may want to see also
Explore related products





![]()
Measles Vaccine (1963): Prevented millions of deaths and complications annually worldwide
The measles vaccine, introduced in 1963, stands as a monumental achievement in 20th-century medicine, transforming a once-common childhood illness into a preventable disease. Before its development, measles infected millions annually, causing severe complications like pneumonia, encephalitis, and blindness, and claiming the lives of approximately 2.6 million people each year, mostly children under five. The vaccine’s impact was immediate and profound, reducing global measles deaths by 73% between 2000 and 2018 alone. This single intervention exemplifies how scientific innovation can reshape public health on a global scale.
Administered typically as part of the MMR (measles, mumps, rubella) vaccine, the measles vaccine is given in two doses: the first at 12–15 months of age and the second at 4–6 years. This schedule ensures robust immunity, with over 97% of recipients becoming protected after the second dose. The vaccine’s efficacy is not just theoretical; it has prevented an estimated 23.2 million deaths between 2000 and 2018, making it one of the most cost-effective health interventions ever developed. For parents, adherence to the recommended schedule is critical, as delays can leave children vulnerable during outbreaks.
Despite its success, the measles vaccine faces challenges, particularly in regions with low vaccination rates or vaccine hesitancy. Outbreaks still occur, often fueled by misinformation or limited access to healthcare. For instance, in 2019, the World Health Organization reported nearly 10 million measles cases worldwide, a stark reminder of the disease’s persistence. Travelers to endemic areas are advised to ensure their vaccinations are up to date, as measles remains prevalent in parts of Africa and Asia. Public health campaigns emphasizing the vaccine’s safety and efficacy are essential to countering myths and maintaining herd immunity.
The measles vaccine’s legacy extends beyond its direct impact on the disease. It has served as a model for vaccine development, demonstrating the power of immunization to eradicate infectious threats. Its success underscores the importance of global collaboration in vaccine distribution and the need for sustained investment in public health infrastructure. As new diseases emerge, the measles vaccine reminds us that prevention through vaccination remains one of humanity’s most effective tools for safeguarding lives.
Understanding the Anthrax Vaccine: Type, Composition, and Protection
You may want to see also
Explore related products






![]()
Mumps Vaccine (1967): Included in MMR vaccine, significantly lowered mumps-related complications
The mumps vaccine, introduced in 1967, marked a turning point in the battle against a once-common childhood illness. Prior to its development, mumps outbreaks were frequent, affecting millions annually and leading to complications such as deafness, meningitis, and orchitis. By integrating the mumps vaccine into the MMR (Measles, Mumps, Rubella) combination vaccine in 1971, public health officials streamlined immunization efforts, ensuring broader protection with fewer injections. This strategic inclusion not only simplified vaccination schedules but also significantly reduced the incidence of mumps and its associated complications, showcasing the power of vaccine innovation and consolidation.
Administering the MMR vaccine typically begins with the first dose at 12–15 months of age, followed by a second dose at 4–6 years. This two-dose regimen provides over 90% efficacy against mumps, offering long-term immunity for most recipients. For adults born before 1957 who may lack natural immunity, catching up with at least one dose is recommended, particularly for healthcare workers, students, and international travelers. The vaccine’s safety profile is well-established, with mild side effects like fever or rash being rare and transient.
Comparatively, the mumps vaccine’s impact stands out among 20th-century immunizations. While vaccines like polio and measles saved lives by preventing severe, often fatal diseases, the mumps vaccine primarily targeted quality-of-life improvements by averting complications such as infertility or neurological damage. This distinction highlights the evolving goals of vaccination—from survival to holistic well-being. The MMR’s success also underscores the value of combination vaccines in maximizing coverage while minimizing logistical challenges.
Practical tips for parents and caregivers include scheduling vaccinations during well-child visits to ensure timely administration and maintaining open communication with healthcare providers about any concerns. For those hesitant about vaccines, understanding the rigorous testing and monitoring processes can alleviate fears. Additionally, tracking local mumps outbreaks can reinforce the importance of staying up-to-date on immunizations. The mumps vaccine’s legacy is clear: by integrating it into the MMR, public health systems achieved a dual victory—simplifying vaccine delivery and dramatically reducing disease burden.
Incorrect Vaccine Administration: Risks of Missing the Muscle Injection
You may want to see also
Explore related products






![]()
Rubella Vaccine (1969): Prevented congenital rubella syndrome, protecting unborn children from severe defects
The rubella vaccine, introduced in 1969, stands as a pivotal achievement in 20th-century medicine, specifically for its role in preventing congenital rubella syndrome (CRS). Before its development, rubella, though mild in children and adults, posed a grave threat to unborn children if contracted by pregnant women. CRS could lead to severe birth defects, including deafness, blindness, heart defects, and developmental delays. The vaccine’s creation marked a turning point, offering a shield for both mothers and their unborn children. Administered typically as part of the MMR (measles, mumps, rubella) vaccine, it is recommended for children in two doses: the first at 12–15 months and the second at 4–6 years. For adults, especially women of childbearing age, ensuring immunity through vaccination or testing is critical to prevent CRS.
Analytically, the rubella vaccine’s impact is measurable in the near-eradication of CRS in countries with high vaccination rates. Prior to 1969, rubella epidemics caused tens of thousands of cases of CRS globally. By the 1980s, following widespread vaccination, CRS cases plummeted by over 95% in the United States alone. This success underscores the vaccine’s dual role: protecting individuals from rubella and safeguarding fetal development. However, its effectiveness relies on herd immunity, making vaccination rates a public health priority. A single dose of the rubella vaccine provides 95% immunity, while two doses increase protection to 97%, ensuring robust defense against the virus.
Instructively, ensuring rubella immunity is straightforward but requires proactive steps. Pregnant women should avoid the MMR vaccine, as it contains live attenuated viruses, but should verify immunity through blood tests early in pregnancy. Non-pregnant women and men can receive the vaccine at any time, though it’s advisable to wait 28 days after vaccination before conceiving. For travelers or those in outbreak-prone areas, immunity checks are essential. Practical tips include scheduling vaccinations during routine health visits and keeping immunization records updated. Schools and workplaces often require proof of MMR vaccination, making it a lifelong health investment.
Persuasively, the rubella vaccine is not just a medical triumph but a moral imperative. CRS is entirely preventable, yet outbreaks persist in regions with low vaccination rates. The vaccine’s safety and efficacy are well-documented, with rare side effects limited to mild fever or rash. Skepticism or misinformation about vaccines endangers not only individuals but also vulnerable populations, including unborn children. By prioritizing rubella vaccination, societies uphold the principle of protecting the most vulnerable. It’s a small step with monumental consequences, ensuring that no child suffers from preventable defects.
Comparatively, the rubella vaccine’s success contrasts with challenges faced by other 20th-century vaccines, such as polio or influenza, which require constant adaptation due to evolving viruses. Rubella’s stability as a virus has allowed the vaccine to remain highly effective without frequent updates. This consistency highlights the importance of targeting stable pathogens for long-term prevention. Unlike vaccines requiring annual boosters, the rubella vaccine offers lifelong immunity after two doses, simplifying public health strategies. Its development serves as a model for how vaccines can address specific, preventable harms with lasting impact.
Airports and Vaccination: What's the Connection?
You may want to see also
Frequently asked questions
In the early 20th century, key vaccines developed included the diphtheria antitoxin (1913) and the tetanus toxoid (1924), which laid the foundation for modern immunization.
The yellow fever vaccine (1937) was the first widely used vaccine for a viral disease, developed by Max Theiler and his team.
The polio vaccine was developed in the 1950s, with Jonas Salk creating the inactivated polio vaccine (IPV) in 1955 and Albert Sabin developing the oral polio vaccine (OPV) in 1961.
The measles vaccine was licensed in 1963, with the combined MMR vaccine (measles, mumps, rubella) introduced in 1971, significantly reducing global measles cases.
The hepatitis B vaccine was first approved in 1981, becoming the first vaccine to prevent a major human cancer (hepatocellular carcinoma) caused by chronic infection.