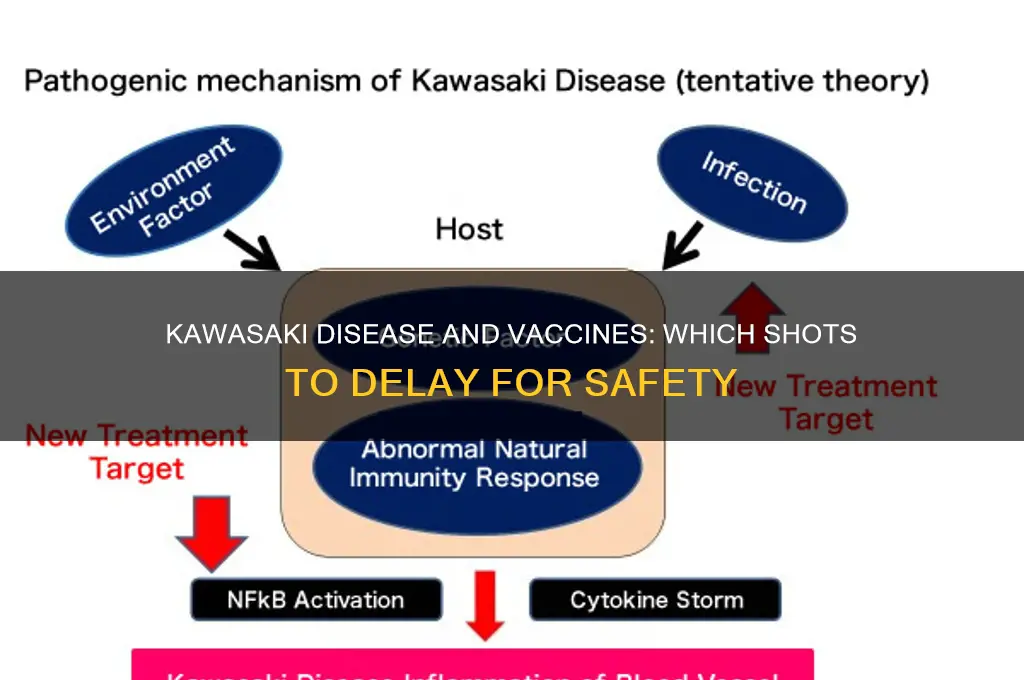
Kawasaki disease, an acute febrile illness primarily affecting children under five, is characterized by systemic inflammation of blood vessels, potentially leading to serious complications like coronary artery aneurysms. While vaccines are crucial for preventing infectious diseases, certain considerations arise when administering them to children with a history of Kawasaki disease, particularly during the acute phase or shortly after recovery. Vaccines that may stimulate the immune system excessively, such as live attenuated vaccines (e.g., MMR, varicella), or those containing adjuvants, could theoretically exacerbate inflammation or trigger a relapse. Therefore, healthcare providers must carefully evaluate the timing and type of vaccines for these patients, often delaying immunizations until the child is fully recovered and stable, while ensuring they remain protected against vaccine-preventable diseases.
Explore related products


$11.93 $21.99




What You'll Learn
![]()
MMR Vaccine Timing
Kawasaki disease, an acute febrile illness primarily affecting children under five, complicates vaccination schedules due to its potential to cause systemic inflammation and immune dysregulation. Among the vaccines requiring careful timing, the MMR (measles, mumps, rubella) vaccine stands out due to its live attenuated nature and the immune response it elicits. While MMR is generally safe, its administration in the context of Kawasaki disease demands a nuanced approach to avoid exacerbating immune-related risks.
Timing Considerations: The MMR vaccine is typically administered in two doses: the first at 12–15 months and the second at 4–6 years. However, in children with a history of Kawasaki disease, delaying the first dose until at least 6 months post-recovery is often recommended. This delay minimizes the risk of overlapping inflammatory responses, as Kawasaki disease can leave the immune system in a heightened state for several months. For children who experienced severe or prolonged Kawasaki disease, consulting an immunologist or infectious disease specialist is crucial to tailor the timing further.
Immune Status Evaluation: Before administering MMR, healthcare providers should assess the child’s immune status, including IgG and IgM levels, to ensure the immune system has stabilized. If the child received intravenous immunoglobulin (IVIG) as part of Kawasaki treatment, waiting at least 3 months post-IVIG is advised, as IVIG can transiently suppress vaccine efficacy. This precaution ensures the MMR vaccine elicits an adequate immune response without interference.
Practical Tips for Parents: If your child has had Kawasaki disease, maintain open communication with their pediatrician about vaccination timelines. Keep a detailed record of their recovery milestones, including treatments received and follow-up test results. Avoid scheduling MMR vaccination during periods of illness or immune stress, as this could further complicate the response. Additionally, monitor your child closely post-vaccination for any unusual symptoms, such as persistent fever or rash, and report them promptly.
Comparative Perspective: Unlike inactivated vaccines (e.g., DTaP or IPV), which are generally safe to administer on schedule, live vaccines like MMR require more cautious handling in Kawasaki disease cases. This distinction highlights the importance of vaccine type in decision-making. While delaying MMR may temporarily increase susceptibility to measles, mumps, or rubella, the risk of adverse reactions in a recovering immune system outweighs this concern, particularly in regions with high vaccination coverage and low disease prevalence.
In summary, MMR vaccine timing in Kawasaki disease patients hinges on balancing immune recovery with disease prevention. Delayed administration, immune status evaluation, and individualized planning are key to ensuring safety and efficacy. By approaching MMR vaccination with careful consideration, healthcare providers and parents can protect children from vaccine-preventable diseases without compromising their recovery from Kawasaki disease.
Is Fever Normal After Hepatitis B Vaccine? Understanding Side Effects
You may want to see also
Explore related products






![]()
Live Vaccines Risks
Live vaccines, such as the measles-mumps-rubella (MMR) and varicella (chickenpox) vaccines, contain weakened forms of the virus, designed to trigger an immune response without causing the disease. However, in children with a history of Kawasaki disease, particularly those recently treated with intravenous immunoglobulin (IVIG) or on high-dose aspirin, these vaccines pose unique risks. IVIG can temporarily suppress the immune system, reducing the body's ability to respond effectively to live vaccines. Administering live vaccines within 11 months of IVIG treatment may result in suboptimal immunity or, in rare cases, vaccine-related complications. For instance, the varicella vaccine, given too soon after IVIG, could lead to a milder but still concerning form of chickenpox due to impaired immune response.
Consider the timing of live vaccines carefully in Kawasaki disease patients. The American Academy of Pediatrics (AAP) and Centers for Disease Control and Prevention (CDC) recommend delaying live vaccines for at least 11 months after IVIG administration. This waiting period ensures the immune system has recovered sufficiently to mount a robust response. For example, if a 2-year-old receives IVIG for Kawasaki disease in January, live vaccines like MMR or varicella should be postponed until December or later. If a child misses a dose due to this delay, consult a healthcare provider to reschedule without compromising the overall vaccination schedule.
A comparative analysis highlights the difference in risk between live and inactivated vaccines. Inactivated vaccines, such as the injectable polio vaccine or hepatitis A vaccine, do not carry the same risks as live vaccines in immunocompromised states. These can typically be administered without delay, even in children recovering from Kawasaki disease. However, live vaccines require a more cautious approach. For instance, the oral rotavirus vaccine, another live vaccine, should also be delayed post-IVIG, as it relies on a competent immune system to prevent vaccine-derived viral shedding.
Practical tips for parents and caregivers include maintaining open communication with healthcare providers about the child’s Kawasaki disease history and recent treatments. Keep a detailed record of IVIG administration dates and share this information with all healthcare providers involved in vaccination decisions. If a live vaccine is inadvertently given too soon after IVIG, monitor the child closely for signs of vaccine-related illness and report any concerns immediately. While delays in live vaccines may temporarily leave a child unprotected against certain diseases, the risk of complications from improper vaccination outweighs the benefits of adhering to a standard schedule. Always prioritize safety and follow evidence-based guidelines tailored to the child’s medical history.
Understanding Vaccine Ordering, Tracking, and Waste Management Challenges
You may want to see also
Explore related products






![]()
IVIG Treatment Impact
Kawasaki disease, an acute febrile illness primarily affecting children under five, often necessitates intravenous immunoglobulin (IVIG) treatment to reduce inflammation and prevent coronary artery complications. When administering IVIG, healthcare providers must carefully consider its impact on vaccine efficacy, as it can transiently suppress the immune system. The standard IVIG dose for Kawasaki disease is 2 g/kg, administered intravenously over 8–12 hours, which can interfere with the immune response to live-attenuated vaccines for up to 3 months post-treatment. This delay is crucial to ensure vaccines remain effective, as IVIG’s antibodies may neutralize the vaccine antigens, rendering immunization less protective.
Analyzing the interaction between IVIG and vaccines reveals a clear pattern: live-attenuated vaccines, such as MMR (measles, mumps, rubella), varicella (chickenpox), and rotavirus, are most affected. For instance, if a child receives IVIG for Kawasaki disease, the MMR vaccine should be delayed for at least 11 months to avoid potential interference. In contrast, inactivated vaccines like DTaP (diphtheria, tetanus, pertussis) and hepatitis B are less impacted and can generally be administered according to the standard schedule. This distinction underscores the importance of tailoring vaccine timing based on the type of vaccine and the child’s treatment history.
From a practical standpoint, parents and caregivers should maintain open communication with healthcare providers to ensure proper vaccine scheduling post-IVIG. For example, if a child is due for the varicella vaccine but has recently received IVIG, the vaccine should be postponed until the immune system has recovered. Additionally, documenting the IVIG treatment date in the child’s medical record is essential for future reference. Pediatricians may also recommend serologic testing to confirm immunity before revaccinating, particularly for live-attenuated vaccines, to avoid unnecessary delays or repeated doses.
Comparatively, the impact of IVIG on vaccine efficacy highlights the delicate balance between treating acute conditions and maintaining long-term immunity. While IVIG is a lifesaving intervention for Kawasaki disease, its immunomodulatory effects require careful management. For instance, children who receive IVIG before their first birthday may need to repeat certain vaccines later to ensure adequate protection. This approach contrasts with the standard vaccine schedule, emphasizing the need for individualized care in immunocompromised or treated populations.
In conclusion, the impact of IVIG treatment on vaccine efficacy in Kawasaki disease patients demands a nuanced approach to immunization. By delaying live-attenuated vaccines and closely monitoring vaccine timing, healthcare providers can ensure optimal protection while addressing the acute needs of the child. Parents and caregivers play a critical role in this process by staying informed and adhering to adjusted vaccine schedules. Ultimately, this tailored strategy minimizes risks and maximizes the benefits of both IVIG therapy and vaccination.
Business Owners: Vaccination Requirements and Your Rights
You may want to see also
Explore related products






![]()
Fever-Inducing Vaccines
Fever is a common side effect of many vaccines, typically mild and short-lived. However, in the context of Kawasaki disease, a condition characterized by inflammation of blood vessels and often accompanied by high fever, the potential for vaccine-induced fever raises specific concerns. Fever-inducing vaccines, while generally safe, may exacerbate symptoms or complicate the clinical picture in Kawasaki disease patients, making careful consideration of timing and type essential.
Analytically, the live attenuated vaccines, such as the measles, mumps, and rubella (MMR) vaccine and the varicella vaccine, are more likely to cause fever due to their mechanism of action. These vaccines contain weakened forms of the virus, which stimulate a robust immune response, sometimes resulting in fever. For children with Kawasaki disease, who may already have elevated temperatures and systemic inflammation, this additional fever could be problematic. Studies suggest delaying live vaccines until the acute phase of Kawasaki disease has resolved, typically 4–6 weeks after the onset of symptoms, to minimize the risk of complications.
Instructively, healthcare providers should assess the patient’s fever history and current inflammatory markers before administering any vaccine. For instance, if a child with Kawasaki disease has recently experienced persistent high fevers, delaying fever-inducing vaccines like MMR or varicella is prudent. Instead, prioritize non-live vaccines, such as the diphtheria, tetanus, and acellular pertussis (DTaP) or inactivated polio vaccine (IPV), which are less likely to cause fever. Always consult the patient’s cardiologist or immunologist to tailor the vaccination schedule to their specific condition.
Persuasively, while delaying certain vaccines may seem inconvenient, the benefits of avoiding potential complications far outweigh the risks. For example, a fever spike in a Kawasaki disease patient could mask signs of disease recurrence or treatment failure, complicating diagnosis and management. By postponing fever-inducing vaccines until the child is stable, caregivers can ensure a clearer clinical picture and reduce the burden on both the patient and healthcare system. This approach aligns with the precautionary principle in medicine, prioritizing safety above all else.
Comparatively, the approach to fever-inducing vaccines in Kawasaki disease contrasts with standard vaccination protocols for healthy children. Healthy children typically receive live vaccines according to the recommended schedule, with fever managed symptomatically using acetaminophen or ibuprofen. In Kawasaki disease, however, proactive delay and careful monitoring are necessary. For instance, the MMR vaccine, usually given at 12–15 months, might be postponed until the child is 18–24 months if Kawasaki disease is diagnosed in infancy. This tailored approach ensures that vaccination remains safe and effective without compromising the child’s recovery.
Practically, parents and caregivers can take steps to minimize fever risk when vaccines are administered. Administering vaccines in the morning allows for closer monitoring during the day, as fever is more likely to occur 6–12 hours post-vaccination. Keep a fever log to track temperature changes and report any unusual symptoms to the healthcare provider promptly. For children with Kawasaki disease, having a cooling plan—such as light clothing and a cool environment—can help manage fever if it occurs. Always follow the healthcare provider’s guidance on medication use, such as avoiding prophylactic antipyretics unless specifically advised.
MMRV Vaccine: How Many U.S. Children Received the Shot?
You may want to see also
Explore related products





![]()
Post-Kawasaki Immunization Schedule
Kawasaki disease, an acute febrile illness primarily affecting children under five, necessitates careful management of post-recovery immunization schedules. The inflammatory nature of the disease, particularly its impact on the cardiovascular system, raises concerns about vaccine safety and timing. While no vaccines are universally contraindicated, certain precautions and delays are recommended to minimize risks, especially in children with a history of coronary artery abnormalities. This tailored approach ensures both protection against vaccine-preventable diseases and avoidance of potential complications.
Step-by-Step Guidance for Post-Kawasaki Immunization:
- Initial Delay Post-Acute Phase: Vaccinations should be deferred for at least 1 month after the onset of Kawasaki disease to allow for resolution of acute inflammation. This precaution is particularly critical for live vaccines, such as MMR (measles, mumps, rubella) and varicella, which may pose theoretical risks during active inflammation.
- Cardiac Evaluation Before Resuming: Prior to restarting the immunization schedule, a cardiology consultation is essential for children with a history of coronary artery aneurysms or ectasia. If abnormalities persist, non-live vaccines (e.g., DTaP, IPV, Hib) can typically proceed, but live vaccines may require further delay until cardiac stability is confirmed.
- Age-Specific Considerations: For children under 12 months, the focus should be on completing core vaccinations like DTaP, IPV, and pneumococcal conjugate vaccine (PCV13), as these are less likely to exacerbate residual inflammation. Older children may resume age-appropriate vaccines, such as Tdap or HPV, after cardiac clearance.
- Practical Tips for Parents: Maintain a detailed record of the child’s Kawasaki disease history, including cardiac imaging results, to share with healthcare providers. Schedule immunizations during periods of optimal health, avoiding times of minor illnesses or stress, which could mimic Kawasaki symptoms.
Cautions and Comparative Analysis: While the inactivated influenza vaccine is generally safe, the live attenuated nasal spray (LAIV) should be avoided in children with a history of Kawasaki disease, especially those with cardiac involvement. This distinction highlights the importance of vaccine type in post-Kawasaki planning. Additionally, the COVID-19 vaccine, particularly mRNA formulations, has been administered safely in this population but should be timed carefully, ideally 3–6 months post-recovery, to avoid coincidental fever misinterpretation.
Travel Rules: Vaccination Requirements for Canadians Entering the U.S
You may want to see also
Frequently asked questions
There is no evidence to suggest that the COVID-19 vaccine should be delayed in children with a history of Kawasaki disease. However, consult a pediatrician or cardiologist to ensure there are no specific cardiac complications from Kawasaki disease that might require precautions.
The MMR vaccine can typically be given on schedule unless the child is severely ill or immunocompromised. Always consult a healthcare provider for personalized advice based on the child’s condition.
The flu vaccine is generally safe and should not be delayed unless the child is acutely ill. Discuss with a healthcare provider to ensure it’s appropriate during treatment.
The varicella vaccine is usually safe for children with a history of Kawasaki disease, but consult a healthcare provider, especially if there are ongoing cardiac issues or immunosuppression.
The HPV vaccine does not need to be delayed in adolescents with a history of Kawasaki disease unless there are specific medical concerns. Always consult a healthcare provider for individualized guidance.