The vaccination rate in the United States has been a critical public health metric, particularly in the wake of the COVID-19 pandemic, which underscored the importance of widespread immunization. As of recent data, the U.S. has made significant strides in vaccinating its population against various diseases, including COVID-19, influenza, and childhood illnesses like measles and polio. However, vaccination rates vary widely across states, demographics, and age groups, influenced by factors such as access to healthcare, public health messaging, and vaccine hesitancy. Understanding these rates is essential for assessing the nation’s preparedness to combat infectious diseases and for identifying areas where targeted interventions may be needed to improve coverage and protect public health.
Explore related products






What You'll Learn
- Overall Vaccination Rate Trends: National average vaccination rates over time, including historical data and recent updates
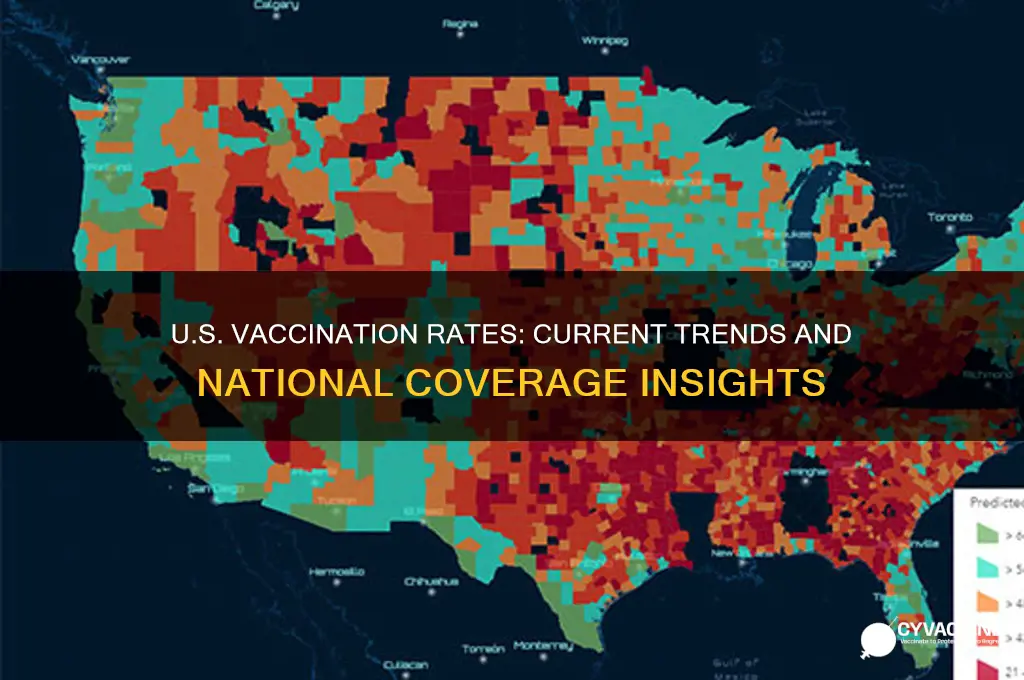
- State-by-State Breakdown: Vaccination rates by state, highlighting highest and lowest performing regions
- Demographic Disparities: Vaccination rates by age, race, ethnicity, and socioeconomic status
- Vaccine Type Distribution: Rates for COVID-19, flu, childhood vaccines, and other common immunizations
- Impact of Policies: Effect of mandates, incentives, and public health campaigns on vaccination rates
![]()
Overall Vaccination Rate Trends: National average vaccination rates over time, including historical data and recent updates
The United States has witnessed significant fluctuations in vaccination rates over the past century, reflecting both public health triumphs and ongoing challenges. Historical data reveals a dramatic rise in vaccination coverage following the introduction of vaccines for diseases like polio, measles, and pertussis in the mid-20th century. By the 1980s, childhood vaccination rates for diseases such as measles, mumps, and rubella (MMR) exceeded 90%, leading to the near-elimination of these diseases domestically. However, recent trends show a concerning decline in certain vaccine uptake, particularly among younger age groups. For instance, the CDC reported that during the 2020-2021 school year, MMR vaccination rates among kindergarteners dropped to 93.9%, the lowest in over a decade, likely exacerbated by the COVID-19 pandemic disrupting routine healthcare access.
Analyzing the data, the COVID-19 vaccination rollout provides a unique case study in rapid vaccination trends. As of October 2023, approximately 68% of the U.S. population has completed the primary COVID-19 vaccine series, with booster doses administered to about 32% of eligible individuals. This rollout highlights disparities in vaccine acceptance across regions and demographics. States like Vermont and Massachusetts boast vaccination rates above 75%, while others, such as Mississippi and Alabama, lag below 55%. Age remains a critical factor, with individuals over 65 achieving higher vaccination rates (over 90%) compared to younger adults (50-60%). These variations underscore the influence of local policies, socioeconomic factors, and public health messaging on vaccination behavior.
To address declining vaccination rates, public health initiatives must focus on rebuilding trust and improving accessibility. For childhood vaccines, schools and pediatricians play a pivotal role in ensuring timely immunizations. Parents should adhere to the CDC’s recommended vaccine schedule, which includes doses for diseases like hepatitis B, varicella, and Tdap, starting at birth and continuing through adolescence. Adults, too, require periodic vaccinations, such as the Td/Tdap booster every 10 years and annual flu shots. Practical tips include using immunization tracking tools like the CDC’s Vaccine Records app and scheduling vaccine appointments during routine healthcare visits to minimize missed opportunities.
Comparatively, the U.S. vaccination landscape mirrors global trends but with distinct challenges. While countries like Portugal and Singapore achieve over 95% childhood vaccination rates through stringent policies and public education, the U.S. system relies heavily on individual choice and state-level mandates. This decentralized approach has led to pockets of vaccine hesitancy, particularly in communities with misinformation or historical mistrust of medical institutions. For example, the rise of non-medical exemptions for school vaccinations in states like Oregon and Idaho has contributed to localized outbreaks of preventable diseases like measles. Addressing these disparities requires tailored strategies, including community-based education campaigns and stronger policy frameworks to balance individual freedoms with public health imperatives.
In conclusion, understanding national vaccination rate trends demands a nuanced approach that considers historical context, demographic factors, and systemic influences. While the U.S. has made remarkable strides in disease prevention through vaccination, recent declines signal a need for proactive measures. By leveraging data-driven insights, improving access, and fostering trust, public health officials can reverse negative trends and ensure sustained protection against vaccine-preventable diseases. Whether for routine childhood immunizations or emerging threats like COVID-19, vaccination remains a cornerstone of public health—one that requires collective effort to uphold.
Maldives Travel: Is Yellow Fever Vaccine Necessary?
You may want to see also
Explore related products






![]()
State-by-State Breakdown: Vaccination rates by state, highlighting highest and lowest performing regions
As of the latest data, vaccination rates in the United States vary significantly by state, reflecting a patchwork of public health efforts, demographic factors, and local policies. Vermont leads the nation with over 80% of its population fully vaccinated, a testament to its robust healthcare infrastructure and high community engagement. In contrast, states like Mississippi and Alabama lag behind, with rates hovering around 50%, underscoring persistent challenges in access and vaccine hesitancy. These disparities highlight the need for targeted strategies to address regional differences in vaccination uptake.
Analyzing the highest-performing states reveals common denominators: strong public health messaging, widespread availability of vaccines, and community-based initiatives. For instance, Vermont’s success can be attributed to its early rollout of mobile clinics and partnerships with local organizations to reach underserved populations. Similarly, Massachusetts, with a 78% vaccination rate, has leveraged its dense network of healthcare providers and universities to promote vaccine confidence. These states demonstrate that a combination of accessibility and trust-building measures can drive high vaccination rates.
On the other end of the spectrum, low-performing states often face barriers such as limited healthcare access, lower population density, and higher rates of skepticism. In Mississippi, for example, only 51% of the population is fully vaccinated, partly due to a lack of healthcare providers in rural areas and a history of mistrust in medical institutions. Alabama faces similar challenges, compounded by lower educational attainment rates, which correlate with vaccine hesitancy. Addressing these issues requires tailored solutions, such as deploying community health workers and combating misinformation through trusted local leaders.
A comparative analysis of these states also reveals age-specific trends. In high-performing regions, vaccination rates among seniors (65+) often exceed 90%, reflecting targeted campaigns to protect the most vulnerable. Conversely, younger adults (18-29) in low-performing states show lower uptake, influenced by perceptions of lower risk and misinformation on social media. Practical tips for improving rates include offering incentives like gift cards or paid time off for vaccination, hosting pop-up clinics at schools and workplaces, and using data to identify and target under-vaccinated neighborhoods.
Ultimately, the state-by-state breakdown of vaccination rates serves as a roadmap for improving national coverage. By studying the successes of Vermont and Massachusetts, and addressing the challenges in Mississippi and Alabama, policymakers can design interventions that bridge the gap. Whether through expanding access, building trust, or tailoring messaging, the goal remains clear: to protect every community, one dose at a time.
California's Vaccine Exemptions: What You Need to Know
You may want to see also
Explore related products






![]()
Demographic Disparities: Vaccination rates by age, race, ethnicity, and socioeconomic status
As of recent data, vaccination rates in the United States reveal stark disparities across demographic lines, particularly when broken down by age, race, ethnicity, and socioeconomic status. For instance, while over 90% of adults aged 65 and older have received at least one vaccine dose, rates among younger adults, especially those aged 18-29, lag significantly, hovering around 70%. This age-based gap underscores broader trends in health behavior and access, but it’s just the tip of the iceberg.
Consider racial and ethnic disparities: Black and Hispanic communities, historically underserved by healthcare systems, have faced systemic barriers to vaccination. While overall vaccination rates among Hispanic individuals have risen to nearly 75%, this group still lags behind White populations, where rates exceed 80%. Black Americans, despite initial hesitancy fueled by historical medical mistrust, have seen rates climb to around 70%, yet disparities persist. These gaps are not merely numbers—they reflect inequities in access to healthcare, vaccine distribution sites, and culturally competent outreach efforts. For example, pop-up clinics in predominantly Black neighborhoods, paired with community leaders as advocates, have proven effective in bridging this divide.
Socioeconomic status further complicates the picture. Individuals living in poverty or without stable employment are less likely to be vaccinated, often due to logistical hurdles like transportation, time off work, or lack of internet access for scheduling appointments. Rural areas, where poverty rates are higher, report vaccination rates up to 10% lower than urban centers. Practical solutions include mobile vaccination units, employer-sponsored vaccine drives, and financial incentives for low-wage workers to take time off for vaccination. For instance, offering a $25 grocery gift card at vaccine events in underserved areas has shown measurable impact.
Age intersects with these factors in critical ways. Older adults, despite high vaccination rates, often face challenges with booster doses, particularly in low-income communities where transportation to pharmacies is limited. Conversely, younger populations, especially teens and young adults, are less likely to perceive COVID-19 as a threat, contributing to lower vaccination rates. Tailored strategies, such as school-based vaccine clinics for adolescents or social media campaigns targeting Gen Z, can address these age-specific barriers. For parents of children aged 5-11, providing clear, accessible information about the pediatric dose (10 micrograms, compared to 30 micrograms for adults) can alleviate concerns and encourage uptake.
In addressing these disparities, a one-size-fits-all approach falls short. Success requires targeted interventions that acknowledge the unique challenges each demographic faces. For policymakers, this means allocating resources to areas with the greatest need, such as funding community health workers in predominantly Black or Hispanic neighborhoods. For healthcare providers, it involves offering flexible hours, multilingual services, and culturally sensitive education. And for individuals, it’s about advocating for equitable access in their communities, whether by volunteering at vaccine drives or amplifying trusted voices in underserved populations. Closing these gaps isn’t just about public health—it’s about justice.
Vaccinated Birds and Marek's Disease: Unraveling the Persistent Mystery
You may want to see also
Explore related products






![]()
Vaccine Type Distribution: Rates for COVID-19, flu, childhood vaccines, and other common immunizations
As of the latest data, COVID-19 vaccination rates in the United States have plateaued, with approximately 68% of the population fully vaccinated. This figure, however, masks significant disparities across age groups and geographic regions. For instance, vaccination rates among adults aged 65 and older are notably higher, nearing 90%, due to targeted public health campaigns and the group’s heightened vulnerability to severe outcomes. In contrast, younger adults and adolescents lag behind, with rates hovering around 60%. These variations highlight the need for tailored strategies to address hesitancy and accessibility barriers in specific demographics.
The distribution of flu vaccines presents a different landscape, with annual vaccination rates consistently falling below public health targets. On average, only about 50% of Americans receive the flu vaccine each year, despite its proven efficacy in reducing hospitalizations and deaths. Pediatricians play a critical role in this context, as childhood flu vaccination rates are slightly higher, around 65%, due to routine well-child visits and school immunization requirements. However, disparities persist among adults, particularly those without regular access to healthcare. Employers can bridge this gap by offering on-site flu clinics, a strategy that has shown to increase vaccination rates by up to 20% in workplace settings.
Childhood vaccines remain a cornerstone of public health, with coverage rates for vaccines like MMR (measles, mumps, rubella) and DTaP (diphtheria, tetanus, pertussis) exceeding 90% nationally. These high rates are largely due to stringent school entry requirements and the success of the Vaccines for Children program, which ensures access for uninsured or underinsured children. However, pockets of undervaccination persist in certain communities, driven by misinformation and logistical challenges. Parents can ensure timely immunization by following the CDC’s recommended schedule, which outlines specific doses at ages 2, 4, 6, and 11–12 years. Catch-up schedules are also available for children who fall behind, emphasizing the flexibility of the system.
Beyond COVID-19, flu, and childhood vaccines, other common immunizations like Tdap (tetanus, diphtheria, pertussis) and HPV (human papillomavirus) show varying uptake. Tdap vaccination during pregnancy, recommended to protect newborns from pertussis, has a coverage rate of approximately 55%, indicating room for improvement through provider education and reminders. HPV vaccination, targeting adolescents to prevent cancers, lags at around 59% for the full series, despite its inclusion in routine adolescent immunizations. Schools and healthcare providers can enhance HPV vaccine uptake by integrating it into existing health education programs and addressing parental concerns with evidence-based information.
Understanding vaccine type distribution is crucial for identifying gaps and tailoring interventions. For example, while COVID-19 and childhood vaccines benefit from widespread awareness and infrastructure, flu and HPV vaccines require more targeted efforts. Practical steps include leveraging electronic health records to send reminders, offering vaccines in non-traditional settings like pharmacies, and addressing misinformation through community-based initiatives. By focusing on these specifics, public health officials can work toward more equitable and comprehensive immunization coverage across all vaccine types.
Ohio Vaccine Lottery Registration Guide: Step-by-Step Process to Enter
You may want to see also
Explore related products






![]()
Impact of Policies: Effect of mandates, incentives, and public health campaigns on vaccination rates
As of the latest data, approximately 68% of the U.S. population is fully vaccinated against COVID-19, with significant variations by state, age, and demographic group. This rate reflects the cumulative impact of policies implemented since the vaccine rollout began in December 2020. Mandates, incentives, and public health campaigns have each played distinct roles in shaping this outcome, often interacting in complex ways. For instance, while federal vaccine mandates for healthcare workers and large employers faced legal challenges, state-level mandates for specific sectors, such as New York’s requirement for healthcare workers, achieved compliance rates exceeding 95%. Conversely, states without mandates or with prohibitions on mandates, like Florida, have seen slower uptake, with vaccination rates lagging by 10–15 percentage points.
Consider the instructive case of incentives: Ohio’s Vax-a-Million lottery, which offered $1 million prizes to vaccinated residents, coincided with a 43% increase in vaccinations among eligible age groups during the campaign period. However, such programs often yield short-term spikes rather than sustained growth. A 2021 study by the Urban Institute found that while incentives can motivate up to 15% of hesitant individuals, their effectiveness diminishes without concurrent education efforts. For example, pairing a $100 cash incentive with personalized text reminders increased vaccination rates by 25% in a Philadelphia pilot program, compared to incentives alone.
Public health campaigns, meanwhile, have leveraged behavioral science to address vaccine hesitancy. The CDC’s *We Can Do This* campaign, which featured localized testimonials and partnerships with community leaders, saw a 7% increase in vaccination intent among targeted audiences. Yet, messaging missteps can backfire: a 2021 survey by the Kaiser Family Foundation revealed that 23% of unvaccinated adults cited inconsistent messaging about booster doses as a reason for delaying vaccination. Effective campaigns, such as those in California that emphasized “community immunity” and provided multilingual materials, achieved higher uptake in diverse populations, with Latino vaccination rates rising from 45% to 62% in six months.
A comparative analysis of policy impacts reveals trade-offs. Mandates, while polarizing, produce immediate results in controlled environments—for example, vaccination rates among U.S. military personnel surged to 98% following the Department of Defense mandate. Incentives, though costly, can target specific demographics, as seen in programs offering $50 grocery vouchers to seniors in rural areas. Public health campaigns, while slower to yield results, build long-term trust and literacy, as evidenced by a 12% increase in flu vaccine uptake among communities exposed to consistent COVID-19 messaging.
To maximize vaccination rates, policymakers should adopt a layered approach: mandates for high-risk sectors, targeted incentives for hesitant groups, and culturally tailored campaigns. For instance, requiring vaccination for school attendance (with medical exemptions) could mirror the 95% measles vaccination rate in states with strict policies. Pairing this with a $50 incentive for first doses in underserved ZIP codes and a campaign featuring local healthcare workers could address access, motivation, and trust simultaneously. Practical tips include using pre-filled appointment links in incentive programs and ensuring campaigns address specific concerns, such as fertility myths for young adults or side-effect transparency for older populations.
Ultimately, the U.S. vaccination rate reflects not just policy strength but policy synergy. Mandates provide structure, incentives offer immediacy, and campaigns foster understanding. By combining these tools strategically, public health efforts can bridge the gap between current rates and herd immunity thresholds, estimated at 80–85% for COVID-19. The challenge lies in balancing coercion with persuasion, ensuring policies are both effective and equitable.
The Vaccine: A Killer Cure?
You may want to see also
Frequently asked questions
As of the latest data, approximately 68% of the total U.S. population is fully vaccinated against COVID-19, with variations by state and demographic group.
The U.S. vaccination rate is higher than the global average but lags behind some countries with robust vaccination campaigns, such as Canada, the UK, and several European nations.
States like Vermont, Massachusetts, and Connecticut have some of the highest vaccination rates, while states like Mississippi, Alabama, and Wyoming have among the lowest.
Vaccination rates are highest among older adults (e.g., 95% of those 65+ have at least one dose) and lower among younger age groups, particularly children under 5, who became eligible for vaccination later.
Key factors include access to vaccines, public health messaging, political and cultural beliefs, socioeconomic status, and geographic location.