Vaccination schedules play a critical role in public health by preventing the spread of infectious diseases and protecting individuals from serious illnesses. In the United States, the Centers for Disease Control and Prevention (CDC) provides recommended vaccination schedules for children, adolescents, and adults, designed to ensure timely immunization against vaccine-preventable diseases. However, adherence to these schedules varies widely across the population due to factors such as access to healthcare, socioeconomic status, geographic location, and personal beliefs. Understanding what percentage of Americans follow the recommended vaccination schedule is essential for identifying gaps in immunization coverage, addressing barriers to vaccination, and implementing strategies to improve public health outcomes. Recent studies and surveys have shed light on compliance rates, revealing both progress and challenges in achieving widespread adherence to these guidelines.
| Characteristics | Values |
|---|---|
| Overall Adherence to Vaccination Schedule | Approximately 70% of children and adolescents follow the recommended vaccination schedule (as of 2023 data). |
| Adult Vaccination Compliance | Only about 30-40% of adults adhere to recommended vaccines like flu, Tdap, and shingles vaccines. |
| Infant Vaccination Rates | Over 90% of infants receive initial doses of vaccines like MMR and DTaP, but completion rates drop slightly. |
| Racial/Ethnic Disparities | White and Asian populations have higher adherence rates compared to Black, Hispanic, and Native American populations. |
| Geographic Variations | Urban areas generally have higher vaccination rates than rural areas due to better access to healthcare. |
| Socioeconomic Factors | Higher income and education levels correlate with increased adherence to vaccination schedules. |
| Vaccine Hesitancy Impact | Approximately 20-25% of Americans express hesitancy or refusal of vaccines, affecting adherence rates. |
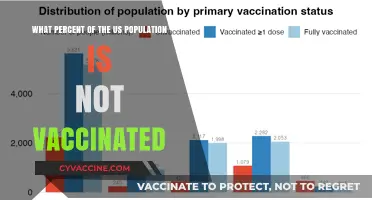
| COVID-19 Vaccine Uptake | About 68% of the U.S. population has completed the primary COVID-19 vaccination series (as of 2023). |
| Influenza Vaccination Rates | Around 50% of adults and 60% of children receive the annual flu vaccine. |
| HPV Vaccination Rates | Approximately 54% of adolescents are up to date with the HPV vaccine series. |
| Source of Data | CDC (Centers for Disease Control and Prevention), National Health Interview Survey (NHIS), and state-level health reports. |
Explore related products






What You'll Learn
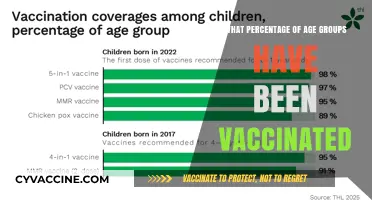
- Vaccination Rates by Age Group: Analyzes adherence to schedules across different age demographics in the U.S
- Geographic Disparities: Examines regional variations in vaccination compliance across states and cities
- Impact of Socioeconomic Factors: Explores how income, education, and access influence vaccination schedule adherence
- Vaccine Hesitancy Trends: Investigates the role of misinformation and distrust in reducing compliance rates
- Healthcare Access Barriers: Highlights how availability of healthcare services affects vaccination schedule follow-through
![]()
Vaccination Rates by Age Group: Analyzes adherence to schedules across different age demographics in the U.S
Childhood vaccination rates in the U.S. are a public health success story, with over 90% of children aged 19-35 months receiving recommended doses for vaccines like MMR (measles, mumps, rubella) and DTaP (diphtheria, tetanus, pertussis). This high adherence is largely due to school entry requirements and the convenience of bundling multiple vaccines into a single visit. However, disparities exist: children in rural areas or low-income households are less likely to be fully vaccinated, often due to limited access to healthcare providers or transportation challenges. Parents can ensure timely vaccinations by scheduling well-child visits at 2, 4, 6, and 15 months, and using tools like the CDC’s Catch-Up Immunization Scheduler if doses are missed.
Adolescents, aged 11-18, show lower adherence to recommended vaccines, particularly HPV (human papillomavirus) and meningococcal vaccines. Only about 54% of teens are up-to-date on HPV vaccination, despite its proven effectiveness in preventing cancers. This gap is partly due to misconceptions about HPV vaccine safety and a lack of consistent healthcare access during teenage years. Pediatricians and school-based health programs can improve rates by educating parents about the vaccine’s long-term benefits and offering reminders during annual check-ups. A practical tip for parents: pair HPV vaccine discussions with the Tdap booster, typically given at age 11, to streamline the conversation.
Among adults aged 19-64, vaccination rates plummet, with only 20-30% receiving recommended vaccines like Tdap, shingles, and pneumococcal vaccines. This age group often overlooks vaccinations, assuming they are only for children or the elderly. Employers can play a role by hosting workplace clinics for flu and COVID-19 boosters, while pharmacies can offer walk-in services for Tdap and shingles vaccines. Adults should consult their healthcare provider during annual physicals to review their vaccination status, especially before travel or if they have chronic conditions like diabetes or heart disease.
Seniors aged 65 and older exhibit higher adherence to vaccines like influenza and pneumococcal shots, with over 65% receiving annual flu vaccines. However, uptake of newer vaccines like shingles (Shingrix) remains lower, around 40%, despite its 90% efficacy. Medicare Part B covers many recommended vaccines, but seniors may be unaware of this benefit. Healthcare providers should proactively discuss vaccination needs during Medicare Annual Wellness Visits, and caregivers can assist by scheduling appointments and providing transportation. A key takeaway: Shingrix requires two doses, 2-6 months apart, so plan ahead to complete the series.
Across all age groups, vaccination adherence is influenced by socioeconomic factors, geographic location, and healthcare access. While children benefit from structured schedules, adolescents and adults require targeted interventions to bridge gaps. By understanding these age-specific trends, public health initiatives can tailor strategies—such as school-based programs for teens or workplace clinics for adults—to improve overall vaccination rates in the U.S.
Foreign Smoking Cessation Vaccines: Do They Exist?
You may want to see also
Explore related products






![]()
Geographic Disparities: Examines regional variations in vaccination compliance across states and cities
Vaccination compliance in the United States is not uniform; it varies significantly across geographic regions, influenced by factors such as local policies, socioeconomic conditions, and cultural attitudes. For instance, states like Vermont and Massachusetts consistently report high vaccination rates, often exceeding 80% for childhood immunizations, while states like Mississippi and West Virginia lag behind, with rates closer to 65%. These disparities are not merely statistical anomalies but reflect deeper systemic issues that impact public health outcomes.
Consider the role of state-level policies in shaping vaccination compliance. States with stricter school immunization requirements, such as California’s elimination of non-medical exemptions in 2015, tend to have higher vaccination rates. Conversely, states with more lenient policies, like Oregon, where non-medical exemptions are still permitted, often struggle to meet national benchmarks. City-level data further highlights these variations. Urban centers like New York City and Seattle, with robust public health infrastructure and targeted outreach programs, typically outperform rural areas, where access to healthcare services and vaccine education may be limited.
Socioeconomic factors also play a critical role in geographic disparities. In states with higher poverty rates, such as Louisiana and Alabama, vaccination compliance is often lower due to barriers like transportation challenges, lack of insurance, and limited access to healthcare providers. For example, a child in a low-income rural area may miss critical doses of the MMR vaccine (measles, mumps, rubella) due to the absence of nearby clinics, while a child in an urban area with multiple healthcare options is more likely to stay on schedule. Addressing these disparities requires targeted interventions, such as mobile clinics and financial assistance programs, to ensure equitable access to vaccines.
Cultural attitudes toward vaccination further exacerbate regional differences. In areas with strong anti-vaccine sentiment, such as parts of the Pacific Northwest and certain Midwestern states, misinformation spreads rapidly, leading to lower compliance rates. For instance, the HPV vaccine, recommended for adolescents aged 11–12, faces particular resistance in these regions, with uptake rates as low as 40% compared to the national average of 54%. Public health campaigns must counter misinformation with evidence-based messaging tailored to local communities, emphasizing the safety and efficacy of vaccines.
To bridge the gap in vaccination compliance, policymakers and healthcare providers must adopt region-specific strategies. In rural areas, investing in telehealth services and community health workers can improve access and education. In urban areas, addressing vaccine hesitancy through culturally sensitive outreach programs is essential. For example, offering vaccination clinics in schools or places of worship can increase convenience and trust. Ultimately, understanding and addressing geographic disparities is crucial for achieving national immunization goals and protecting public health.
Sending Your MMR Vaccine Record to College: A Step-by-Step Guide
You may want to see also
Explore related products






![]()
Impact of Socioeconomic Factors: Explores how income, education, and access influence vaccination schedule adherence
Socioeconomic disparities cast a long shadow over vaccination adherence in the United States. Data reveals a stark divide: children living below the poverty line are significantly less likely to receive all recommended vaccines by age 2 compared to their higher-income peers. This isn't merely a statistical anomaly; it's a symptom of a complex interplay between income, education, and access to healthcare.
Lower-income families often face financial barriers to vaccination. Missed work for appointments, transportation costs, and even the perceived cost of vaccines themselves (despite programs like Vaccines for Children) can deter timely immunization. A single missed dose can disrupt the entire schedule, leaving children vulnerable to preventable diseases.
Education plays a pivotal role in shaping health literacy and vaccine confidence. Parents with lower educational attainment may struggle to navigate complex vaccine schedules, understand the importance of timely doses, or critically evaluate misinformation. For instance, a study found that parents with lower educational levels were more likely to believe myths about vaccine safety, leading to hesitancy and delayed vaccinations.
Healthcare access is the final, critical piece of the puzzle. Families in underserved communities often lack convenient access to pediatricians or clinics offering vaccinations. Limited clinic hours, long wait times, and a shortage of healthcare providers in these areas create significant barriers to adherence. Imagine a single mother working multiple jobs, struggling to find transportation to a clinic open during her limited free time – the system is stacked against her child receiving timely vaccinations.
Addressing these disparities requires a multi-pronged approach. Expanding access to affordable, convenient vaccination services in underserved areas is crucial. This could involve mobile clinics, extended clinic hours, and partnerships with community organizations. Public health campaigns tailored to diverse educational levels and cultural backgrounds can combat misinformation and build trust in vaccines. Finally, policies that alleviate financial burdens, such as paid sick leave for vaccine appointments and robust insurance coverage, are essential to ensure that all children, regardless of socioeconomic status, have the opportunity to follow the recommended vaccination schedule.
No Vaccine Passport? Here’s What You Need to Know
You may want to see also
Explore related products






![]()
Vaccine Hesitancy Trends: Investigates the role of misinformation and distrust in reducing compliance rates
Misinformation spreads faster than measles, and its impact on vaccination rates is just as contagious. Despite the CDC’s recommended immunization schedule covering 14 vaccine-preventable diseases by age 2, adherence remains inconsistent. For instance, while 90% of U.S. children receive the MMR vaccine, only 70% of adults follow through with all recommended doses, including boosters like Tdap and shingles vaccines. This gap isn’t due to lack of access alone; it’s fueled by a toxic mix of false claims, eroded trust in institutions, and algorithmic amplification of anti-vaccine content. A single viral post can undo decades of public health messaging, leaving individuals vulnerable to preventable illnesses.
Consider the HPV vaccine, recommended for adolescents aged 11–12. Despite its proven efficacy in preventing six types of cancer, only 59% of teens complete the two-dose series. Misinformation linking it to infertility or chronic illness persists, even though studies show no such risks. Parents, bombarded with conflicting information, often delay or refuse the vaccine, prioritizing short-term fears over long-term protection. This hesitancy isn’t irrational—it’s a response to a fractured information ecosystem where distrust in pharmaceutical companies and government agencies amplifies doubts. Rebuilding trust requires more than facts; it demands transparency, empathy, and localized communication strategies.
Social media platforms, while not the sole culprits, act as accelerants for vaccine hesitancy. Algorithms prioritize engagement over accuracy, ensuring anti-vaccine content reaches wider audiences. For example, a 2021 study found that 70% of unvaccinated users on Facebook were exposed to misinformation within 24 hours of joining vaccine-related groups. These echo chambers reinforce skepticism, making evidence-based arguments seem like part of a larger conspiracy. Public health campaigns must adapt by leveraging trusted community figures—pediatricians, teachers, or religious leaders—to counter false narratives directly where they spread.
The COVID-19 pandemic exposed the fragility of vaccination compliance. While 68% of Americans completed the primary vaccine series, booster uptake plummeted to 20% by 2023. Fatigue, misinformation about side effects, and politicization of the vaccine created a perfect storm of hesitancy. Yet, the solution isn’t more data; it’s addressing the root cause—distrust. Initiatives like town halls with local health officials, transparent reporting of vaccine development, and partnerships with grassroots organizations can bridge the gap. Practical steps include offering vaccines in schools, workplaces, and pharmacies, removing barriers like cost or time constraints.
Ultimately, combating vaccine hesitancy requires a dual approach: dismantling misinformation while rebuilding trust. Fact-checking alone isn’t enough; narratives must be replaced with relatable stories of vaccine success. For instance, highlighting how the flu vaccine reduces hospitalizations by 40–60% annually can reframe its value. Pairing this with policies that ensure equitable access—like mobile clinics in underserved areas—creates a foundation for compliance. The goal isn’t to eliminate questions but to ensure they’re answered with accuracy, compassion, and respect for individual concerns. In this battle, every dose administered is a step toward herd immunity—and a victory against the spread of doubt.
Kroger's Shingrix Vaccine Administration Fee: What You Need to Know
You may want to see also
Explore related products






![]()
Healthcare Access Barriers: Highlights how availability of healthcare services affects vaccination schedule follow-through
The availability of healthcare services is a critical determinant in whether Americans adhere to the recommended vaccination schedule. Geographic disparities play a significant role; rural areas often lack sufficient healthcare facilities, making it difficult for residents to access routine immunizations. For instance, a family in a remote region may need to travel hours to reach the nearest clinic, a barrier that urban dwellers rarely face. This logistical challenge disproportionately affects low-income families, who may also lack reliable transportation or flexible work schedules to accommodate such trips. Without convenient access, even those who intend to follow the vaccination schedule may fall behind, leaving gaps in immunity that can have broader public health consequences.
Another layer of this issue is the shortage of healthcare providers in underserved communities. Pediatricians and family physicians are often overburdened, leading to long wait times for appointments. For example, a child due for a 2-month vaccination, which includes doses of DTaP, IPV, Hib, HepB, and PCV13, may not be seen until they are 3 or 4 months old due to scheduling delays. This not only disrupts the recommended timeline but also increases the risk of vaccine-preventable diseases during the interim period. Telehealth services, while growing in popularity, are not a viable solution for vaccinations, as they require in-person administration, further highlighting the need for physical healthcare infrastructure.
Financial barriers also intersect with healthcare access, particularly for uninsured or underinsured individuals. Despite programs like the Vaccines for Children (VFC) program, which provides free vaccines for eligible children, adults often face out-of-pocket costs that can deter them from completing their vaccination schedules. For example, the Tdap booster, recommended every 10 years, can cost upwards of $100 without insurance coverage. This financial strain, combined with limited clinic availability, creates a compounding effect that discourages follow-through, especially for multi-dose vaccines like HPV, which requires two to three doses over 6 to 12 months.
Addressing these barriers requires a multi-faceted approach. Expanding mobile vaccination clinics, particularly in rural and underserved areas, can bridge the gap by bringing services directly to communities. Additionally, extending clinic hours or offering weekend appointments can accommodate working families. Policymakers must also prioritize funding for healthcare infrastructure and workforce development in these regions. For individuals, practical tips include scheduling vaccination appointments well in advance, exploring local health department resources, and inquiring about financial assistance programs. By tackling these access barriers head-on, we can improve adherence to vaccination schedules and strengthen overall public health resilience.
Is RSV a Once-in-a-Lifetime Vaccine? What You Need to Know
You may want to see also
Frequently asked questions
According to the Centers for Disease Control and Prevention (CDC), approximately 70% of U.S. children aged 19-35 months receive all recommended vaccines by their second birthday, though rates vary by vaccine and demographic group.
Adult vaccination rates in the U.S. are lower than those for children. For example, only about 30-40% of adults receive the annual flu vaccine, and less than 30% are up to date with vaccines like Tdap (tetanus, diphtheria, pertussis) and shingles vaccines.
Adherence is influenced by access to healthcare, socioeconomic status, education, geographic location, vaccine availability, and personal beliefs or misinformation about vaccines.
Yes, disparities exist. Lower vaccination rates are often observed in rural areas, among racial and ethnic minorities, and in populations with lower income or limited access to healthcare, highlighting inequities in vaccine access and uptake.