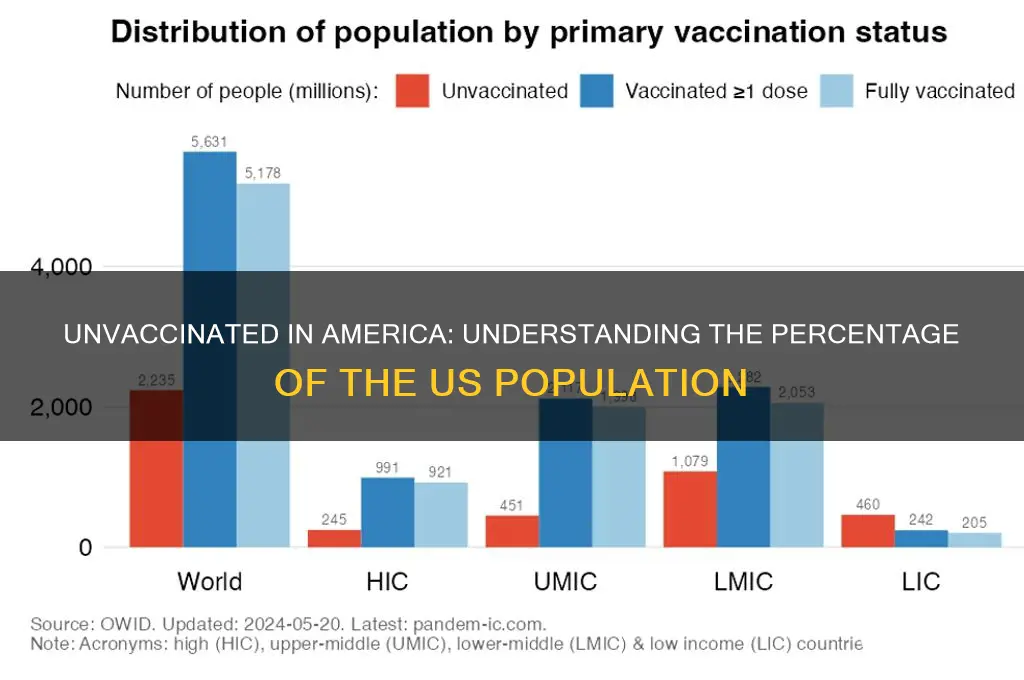
The percentage of the U.S. population that remains unvaccinated against COVID-19 is a critical public health concern, as it directly impacts disease transmission, hospitalization rates, and the potential for new variants to emerge. As of recent data, approximately 10-15% of the eligible U.S. population (ages 5 and older) has not received a single dose of a COVID-19 vaccine, though this figure varies by state and demographic group. Factors such as vaccine hesitancy, access barriers, and misinformation continue to influence these numbers, highlighting the need for targeted outreach and education to address remaining gaps in immunization coverage.
Explore related products





What You'll Learn
- Vaccine Hesitancy Demographics: Age, race, education, and income levels influencing unvaccinated populations in the U.S
- Regional Variations: State-by-state differences in vaccination rates and unvaccinated percentages
- Children and Vaccines: Percentage of unvaccinated children under 12 and reasons behind it
- Religious Exemptions: Impact of religious beliefs on vaccination rates and unvaccinated numbers
- Access Barriers: How healthcare access and misinformation contribute to unvaccinated populations
![]()
Vaccine Hesitancy Demographics: Age, race, education, and income levels influencing unvaccinated populations in the U.S
As of recent data, approximately 10-15% of the U.S. population remains unvaccinated against COVID-19, a figure that varies by demographic factors such as age, race, education, and income. Understanding these disparities is crucial for tailoring public health strategies to address vaccine hesitancy effectively.
Age and Vaccine Hesitancy: A Generational Divide
Young adults aged 18-29 and older adults aged 65+ represent the highest and lowest unvaccinated rates, respectively. While younger individuals may perceive lower personal risk or distrust health messaging, older adults often prioritize health, driven by higher vulnerability to severe illness. Public health campaigns should leverage peer influencers for younger demographics and emphasize community protection for older groups. For instance, hosting vaccine drives at colleges or senior centers with age-specific educational materials can bridge this gap.
Racial and Ethnic Disparities: Historical Context Matters
Black and Hispanic communities exhibit higher unvaccinated rates compared to White populations, often rooted in systemic mistrust stemming from historical injustices like the Tuskegee experiments. However, targeted initiatives, such as partnerships with community leaders and culturally sensitive messaging, have shown promise. For example, mobile clinics in underserved neighborhoods and bilingual outreach can improve accessibility and trust, reducing hesitancy by addressing logistical and cultural barriers.
Education and Income: Knowledge vs. Access
Individuals with lower educational attainment and income levels are disproportionately unvaccinated. Limited health literacy and financial constraints, such as unpaid leave for vaccine side effects, exacerbate this trend. Employers can play a pivotal role by offering paid time off for vaccination and recovery, while schools and workplaces can host workshops to debunk myths. A practical tip: provide clear, concise information about vaccine safety and efficacy in multiple languages, paired with incentives like gift cards or discounts for vaccination.
Intersectionality: Where Demographics Overlap
The most significant hesitancy occurs at the intersection of multiple factors—for example, low-income Black adults with limited education face compounded barriers. Addressing these requires multifaceted approaches, such as combining transportation assistance with community-led education campaigns. Policymakers must allocate resources to these groups, ensuring that solutions are both equitable and sustainable. By focusing on these intersections, public health efforts can move beyond one-size-fits-all strategies to create meaningful, lasting change.
US Vaccination Rates: Tracking the Percentage of Americans Immunized
You may want to see also
Explore related products






![]()
Regional Variations: State-by-state differences in vaccination rates and unvaccinated percentages
As of recent data, vaccination rates across the United States exhibit striking regional disparities, with some states boasting near-universal coverage while others lag significantly behind. For instance, Vermont leads the nation with over 80% of its population fully vaccinated, a testament to robust public health campaigns and high community trust in medical institutions. In contrast, states like Mississippi and Alabama report vaccination rates below 50%, reflecting a complex interplay of socioeconomic factors, political leanings, and healthcare access. These variations underscore the importance of localized strategies to address vaccine hesitancy and logistical barriers.
Consider the role of urban versus rural divides in shaping these trends. Urban centers, such as those in California and New York, often have higher vaccination rates due to greater access to clinics, pharmacies, and mobile vaccination units. Rural areas, however, face challenges like limited healthcare infrastructure and longer travel distances, contributing to lower uptake. For example, in Wyoming, only 40% of the population is fully vaccinated, compared to 70% in urbanized New Jersey. To bridge this gap, targeted initiatives like pop-up clinics at community centers or workplaces could prove effective, particularly in underserved regions.
Another critical factor is the influence of state-level policies and public messaging. States with mandates for certain groups, such as healthcare workers or schoolchildren, tend to have higher vaccination rates. For instance, Rhode Island’s strict school vaccination requirements have contributed to its 85% adolescent vaccination rate. Conversely, states like Florida, which have actively discouraged mandates, see lower overall compliance. Policymakers in hesitant regions could emulate successful models by pairing mandates with education campaigns that address specific concerns, such as vaccine safety or efficacy.
Age-specific trends further highlight regional differences. While national data shows that older adults (65+) have the highest vaccination rates, exceeding 90% in many states, younger populations (12–39) exhibit wider disparities. In Minnesota, for example, 80% of seniors are vaccinated, but only 55% of 18–29-year-olds have received their shots. This gap may stem from differing risk perceptions or misinformation targeting younger demographics. Tailored outreach, such as social media campaigns debunking myths or incentives like discounts at local businesses, could encourage younger individuals to get vaccinated.
Finally, socioeconomic and cultural factors cannot be overlooked. States with higher poverty rates, such as West Virginia, often struggle with lower vaccination coverage due to limited access to healthcare and lower health literacy. Similarly, communities with strong religious or political opposition to vaccines, as seen in parts of the South, face unique challenges. Addressing these barriers requires culturally sensitive approaches, such as engaging local leaders as advocates or offering multilingual resources. By understanding and adapting to these regional nuances, public health efforts can make meaningful strides in reducing unvaccinated percentages nationwide.
Smallpox Eradication: Key Factors Behind the Vaccine Program's Triumph
You may want to see also
Explore related products



$20.29 $35



![]()
Children and Vaccines: Percentage of unvaccinated children under 12 and reasons behind it
As of recent data, approximately 5-10% of children under 12 in the U.S. remain unvaccinated against preventable diseases, a figure that varies by region and demographic. This percentage, while smaller than the unvaccinated adult population, raises significant public health concerns due to the vulnerability of this age group. Unlike adults, children under 12 often rely on herd immunity for protection, making even small gaps in vaccination coverage potentially dangerous. For instance, measles outbreaks have occurred in communities where vaccination rates dropped below 95%, the threshold needed for herd immunity. Understanding the reasons behind this unvaccinated percentage is crucial for addressing the issue effectively.
One primary reason for unvaccinated children under 12 is parental hesitancy, often fueled by misinformation about vaccine safety. Despite decades of research confirming the safety and efficacy of vaccines—such as the MMR vaccine, which requires two doses starting at 12 months—misconceptions persist. For example, a debunked 1998 study linking the MMR vaccine to autism continues to influence some parents, even though it has been retracted and its author discredited. Public health campaigns must counter this misinformation with clear, evidence-based communication, emphasizing that vaccines undergo rigorous testing and monitoring. Practical tips for parents include consulting trusted healthcare providers and verifying information through reputable sources like the CDC or WHO.
Another factor contributing to unvaccinated children is systemic barriers, particularly in underserved communities. Access to healthcare, transportation challenges, and lack of insurance can prevent families from completing the recommended vaccine schedule. For instance, the CDC’s Vaccines for Children (VFC) program provides free vaccines to eligible children, but awareness and enrollment remain low in some areas. Addressing these barriers requires community-based initiatives, such as mobile clinics and school-based vaccination programs. Policymakers should also consider expanding Medicaid coverage and reducing administrative hurdles to ensure equitable access.
Comparatively, philosophical or religious exemptions also play a role, though their impact varies by state. As of 2023, 44 states allow religious exemptions for school-required vaccines, and 15 permit philosophical exemptions. States with more lenient policies tend to have higher rates of unvaccinated children. For example, Idaho and Oregon, which allow both types of exemptions, have seen clusters of vaccine-preventable diseases like pertussis. While respecting individual beliefs is important, public health policies must balance these exemptions with the collective need for disease prevention. A potential solution is tightening exemption criteria and requiring annual education sessions for parents seeking exemptions.
In conclusion, the percentage of unvaccinated children under 12 in the U.S. is driven by a combination of parental hesitancy, systemic barriers, and policy gaps. Addressing this issue requires a multi-faceted approach: combating misinformation with accurate information, improving healthcare access, and refining exemption policies. By focusing on these areas, we can protect vulnerable children and strengthen community immunity, ensuring that preventable diseases remain a thing of the past.
Alabama Vaccine Sign-Up Guide: Easy Steps to Schedule Your COVID-19 Shot
You may want to see also
Explore related products






![]()
Religious Exemptions: Impact of religious beliefs on vaccination rates and unvaccinated numbers
As of recent data, approximately 10-15% of the U.S. population remains unvaccinated against COVID-19, with religious exemptions playing a notable role in this statistic. While medical and philosophical exemptions also contribute, religious objections have emerged as a significant factor, particularly in states with lenient exemption policies. This trend raises questions about the intersection of faith, public health, and individual rights, especially as vaccine-preventable diseases like measles and pertussis continue to pose risks.
Analyzing the Landscape: Religious Exemptions and Vaccination Rates
Religious exemptions to vaccination are rooted in deeply held beliefs, often tied to interpretations of faith that conflict with medical interventions. For instance, some Christian Scientists cite reliance on prayer for healing, while certain Orthodox Jewish communities have expressed concerns about vaccine ingredients. In states like Pennsylvania and Texas, where religious exemptions are relatively easy to obtain, vaccination rates for diseases like measles have dipped below the 95% threshold needed for herd immunity. This gap highlights the tangible impact of religious beliefs on public health outcomes, particularly in schools and close-knit communities where outbreaks can spread rapidly.
Practical Considerations: Navigating Exemptions and Risks
For parents seeking religious exemptions, the process varies widely by state. In Oregon, a notarized statement is sufficient, while Mississippi and West Virginia allow no non-medical exemptions at all. However, obtaining an exemption does not eliminate the risk of disease. Unvaccinated individuals are 35 times more likely to contract measles, a highly contagious virus that can lead to pneumonia, encephalitis, or death. Public health officials recommend that exempt families stay informed about local outbreaks and consider alternative protective measures, such as voluntary quarantine during outbreaks.
Persuasive Argument: Balancing Faith and Community Health
While religious freedom is a cornerstone of American society, the collective impact of exemptions cannot be ignored. A single unvaccinated child can serve as a vector for disease, endangering infants too young to be vaccinated or immunocompromised individuals. Faith leaders and medical professionals increasingly collaborate to address misconceptions, emphasizing that vaccines align with the principle of preserving life. For example, the Catholic Church has endorsed vaccination, stating that morally produced vaccines are acceptable. Such endorsements can sway hesitant communities, bridging the gap between spiritual convictions and scientific consensus.
Comparative Perspective: Lessons from History
Historically, religious exemptions have played a role in vaccine hesitancy, but their impact has been mitigated through education and policy. During the 1990s measles resurgence, states tightened exemption laws, leading to a 30% reduction in outbreaks. Today, the challenge lies in balancing individual rights with public safety. Countries like France and Germany have adopted stricter policies, requiring counseling sessions before granting exemptions. These models suggest that informed consent, coupled with accessible health education, can reduce reliance on exemptions while respecting religious beliefs.
Takeaway: A Path Forward
Addressing the impact of religious exemptions requires a nuanced approach—one that respects faith while prioritizing community health. Policymakers can strengthen exemption processes by mandating consultations with healthcare providers, ensuring families understand the risks. Simultaneously, faith-based initiatives can foster dialogue, leveraging trusted leaders to dispel myths. By combining empathy with evidence, society can navigate this complex issue, protecting both individual freedoms and public well-being.
Easy Steps to Schedule Your Vaccine Appointment at Publix
You may want to see also
Explore related products






![]()
Access Barriers: How healthcare access and misinformation contribute to unvaccinated populations
As of recent data, approximately 10-15% of the U.S. population remains unvaccinated against COVID-19, a figure that highlights persistent gaps in public health efforts. While personal choice plays a role, systemic barriers to healthcare access and the pervasive spread of misinformation are critical factors driving this statistic. These issues disproportionately affect marginalized communities, creating a cycle of vulnerability that extends beyond the pandemic.
Consider the logistical hurdles faced by rural populations. In areas where the nearest vaccination site is hours away, transportation becomes a prohibitive barrier. For instance, a single mother working multiple jobs may lack the time or means to travel for a vaccine, especially when factoring in potential side effects that could disrupt her ability to work. Similarly, individuals without health insurance often avoid seeking care due to fear of hidden costs, despite vaccines being free. These access issues are compounded by limited clinic hours, which rarely align with the schedules of hourly workers. Addressing these barriers requires practical solutions, such as mobile clinics, extended hours, and clear communication about cost-free services.
Misinformation, however, operates on a different but equally damaging level. Social media platforms amplify false claims about vaccine safety, often targeting communities with historical reasons to distrust medical institutions. For example, a study found that 40% of unvaccinated Black Americans cited concerns rooted in the Tuskegee Syphilis Study as a reason for hesitancy. While this mistrust is valid, it’s often exploited by bad actors spreading unverified claims, such as the myth that vaccines alter DNA or contain microchips. Combating this requires culturally sensitive messaging and trusted messengers—community leaders, clergy, or local healthcare providers—who can debunk myths while acknowledging legitimate historical grievances.
The intersection of access barriers and misinformation creates a perfect storm. A Latino immigrant family, for instance, might face language barriers that prevent them from understanding vaccine information, while simultaneously encountering false claims on WhatsApp groups. Without bilingual resources or reliable sources, they remain unvaccinated not out of choice, but due to systemic exclusion. Bridging this gap demands targeted interventions: translated materials, partnerships with community organizations, and fact-checking initiatives tailored to specific cultural contexts.
Ultimately, reducing the unvaccinated population requires addressing these dual challenges head-on. Policymakers must invest in infrastructure that brings healthcare to underserved areas, while simultaneously funding campaigns that counter misinformation with empathy and evidence. Until these barriers are dismantled, the 10-15% figure will persist, reflecting not individual failure, but systemic shortcomings that demand urgent correction.
AstraZeneca Vaccine: Is It Available in the US?
You may want to see also
Frequently asked questions
As of 2023, approximately 10-15% of the US population remains unvaccinated against COVID-19, though this figure varies by source and region.
Yes, the percentage often includes all age groups, including children under 5, though vaccination rates for younger children tend to be lower compared to older populations.
Yes, there are notable regional differences, with rural areas and certain states in the South and Midwest generally having higher percentages of unvaccinated individuals compared to urban areas and states in the Northeast and West Coast.
Medical exemptions account for a very small percentage of the unvaccinated population, typically less than 1%, as most people are unvaccinated by choice or due to hesitancy rather than medical reasons.
The US has a higher percentage of unvaccinated individuals compared to many other developed countries, such as those in Western Europe, where vaccination rates are generally higher due to stronger public health campaigns and higher trust in vaccines.