As of the latest global health reports, the percentage of the world’s population that has received at least one dose of a COVID-19 vaccine stands at approximately 65%, with significant variations across regions. High-income countries have achieved vaccination rates exceeding 80%, while many low-income nations struggle to reach 20% due to disparities in vaccine distribution, infrastructure, and access. Efforts by international organizations like COVAX aim to bridge this gap, but challenges such as vaccine hesitancy, logistical hurdles, and inequitable supply chains persist. Monitoring global vaccination rates remains crucial for controlling the pandemic and preventing future outbreaks.
Explore related products






What You'll Learn
![]()
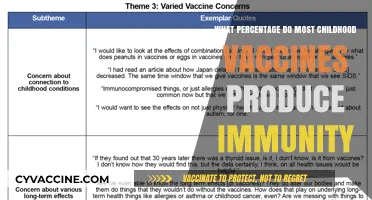
Global Vaccination Rates by Region
As of the latest data, global vaccination rates vary significantly by region, reflecting disparities in healthcare infrastructure, economic resources, and policy priorities. For instance, high-income countries in North America and Western Europe have achieved vaccination rates exceeding 70% for COVID-19, with many individuals receiving booster doses to maintain immunity. In contrast, low-income regions such as Sub-Saharan Africa and parts of Southeast Asia report rates below 30%, often due to limited vaccine supply and distribution challenges. These differences highlight the urgent need for equitable vaccine distribution and localized strategies to address regional barriers.
Analyzing the data reveals that vaccination rates are not solely determined by vaccine availability but also by cultural attitudes, misinformation, and logistical hurdles. In South Asia, for example, India has administered over 2 billion COVID-19 vaccine doses, yet its vast population means that only approximately 65% of the population is fully vaccinated. Meanwhile, smaller countries like Bhutan have achieved nearly 100% vaccination rates through targeted campaigns and community engagement. This underscores the importance of tailoring vaccination efforts to regional contexts, including addressing hesitancy through trusted local leaders and accessible education.
From a comparative perspective, the Americas showcase both extremes of vaccination success. While the United States and Canada boast high vaccination rates, particularly among older adults, Latin American countries like Haiti and Nicaragua struggle with rates below 20%. Economic sanctions, political instability, and reliance on global vaccine-sharing initiatives like COVAX have hindered progress in these regions. Practical steps to improve global equity include increasing funding for COVAX, waiving vaccine patents, and strengthening local healthcare systems to ensure sustainable distribution networks.
A persuasive argument for prioritizing regional vaccination equity lies in its global health and economic benefits. Unvaccinated populations serve as reservoirs for virus mutations, threatening the efficacy of existing vaccines worldwide. For instance, the Omicron variant emerged in regions with low vaccination rates, emphasizing the interconnectedness of global health. By investing in equitable vaccination, high-income countries not only protect vulnerable populations but also reduce the risk of future pandemics. This requires a shift from short-term donations to long-term partnerships that build regional manufacturing capabilities and healthcare resilience.
Finally, a descriptive examination of vaccination trends in the Middle East and North Africa (MENA) region offers valuable insights. Countries like the United Arab Emirates and Israel have led global vaccination efforts, with over 90% of their populations fully vaccinated. However, conflict-affected nations like Yemen and Syria face rates below 10%, exacerbated by humanitarian crises and fragmented governance. Practical tips for improving MENA vaccination rates include leveraging religious institutions to combat misinformation, utilizing mobile clinics to reach remote areas, and integrating vaccination campaigns with existing health services. Such region-specific approaches are essential for closing the global vaccination gap.
Smallpox Vaccine in India: Understanding the Name and Its History
You may want to see also
Explore related products






![]()
Vaccination Trends in Developed Countries
As of recent data, approximately 69% of the global population has received at least one dose of a COVID-19 vaccine, with significant disparities between developed and developing nations. In developed countries, vaccination rates often exceed 75%, reflecting robust healthcare infrastructure and public health campaigns. However, these nations now face new challenges, such as administering booster doses and addressing vaccine hesitancy among specific demographics. For instance, in the United States, while 80% of adults have completed their primary series, only 20% of those eligible have received the updated bivalent booster, highlighting gaps in ongoing vaccination efforts.
Analyzing trends in developed countries reveals a shift from mass vaccination drives to targeted strategies. Countries like Canada and Germany are prioritizing high-risk groups, including individuals over 65 and those with comorbidities, for booster shots. For example, Germany’s Standing Committee on Vaccination (STIKO) recommends a second booster for vulnerable populations, emphasizing personalized vaccination plans. This approach contrasts with earlier blanket campaigns and underscores the evolving nature of immunization strategies in response to new variants and waning immunity.
Persuasively, developed nations must address vaccine hesitancy to sustain high vaccination rates. In France, despite 80% of the population being fully vaccinated, skepticism about booster doses persists, particularly among younger adults. Public health officials are employing creative measures, such as mobile vaccination units and partnerships with local pharmacies, to improve accessibility and trust. Similarly, the UK’s “Get Vaccinated for Winter” campaign combines data-driven messaging with community engagement to combat misinformation and encourage uptake.
Comparatively, the pace of pediatric vaccination in developed countries varies widely. While the U.S. has administered at least one dose to 60% of children aged 5–11, uptake in countries like Sweden and Norway remains below 30%. This disparity reflects differing regulatory approvals, cultural attitudes, and risk perceptions. For parents in countries with lower pediatric vaccination rates, practical tips include consulting healthcare providers for personalized advice and leveraging school-based vaccination programs where available.
In conclusion, vaccination trends in developed countries are marked by a transition from initial mass campaigns to nuanced, data-driven strategies. Success hinges on addressing booster fatigue, combating hesitancy, and tailoring efforts to specific demographics. As global vaccination efforts continue, these nations serve as both models and cautionary tales, demonstrating the complexities of sustaining high immunization rates in an ever-changing public health landscape.
Inactivated Poliovirus Vaccine: How It Fights Polio and Prevents Paralysis
You may want to see also
Explore related products



$27.74 $32.99



![]()
Challenges in Low-Income Nations
As of the latest data, approximately 65% of the world’s population has received at least one dose of a COVID-19 vaccine, but this global average masks stark disparities. In low-income nations, vaccination rates often hover below 20%, with some countries struggling to reach even 10%. This gap is not merely a statistic but a reflection of systemic challenges that hinder vaccine distribution and uptake. Understanding these obstacles is crucial for devising targeted solutions that address the unique needs of these regions.
One of the most pressing challenges in low-income nations is the lack of infrastructure to support large-scale vaccination campaigns. Many of these countries have limited cold chain facilities, which are essential for storing vaccines at the required temperatures. For instance, the Pfizer-BioNTech vaccine must be stored at -70°C, a logistical nightmare for nations with unreliable electricity or inadequate refrigeration systems. Even vaccines with less stringent storage requirements, like AstraZeneca (which can be stored at 2-8°C), face distribution hurdles due to poor transportation networks. Without robust infrastructure, vaccines often expire before reaching remote or rural populations, exacerbating inequities.
Another critical issue is vaccine hesitancy, fueled by misinformation and distrust in healthcare systems. In low-income nations, where access to reliable information is limited, rumors and myths about vaccines spread rapidly. For example, in some communities, false claims that vaccines cause infertility or contain harmful substances have led to widespread refusal. Addressing this requires culturally sensitive communication strategies, such as engaging local leaders and using community health workers to disseminate accurate information. Additionally, translating vaccine materials into local languages and leveraging trusted media channels can help bridge the knowledge gap.
Financial constraints further compound these challenges. Low-income nations often lack the funds to purchase vaccines outright, relying instead on global initiatives like COVAX. However, COVAX has faced significant funding shortfalls and supply chain disruptions, leaving many countries with insufficient doses. Even when vaccines are available, the cost of administering them—including training healthcare workers, setting up vaccination sites, and monitoring side effects—can strain already overburdened health systems. International donors and organizations must prioritize sustainable funding models to ensure long-term vaccine accessibility.
Finally, political instability and conflict pose unique barriers in many low-income nations. In countries like Yemen or South Sudan, ongoing violence disrupts healthcare services, making it nearly impossible to conduct vaccination campaigns. Humanitarian corridors and ceasefires are sometimes negotiated to deliver vaccines, but these efforts are often temporary and insufficient. Addressing this challenge requires a dual approach: advocating for peace and stability while simultaneously developing flexible vaccine distribution strategies that can adapt to volatile environments.
In conclusion, the low vaccination rates in low-income nations are not due to a single issue but a complex interplay of infrastructure deficiencies, misinformation, financial constraints, and political instability. Tackling these challenges demands coordinated global efforts, innovative solutions, and a commitment to equity. Only by addressing these barriers can we hope to achieve a more equitable distribution of vaccines and protect the world’s most vulnerable populations.
Can Cats Get a Toxoplasmosis Vaccine? Exploring Prevention Options
You may want to see also
Explore related products






![]()
Impact of Vaccine Hesitancy Worldwide
As of recent data, approximately 68% of the world’s population has received at least one dose of a COVID-19 vaccine, with significant disparities across regions. High-income countries boast vaccination rates exceeding 80%, while low-income nations struggle below 20%. This uneven distribution underscores a global health crisis, but vaccine hesitancy compounds the problem, even in regions with ample supply. From misinformation campaigns to historical mistrust of medical systems, hesitancy erodes progress, leaving communities vulnerable to outbreaks and new variants.
Consider the case of Eastern Europe, where vaccine hesitancy has driven some of the lowest uptake rates globally. In countries like Bulgaria and Romania, less than 30% of the population is fully vaccinated against COVID-19. This reluctance stems from deep-rooted skepticism, amplified by social media disinformation. For instance, false claims linking vaccines to infertility or chronic illnesses have deterred younger age groups, who often require two doses of mRNA vaccines (e.g., Pfizer or Moderna) or a single-dose option like Johnson & Johnson. Without targeted education campaigns addressing these fears, hesitancy persists, hindering herd immunity and prolonging the pandemic’s impact.
In contrast, African nations face a dual challenge: limited vaccine access and growing hesitancy. While supply shortages initially slowed vaccination efforts, recent studies show that up to 40% of people in countries like Nigeria and the Democratic Republic of Congo are hesitant to receive doses when available. This reluctance is fueled by colonial-era medical exploitation and mistrust of foreign-developed vaccines. Practical solutions include involving local leaders in awareness campaigns and ensuring vaccines are administered in familiar community settings. For example, using mobile clinics to deliver single-dose vaccines like AstraZeneca can improve accessibility and trust.
The consequences of hesitancy extend beyond COVID-19. In the Philippines, measles outbreaks surged in 2019 after vaccine confidence plummeted due to a dengue vaccine controversy. Similarly, polio eradication efforts in Pakistan and Afghanistan face resistance from communities suspicious of vaccination drives. To combat this, health organizations must prioritize transparency and cultural sensitivity. For parents, a simple tip: verify vaccine information through trusted sources like the WHO or local health ministries, not unverified social media posts.
Ultimately, addressing hesitancy requires a multi-faceted approach. Governments and NGOs must invest in clear, culturally tailored messaging, while tech platforms need to curb misinformation. For individuals, staying informed and encouraging open dialogue can make a difference. Vaccine hesitancy is not just a personal choice—it’s a global barrier to health equity. By understanding its roots and taking proactive steps, we can bridge the gap between availability and acceptance, ensuring vaccines reach their full potential.
How to Reschedule Your Walgreens Vaccine Appointment: A Step-by-Step Guide
You may want to see also
Explore related products






![]()
COVID-19 Vaccination Distribution Equity
As of the latest data, approximately 68% of the global population has received at least one dose of a COVID-19 vaccine, yet this figure masks stark disparities in distribution equity. High-income countries have administered over 150 doses per 100 people, while low-income countries struggle at around 20 doses per 100 people. This imbalance highlights a critical issue: vaccine equity is not just a moral imperative but a practical necessity for ending the pandemic. Without equitable distribution, new variants can emerge in under-vaccinated regions, prolonging the crisis for everyone.
Consider the logistical challenges in low-resource settings. Many countries lack the infrastructure to store mRNA vaccines, which require ultra-cold temperatures (as low as -70°C for Pfizer-BioNTech). In contrast, viral vector vaccines like AstraZeneca and Johnson & Johnson are more heat-stable, making them better suited for regions with limited refrigeration. However, wealthier nations often hoard these more accessible options, leaving poorer countries with fewer choices. For instance, COVAX, the global vaccine-sharing initiative, aimed to deliver 2 billion doses by 2021 but fell short due to supply shortages and export restrictions.
To address this inequity, a multi-faceted approach is essential. First, high-income countries must fulfill their dose-sharing pledges. For example, the U.S. promised 1.1 billion doses but has delivered only 46% of that commitment. Second, pharmaceutical companies should waive intellectual property rights temporarily, enabling local production in low-income regions. This step could increase global supply and reduce dependency on exports. Third, investing in local healthcare systems is crucial. Training healthcare workers and improving cold-chain logistics can ensure vaccines reach remote populations efficiently.
A comparative analysis reveals that countries with strong regional cooperation fare better. The African Union’s COVID-19 Vaccine Acquisition Task Team negotiated bulk purchases, securing 400 million doses for member states. In contrast, fragmented efforts in Southeast Asia led to slower vaccination rates. This example underscores the importance of collective action. Additionally, age-specific strategies are vital. Prioritizing elderly and immunocompromised populations in low-income countries can maximize the impact of limited doses, as these groups face higher mortality risks.
In conclusion, achieving COVID-19 vaccination equity requires more than goodwill—it demands actionable steps. High-income nations and pharmaceutical companies must prioritize global access over profit and nationalism. Practical measures, such as technology transfer and infrastructure support, can bridge the gap. Until every region has sufficient vaccine coverage, the world remains vulnerable. Equity is not just a goal; it’s the only path to a sustainable recovery.
Vaccines: Protecting Children from Preventable Harm
You may want to see also
Frequently asked questions
As of the latest data, approximately 70% of the global population has received at least one dose of a COVID-19 vaccine, though this varies widely by region.
High-income countries, particularly in North America, Western Europe, and parts of Asia (e.g., Singapore and the UAE), have the highest vaccination rates, often exceeding 80% of their populations fully vaccinated.
Approximately 60% of the world's population is considered fully vaccinated, though this figure includes only those who have completed their primary vaccine series.
Disparities arise due to unequal vaccine distribution, limited healthcare infrastructure, vaccine hesitancy, and logistical challenges in low-income countries, with some regions having vaccination rates below 20%.
Higher global vaccination rates reduce severe illness, hospitalizations, and deaths, but uneven distribution and emerging variants continue to pose challenges to ending the pandemic.












![International Certificate of Vaccination with Vinyl Document Holder - World Health Organization Bilingual Version [cards] World Health Organization [Jan 01, 2007]](https://m.media-amazon.com/images/I/61SHjBP1VYL._AC_UL320_.jpg)