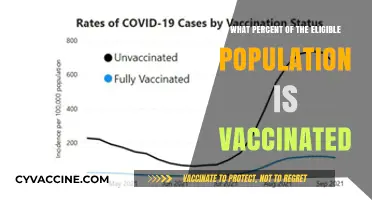
The question of what percent of the medical community is vaccinated is a critical topic in public health, as healthcare workers are on the front lines of disease prevention and treatment. Studies and surveys across various countries indicate that vaccination rates among medical professionals are generally high, often exceeding 90%, particularly for vaccines like influenza and COVID-19. These high rates reflect the medical community’s trust in vaccine efficacy and safety, as well as their commitment to protecting patients and preventing the spread of infectious diseases. However, vaccination rates can vary by region, specialty, and individual beliefs, highlighting the importance of ongoing education and addressing vaccine hesitancy within the healthcare workforce. Understanding these percentages is essential for maintaining public trust and ensuring the resilience of healthcare systems during outbreaks.
Explore related products






What You'll Learn
![]()
Global Vaccination Rates Among Healthcare Workers
Healthcare workers, the backbone of global health systems, have been at the forefront of the battle against infectious diseases, particularly during the COVID-19 pandemic. Their vaccination rates serve as a critical indicator of both their commitment to public health and the overall safety of healthcare environments. As of recent data, over 80% of healthcare workers worldwide have received at least one dose of a COVID-19 vaccine, with rates exceeding 90% in many high-income countries like the United States, Canada, and several European nations. However, disparities persist, with low- and middle-income countries (LMICs) reporting rates as low as 50% in some regions, such as parts of Africa and Southeast Asia. These variations highlight the influence of resource availability, vaccine access, and local health policies on vaccination uptake.
Analyzing these trends reveals a complex interplay of factors driving vaccination rates among healthcare workers. In high-income countries, robust healthcare infrastructure, widespread vaccine availability, and strong public health messaging have contributed to high uptake. For instance, in the U.S., mandates in many healthcare facilities requiring vaccination as a condition of employment have significantly boosted compliance. Conversely, in LMICs, logistical challenges, such as limited vaccine supply and distribution networks, coupled with vaccine hesitancy fueled by misinformation, have hindered progress. A study in India found that while 70% of healthcare workers were vaccinated, hesitancy was higher among younger staff and those in rural areas, underscoring the need for targeted interventions.
Persuasive efforts to increase vaccination rates must address both structural barriers and individual concerns. For LMICs, international collaboration to improve vaccine distribution and funding for local health systems is essential. The COVAX initiative, though facing challenges, remains a critical tool in this regard. Simultaneously, tailored communication strategies can combat hesitancy. In Brazil, for example, campaigns featuring trusted healthcare leaders and debunking myths in local languages have shown promise in increasing vaccine confidence. For healthcare workers, emphasizing the dual role of vaccination—protecting both themselves and vulnerable patients—can be a powerful motivator.
Comparatively, the success of vaccination campaigns in high-income countries offers lessons for global efforts. Mandatory vaccination policies, while controversial, have proven effective in achieving high coverage rates. However, such measures must be balanced with ethical considerations and alternatives like regular testing for those unable or unwilling to vaccinate. In contrast, voluntary campaigns in countries like Sweden, which achieved over 85% vaccination rates among healthcare workers through education and accessibility, demonstrate the power of trust-based approaches. These examples suggest that a one-size-fits-all strategy is insufficient; instead, solutions must be context-specific, addressing local needs and cultural nuances.
Practically, healthcare facilities can take proactive steps to improve vaccination rates. First, ensure easy access to vaccines by offering on-site clinics and flexible scheduling. Second, provide clear, evidence-based information to address concerns, particularly around vaccine safety and efficacy. Third, leverage peer influence by encouraging vaccinated staff to share their experiences. For instance, in the UK, hospitals that organized Q&A sessions with vaccinated colleagues saw higher uptake among hesitant staff. Finally, monitor and address disparities within the workforce, such as lower rates among support staff or specific age groups, through targeted outreach. By combining global insights with local action, the medical community can strive for equitable and comprehensive vaccination coverage.
The Booster Question: What Counts as Fully Vaccinated?
You may want to see also
Explore related products






![]()
Regional Variations in Medical Staff Vaccination
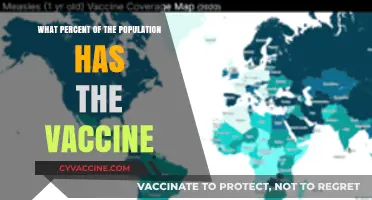
Vaccination rates among medical staff vary significantly across regions, influenced by factors such as local policies, cultural attitudes, and healthcare infrastructure. For instance, in North America, particularly the United States, vaccination rates among healthcare workers reached approximately 90% by early 2022, driven by mandates in many states and hospital systems. In contrast, parts of Africa and Southeast Asia report rates as low as 50-60%, often due to limited vaccine access and hesitancy fueled by misinformation. These disparities highlight the interplay between systemic support and community trust in shaping vaccination outcomes.
Consider the European landscape, where vaccination rates among medical professionals exhibit a distinct east-west divide. Countries like France and Germany boast rates exceeding 85%, supported by robust public health campaigns and mandatory vaccination policies in certain sectors. Conversely, nations such as Bulgaria and Romania struggle with rates below 50%, reflecting broader vaccine skepticism and weaker healthcare systems. This regional variation underscores the need for tailored strategies that address both logistical barriers and cultural perceptions.
Instructively, regions with high vaccination rates often share common practices: clear communication, accessible vaccination sites within healthcare facilities, and incentives for compliance. For example, in Australia, where over 95% of healthcare workers are vaccinated, hospitals implemented on-site vaccination clinics and provided paid time off for staff to receive doses. Conversely, in areas with lower rates, such as rural India, efforts to improve access—like mobile vaccination units—have shown promise but require sustained investment.
Persuasively, addressing regional disparities demands a dual approach: strengthening infrastructure and fostering trust. In Latin America, countries like Chile achieved over 90% vaccination rates among medical staff through a combination of early vaccine procurement and transparent public messaging. Meanwhile, in the Middle East, nations like Israel leveraged digital health records to streamline vaccination campaigns, achieving similar success. These examples illustrate that even in resource-constrained settings, strategic planning can overcome barriers.
Descriptively, the impact of regional variations extends beyond statistics, affecting patient safety and public health. In regions with lower vaccination rates, healthcare facilities face higher risks of outbreaks, compromising both staff and vulnerable patients. For instance, during the Delta variant surge, hospitals in parts of Eastern Europe struggled with staffing shortages due to unvaccinated workers contracting COVID-19. This underscores the critical role of regional vaccination equity in maintaining healthcare system resilience.
Mink Enteritis Vaccination: Protecting Raccoons from Deadly Parvovirus Infections
You may want to see also
Explore related products






![]()
Vaccine Hesitancy in the Medical Community
Vaccination rates among healthcare workers (HCWs) are surprisingly lower than expected, with estimates ranging from 70% to 90% depending on the region and vaccine type. For instance, during the COVID-19 pandemic, a 2021 study in the *Journal of the American Medical Association* found that while 96% of physicians reported being vaccinated, only 78% of nurses and 69% of healthcare support staff followed suit. This disparity highlights a critical issue: vaccine hesitancy exists even within the medical community, a group presumed to be uniformly pro-vaccination.
Consider the factors driving this hesitancy. For some HCWs, concerns about vaccine safety and side effects persist, despite overwhelming evidence of efficacy. For example, during the H1N1 pandemic, only 37% of U.S. HCWs received the vaccine, with many citing fear of adverse reactions. Others point to systemic issues, such as mistrust in pharmaceutical companies or government mandates, which can erode confidence even among medical professionals. A 2020 survey in *Vaccine* revealed that 14% of HCWs expressed skepticism about vaccine development processes, particularly expedited timelines.
Addressing hesitancy requires tailored strategies. First, education must go beyond generic messaging. Workshops that debunk myths with peer-reviewed data and involve trusted colleagues as advocates can be effective. For instance, a hospital in Ohio increased COVID-19 vaccination rates from 65% to 89% by hosting town halls led by infectious disease specialists. Second, policies should balance encouragement with flexibility. Mandates, while effective, can backfire if not paired with open dialogue. Offering paid time off for vaccination and recovery from side effects removes practical barriers and demonstrates institutional support.
Finally, the medical community must confront its own biases. HCWs are not immune to misinformation, and their hesitancy can influence public perception. A study in *The Lancet* found that 20% of unvaccinated individuals cited advice from healthcare acquaintances as a reason for their decision. By fostering transparency and accountability, medical institutions can ensure their staff become role models for vaccination, not sources of doubt.
In conclusion, vaccine hesitancy among HCWs is a nuanced issue requiring targeted interventions. By understanding the root causes, implementing evidence-based strategies, and promoting accountability, the medical community can strengthen its own vaccination rates and, in turn, public trust. After all, if healthcare workers lead by example, the ripple effect could be transformative.
Understanding the Rigorous Phases of Vaccine Approval and Safety
You may want to see also
Explore related products






![]()
Impact of Mandates on Medical Vaccination Rates
Vaccination mandates in the medical community have sparked both compliance and controversy, with data showing that regions with strict policies see significantly higher uptake rates. For instance, in New York State, where healthcare workers faced termination for non-compliance, vaccination rates surged to over 98% within months of the mandate’s implementation. This contrasts sharply with areas lacking such policies, where rates often plateau below 80%. The disparity underscores the direct impact of mandates on behavior, particularly in high-stakes environments where patient safety is paramount.
From an analytical standpoint, mandates serve as a dual-edged tool. On one hand, they eliminate ambiguity, ensuring near-universal protection against vaccine-preventable diseases. On the other, they risk alienating a minority of workers, potentially exacerbating staffing shortages in already strained healthcare systems. A study published in *JAMA* found that while mandates increased vaccination rates by an average of 20%, they also led to a 3-5% workforce reduction in some facilities. This trade-off demands careful consideration, balancing public health imperatives with operational feasibility.
Persuasively, mandates align with the ethical duty of healthcare providers to "first, do no harm." Unvaccinated staff pose a risk not only to themselves but also to immunocompromised patients, who may not mount a full immune response even after vaccination. For example, a single unvaccinated nurse working in an oncology ward could inadvertently expose vulnerable patients to preventable illnesses like influenza or COVID-19. Mandates, therefore, act as a safeguard, prioritizing collective well-being over individual choice in a profession built on trust and responsibility.
Comparatively, countries with voluntary vaccination programs often struggle to achieve herd immunity within their medical ranks. In Sweden, where mandates are absent, healthcare worker vaccination rates for COVID-19 hover around 85%, leaving gaps that could facilitate outbreaks. Conversely, France’s mandate-driven approach achieved a 99% vaccination rate among healthcare workers, demonstrating the efficacy of policy enforcement. This comparison highlights how mandates can bridge the gap between voluntary participation and public health goals.
Practically, implementing mandates requires a nuanced approach. Facilities should pair mandates with education campaigns addressing vaccine hesitancy, offer paid time off for vaccination and side effects, and provide accessible on-site clinics. For example, Mayo Clinic’s mandate included a six-week grace period, during which employees could attend informational sessions and receive the vaccine without fear of immediate repercussions. Such measures foster compliance while minimizing resentment, ensuring mandates are seen as protective rather than punitive.
Adult Vaccination Recommendations: Essential Immunizations for Lifelong Health
You may want to see also
Explore related products






![]()
Vaccination Rates by Medical Specialization
Vaccination rates among medical professionals vary significantly by specialization, reflecting differences in exposure risk, patient interaction, and professional culture. For instance, infectious disease specialists and emergency room physicians, who frequently encounter vaccine-preventable diseases, report vaccination rates exceeding 95%. These high rates are not coincidental; they are a direct response to the heightened risk of exposure to pathogens like influenza, measles, and COVID-19. In contrast, specialties such as dermatology or radiology, where patient contact is less frequent or involves lower-risk conditions, often report rates closer to 80-85%. This disparity underscores the influence of workplace environment on vaccination behavior.
Consider the role of patient populations in shaping these trends. Pediatricians, for example, achieve near-universal vaccination rates, often at 98% or higher, due to their constant interaction with vulnerable, unvaccinated children. This high compliance is not just about self-protection but also about preventing disease transmission to immunocompromised patients. Conversely, psychiatrists, who primarily treat patients with mental health conditions, may have lower vaccination rates, around 80%, as their practice settings typically involve minimal physical contact and lower infection risk. These variations highlight how specialization-specific risks drive vaccination decisions.
To improve vaccination rates across all medical specializations, targeted strategies are essential. For high-risk specialties like internal medicine or oncology, where vaccination is critical due to immunocompromised patients, mandates and regular reminders have proven effective. For example, hospitals requiring annual flu shots for staff in these departments see compliance rates rise to 95% or higher. In lower-risk specialties, such as pathology or radiology, educational campaigns emphasizing herd immunity and community protection can bridge the gap. Offering convenient access to vaccines, such as on-site clinics during work hours, further removes barriers to compliance.
A comparative analysis reveals that specializations with strong professional organizations tend to have higher vaccination rates. For instance, the American College of Obstetricians and Gynecologists (ACOG) actively promotes vaccination for its members, resulting in over 90% compliance among OB/GYNs. This success suggests that peer influence and organizational advocacy play a pivotal role. In contrast, specialties with less centralized leadership, such as general surgery, may lag behind, with rates around 85%. Strengthening professional networks and incorporating vaccination advocacy into specialty-specific training could address these disparities.
Finally, understanding these variations is crucial for policymakers and healthcare administrators aiming to boost overall medical community vaccination rates. Tailoring interventions to the unique needs and risks of each specialization can maximize impact. For example, offering COVID-19 booster shots during surgical conferences for surgeons or providing flu vaccine clinics at dermatology meetings could increase participation. By recognizing the distinct challenges and cultures of each medical specialization, the healthcare system can move closer to universal vaccination among its workforce, ultimately enhancing patient safety and public health.
Post-Vaccine Symptoms: When to Isolate and What to Do
You may want to see also
Frequently asked questions
As of recent data, over 90% of healthcare workers in many countries, including the United States, are fully vaccinated against COVID-19.
Generally, vaccination rates are high across all medical professions, but studies show doctors and physicians often have slightly higher vaccination rates compared to nurses and support staff.
Yes, vaccination rates among healthcare workers vary by region, with higher rates in areas with strong public health infrastructure and lower rates in regions with vaccine hesitancy or limited access.
The medical community typically has a significantly higher vaccination rate than the general population, reflecting their trust in scientific evidence and the importance of protecting patients.
While most specialties have high vaccination rates, some studies suggest that certain fields, such as alternative medicine practitioners, may have slightly lower vaccination rates compared to mainstream medical specialties.