Vaccine allergies are a rare but important concern in public health, prompting questions about the percentage of the population affected. While vaccines are generally safe and well-tolerated, a small subset of individuals may experience allergic reactions, typically due to components like gelatin, egg proteins, or preservatives. Studies suggest that severe allergic reactions to vaccines are extremely uncommon, occurring in approximately 1 in a million doses. Mild reactions, such as localized swelling or rash, are more frequent but still rare. Overall, less than 1% of the population is estimated to have a true allergy to vaccine components, making it a minimal but significant consideration in immunization programs. Understanding this prevalence is crucial for healthcare providers to ensure safe vaccination practices and address public concerns effectively.
Explore related products






What You'll Learn
![]()
Prevalence of Vaccine Allergies
Vaccine allergies are rare, affecting less than 1% of the population. This low prevalence is a critical factor in public health, as it ensures that the vast majority of individuals can safely receive vaccinations without adverse reactions. The rarity of these allergies is often attributed to the rigorous testing and purification processes vaccines undergo before approval. For instance, common vaccines like the flu shot or MMR (measles, mumps, rubella) are designed to minimize the presence of potential allergens, such as egg proteins or preservatives, which are often implicated in allergic responses.
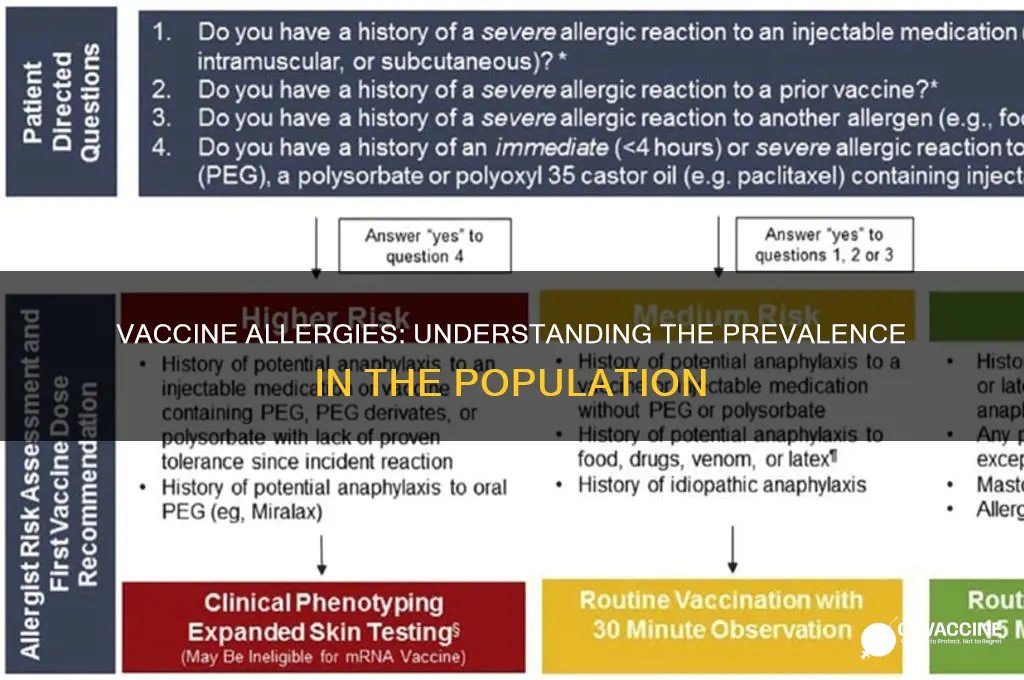
Understanding the demographics most at risk for vaccine allergies is essential for healthcare providers. Children and adults with a history of severe allergies, particularly to components like gelatin or antibiotics, may face a slightly higher risk. For example, gelatin, used as a stabilizer in some vaccines, has been linked to anaphylaxis in rare cases. Similarly, individuals with a history of egg allergies were once advised to avoid certain vaccines, but updated guidelines now indicate that most egg-allergic individuals can safely receive vaccines like the flu shot, often without special precautions.
Practical steps can mitigate the risk of allergic reactions during vaccination. Healthcare providers should always review a patient’s medical history before administering a vaccine, paying special attention to past allergic reactions. In cases where a risk is identified, skin testing or graded challenge doses may be considered under medical supervision. For instance, a graded challenge involves administering a small portion of the vaccine first, waiting to observe for reactions, and then proceeding with the full dose if no symptoms occur. This method has proven effective in safely vaccinating high-risk individuals.
Comparatively, the risk of complications from vaccine-preventable diseases far outweighs the risk of an allergic reaction. For example, measles can lead to pneumonia, encephalitis, and even death, while the risk of a severe allergic reaction to the MMR vaccine is approximately 1 in a million doses. This stark contrast underscores the importance of vaccination, even for those with potential allergy concerns. Public health campaigns should emphasize this balance, encouraging individuals to consult healthcare providers rather than avoiding vaccines altogether.
In conclusion, while vaccine allergies exist, their prevalence is extremely low, and manageable strategies are available for those at risk. By focusing on individualized care, healthcare providers can ensure that the benefits of vaccination are accessible to nearly everyone. This approach not only protects individuals but also contributes to herd immunity, safeguarding communities from preventable diseases.
Understanding Your Rights: Legally Declining Vaccines as an Adult
You may want to see also
Explore related products






![]()
Common Vaccine Allergens
Vaccine allergies, though rare, are a critical concern for a small percentage of the population. Estimates suggest that severe allergic reactions to vaccines occur in approximately 1 in 760,000 doses administered. While this figure is reassuringly low, understanding the common allergens in vaccines is essential for identifying and managing potential risks. These allergens can range from components of the vaccine itself to residual substances from the manufacturing process.
One of the most well-known vaccine allergens is egg protein, commonly found in influenza vaccines. Since many flu vaccines are grown in chicken eggs, trace amounts of egg protein may remain in the final product. For individuals with severe egg allergies, this can pose a risk, though studies show that most can safely receive the flu vaccine under medical supervision. The CDC recommends that people with egg allergies who have only experienced hives after egg exposure can receive any licensed, recommended influenza vaccine. However, those with a history of severe reactions should be vaccinated in a medical setting, supervised by a healthcare provider who can manage anaphylaxis.
Another common allergen is latex, used in the stoppers of some vaccine vials or prefilled syringes. Latex allergy affects approximately 6% of the population, particularly healthcare workers and individuals with spina bifida. Symptoms can range from mild skin irritation to life-threatening anaphylaxis. To mitigate this risk, many vaccines now use latex-free packaging, and healthcare providers should verify the product’s latex status before administration. Patients with known latex allergies should inform their healthcare provider to ensure a safe vaccination process.
Gelatin, a stabilizer in vaccines like MMR (measles, mumps, rubella) and varicella (chickenpox), is another potential allergen. Gelatin allergy is rare but can cause severe reactions, including anaphylaxis. The risk is estimated at 1 in 2 million doses. Individuals with a history of gelatin allergy should be closely monitored during vaccination. Alternative vaccines without gelatin may be considered, though options are limited. Consultation with an allergist is recommended to weigh the risks and benefits.
Finally, antibiotics such as neomycin or polymyxin B, used to prevent bacterial contamination during vaccine production, can trigger allergic reactions in sensitive individuals. These reactions are rare but can occur even in trace amounts. Patients with a history of antibiotic allergies should disclose this to their healthcare provider, who may recommend skin testing or other precautions before vaccination.
In summary, while vaccine allergies are uncommon, awareness of common allergens like egg protein, latex, gelatin, and antibiotics is crucial for safe vaccination practices. Healthcare providers and patients must communicate openly about allergy histories to ensure appropriate precautions are taken. With proper management, the vast majority of individuals, even those with known allergies, can safely receive vaccines.
Healthcare Heroes: Vaccination Rates Among Doctors and Nurses Revealed
You may want to see also
Explore related products





![]()
Symptoms of Vaccine Allergies
Vaccine allergies, though rare, manifest through distinct symptoms that require immediate attention. These reactions typically occur within minutes to hours after vaccination and are primarily mediated by the immune system’s response to specific components in the vaccine, such as gelatin, egg protein, or preservatives like neomycin. Recognizing these symptoms is crucial for timely intervention and prevention of severe outcomes.
Immediate Symptoms to Watch For:
Anaphylaxis is the most severe allergic reaction, characterized by rapid onset of symptoms such as hives, swelling of the face or throat, difficulty breathing, rapid heartbeat, dizziness, or loss of consciousness. For example, a study published in *JAMA* found that anaphylaxis occurs in approximately 1.3 cases per million vaccine doses administered. Less severe but still concerning symptoms include persistent itching, redness, or swelling at the injection site that spreads to other parts of the body. These reactions often appear within 15–30 minutes post-vaccination, emphasizing the importance of monitoring individuals during this window.
Delayed Reactions and Their Implications:
While less common, delayed allergic reactions can occur 24–48 hours after vaccination. These may include fever, joint pain, or widespread skin rashes. For instance, the MMR vaccine has been associated with mild, delayed rashes in 5–15% of recipients, though these are typically non-allergic in nature. However, persistent or worsening symptoms warrant medical evaluation to rule out an allergic response.
High-Risk Groups and Precautions:
Individuals with a history of severe allergies, particularly to vaccine components, are at higher risk. For example, those allergic to eggs should consult a healthcare provider before receiving vaccines like the flu shot, which is often grown in egg cultures. Similarly, gelatin-sensitive individuals may react to vaccines such as the MMR or varicella vaccine. Precautionary measures include administering vaccines in medical settings equipped to handle emergencies and ensuring access to epinephrine auto-injectors for at-risk patients.
Practical Tips for Managing Vaccine Allergies:
If an allergic reaction is suspected, seek medical attention immediately. Mild symptoms like localized swelling or redness can often be managed with antihistamines, but severe reactions require epinephrine. Always disclose any known allergies to healthcare providers before vaccination. For children, parents should monitor for unusual behavior, such as lethargy or persistent crying, which could indicate a reaction. Lastly, keeping a record of previous vaccine responses can aid in identifying patterns and guiding future immunization decisions.
Understanding and responding to vaccine allergy symptoms is essential for ensuring safe immunization practices. While such reactions are rare, their potential severity underscores the need for vigilance and preparedness.
Should Vaccinations Be Mandatory in the United States? A Debate
You may want to see also
Explore related products





![]()
Risk Factors for Reactions
Vaccine allergies are rare, affecting less than 1 in 1 million people. However, understanding risk factors for reactions is crucial for safe immunization. Certain individuals face higher risks due to specific conditions or histories, making personalized assessment essential before vaccination.
Identifying High-Risk Groups: A Checklist
Individuals with a history of severe allergic reactions (anaphylaxis) to vaccine components—such as gelatin, egg protein, or specific antibiotics—require careful evaluation. For example, MMR vaccines contain trace egg protein, posing a risk to those with severe egg allergies. Similarly, some flu vaccines use gelatin as a stabilizer, which has been linked to rare anaphylactic cases. Pregnant individuals, those with compromised immune systems, and infants under 6 months (due to underdeveloped immune responses) also fall into higher-risk categories.
Dosage and Administration: Mitigating Risks
Vaccine dosage and administration techniques play a pivotal role in minimizing reactions. For instance, splitting doses or using lower concentrations for at-risk individuals can reduce adverse effects. Healthcare providers often administer vaccines in controlled settings, ensuring immediate access to epinephrine and other emergency treatments. Patients with a history of reactions may undergo graded dosing, starting with a small test dose before proceeding with the full amount.
Practical Tips for At-Risk Individuals
If you suspect a vaccine allergy, consult an allergist for skin testing or blood tests to identify specific triggers. Always disclose your full medical history, including past reactions, to healthcare providers. After vaccination, remain at the clinic for 15–30 minutes for monitoring, especially if you’re high-risk. Carry an epinephrine auto-injector if prescribed, and wear a medical alert bracelet to inform caregivers of your allergy.
The Takeaway: Balancing Risks and Benefits
While vaccine reactions are exceedingly rare, awareness of risk factors empowers individuals and healthcare providers to make informed decisions. Personalized risk assessment, careful administration, and proactive monitoring ensure that the vast majority can safely benefit from immunization, even those with heightened susceptibility to reactions.
The Evolution of Vaccines: A Journey Before the Polio Breakthrough
You may want to see also
Explore related products






![]()
Statistics by Age Group
Vaccine allergies, though rare, exhibit distinct patterns across age groups, influenced by immune system maturity, exposure history, and vaccine formulations. Pediatric populations (0–17 years) account for the majority of reported cases, with anaphylaxis rates estimated at 1.31 cases per million doses for measles-mumps-rubella (MMR) vaccines and 5.1 cases per million for the diphtheria-tetanus-pertussis (DTaP) vaccine. These reactions are often linked to excipients like gelatin or yeast, rather than the antigens themselves. For instance, gelatin in MMR vaccines has been implicated in 1–2% of pediatric anaphylaxis cases, prompting its removal in newer formulations. Parents should monitor children for symptoms like hives, swelling, or respiratory distress within 30 minutes post-vaccination and report reactions to healthcare providers immediately.
In contrast, adolescents and young adults (18–39 years) show lower overall allergy rates but increased sensitivity to specific vaccines, such as the human papillomavirus (HPV) vaccine. Studies indicate anaphylaxis rates of 1.7 cases per million doses for HPV vaccines, with reactions often tied to latex in prefilled syringes or aluminum adjuvants. This age group also faces higher risks with mRNA COVID-19 vaccines, where polyethylene glycol (PEG) allergies account for 2–3 cases per 100,000 doses. Individuals with a history of severe allergies should undergo pre-vaccination screening, including PEG allergy testing, and receive doses in clinical settings equipped to manage anaphylaxis.
Among middle-aged adults (40–64 years), vaccine allergy statistics are skewed by influenza vaccines, which account for 70% of reported reactions in this demographic. Egg-allergic individuals, comprising 0.2–2% of this age group, were historically cautioned against inactivated flu vaccines due to egg protein residues. However, updated guidelines confirm that all influenza vaccines are safe for egg-allergic patients, with no increased risk of anaphylaxis. Adults receiving high-dose or adjuvanted flu vaccines should be observed for 15–30 minutes post-injection, as these formulations carry slightly elevated reaction risks.
Elderly populations (65+ years) exhibit the lowest vaccine allergy rates, with anaphylaxis occurring in approximately 0.1–0.5 cases per million doses across all vaccines. However, this group faces unique challenges due to age-related immune decline and comorbidities. For example, shingles vaccines (e.g., Shingrix) contain higher concentrations of adjuvants, which may exacerbate local reactions like pain or swelling in 15–20% of recipients. Elderly patients should prioritize hydration and use cold compresses post-vaccination to mitigate discomfort. Caregivers must differentiate between allergic reactions and age-related conditions like dizziness or fatigue, ensuring prompt medical evaluation when symptoms persist.
Across all age groups, proactive measures can minimize vaccine allergy risks. These include reviewing medical histories for prior reactions, inquiring about specific vaccine components, and ensuring access to epinephrine auto-injectors in high-risk cases. Healthcare providers should adhere to age-specific dosing guidelines—for instance, reducing antigen loads in frail elderly patients or using alternative formulations for excipient-sensitive individuals. By tailoring vaccination strategies to age-related vulnerabilities, public health initiatives can enhance safety while maintaining immunization efficacy.
Air Travel and Vaccination: What's the Connection?
You may want to see also
Frequently asked questions
Severe allergic reactions to vaccines are extremely rare, occurring in approximately 1.3 cases per 1 million vaccine doses administered.
No, vaccine allergies in children are very uncommon. Studies suggest that less than 1% of children experience allergic reactions to vaccines, with most cases being mild.
The flu vaccine and vaccines containing gelatin (e.g., MMR, varicella) are more frequently linked to allergic reactions, though such reactions remain rare, affecting less than 0.1% of recipients.