The percentage of individuals who remain unvaccinated against measles varies significantly across regions and demographics, influenced by factors such as access to healthcare, vaccine hesitancy, and public health policies. While global vaccination efforts have reduced measles cases by 73% since 2000, pockets of unvaccinated populations persist, leading to outbreaks in communities with low immunization rates. In some countries, vaccine skepticism, misinformation, and logistical challenges contribute to higher percentages of unvaccinated individuals, particularly in low-income areas or among specific cultural or religious groups. Understanding these disparities is crucial for addressing gaps in immunity and preventing the resurgence of this highly contagious disease.
Explore related products






What You'll Learn
![]()
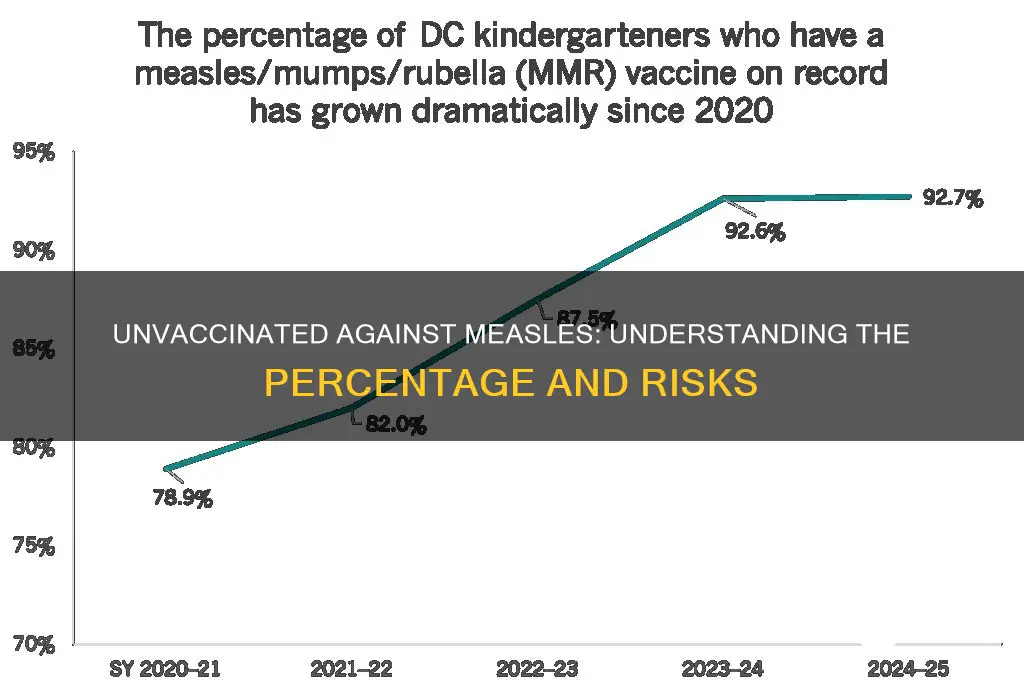
Global vaccination rates for measles
Measles, a highly contagious virus, remains a significant global health concern despite the availability of an effective vaccine. As of recent data, approximately 10% of the global population remains unvaccinated against measles, leaving millions vulnerable to outbreaks. This gap in immunity is not uniform; it varies widely by region, with low-income countries often bearing the brunt of the disease due to limited access to vaccines. For instance, in sub-Saharan Africa, vaccination rates can be as low as 60%, compared to over 90% in many high-income nations. This disparity underscores the urgent need for targeted interventions to bridge the immunization gap.
Analyzing the reasons behind low vaccination rates reveals a complex interplay of logistical, economic, and cultural factors. In remote or conflict-affected areas, vaccine distribution is often hindered by poor infrastructure and political instability. Additionally, misinformation and vaccine hesitancy play a significant role, particularly in regions where distrust of healthcare systems or conspiracy theories thrive. For example, in some European countries, measles outbreaks have been linked to declining vaccination rates driven by anti-vaccine movements. Addressing these challenges requires not only improving access to vaccines but also robust public health education campaigns to rebuild trust.
From a practical standpoint, increasing global measles vaccination rates demands a multi-faceted approach. Strengthening healthcare infrastructure in low-resource settings is critical, including training healthcare workers and ensuring a reliable cold chain for vaccine storage. International organizations like the World Health Organization (WHO) and Gavi, the Vaccine Alliance, play a pivotal role in funding and coordinating these efforts. For parents and caregivers, understanding the measles vaccine schedule is essential: the first dose is typically given at 12–15 months of age, followed by a second dose at 4–6 years. Adhering to this schedule provides over 97% protection against the virus.
Comparatively, regions with high vaccination rates, such as the Americas, have demonstrated the effectiveness of sustained immunization campaigns. However, even in these areas, pockets of under-vaccinated populations can lead to outbreaks, as seen in recent years in the United States. This highlights the importance of maintaining high coverage rates and addressing vaccine hesitancy through evidence-based communication strategies. By learning from successful models and adapting them to local contexts, global efforts can move closer to the WHO’s goal of 95% measles vaccination coverage, a threshold necessary for herd immunity.
In conclusion, the 10% of the global population not vaccinated against measles represents both a challenge and an opportunity. Closing this gap requires addressing systemic barriers, combating misinformation, and ensuring equitable access to vaccines. With coordinated global action and community engagement, it is possible to eliminate measles as a public health threat, saving millions of lives and preventing unnecessary suffering. The tools exist; what’s needed now is the collective will to deploy them effectively.
Unvaccinated Autism Cases: Exploring the Link and Dispelling Myths
You may want to see also
Explore related products






![]()
Reasons for vaccine hesitancy worldwide
Vaccine hesitancy, particularly for measles, is a complex phenomenon with roots in cultural, historical, and psychological factors. One significant reason for hesitancy is misinformation and distrust in institutions. The rise of social media has amplified false claims about vaccine safety, such as the debunked link between the MMR (measles, mumps, rubella) vaccine and autism. For instance, a 2019 study found that countries with higher social media usage saw sharper declines in vaccine confidence. In the Philippines, measles vaccination rates dropped from 88% in 2008 to 69% in 2017, partly due to a controversial dengue vaccine scandal that eroded public trust in all vaccines. This distrust is not just about the information itself but also about the sources—when governments or pharmaceutical companies are perceived as untrustworthy, their health recommendations are often rejected.
Another critical factor is cultural and religious beliefs, which vary widely across regions. In some communities, vaccines are viewed as interfering with natural immunity or as a product of Western influence, conflicting with traditional practices. For example, in parts of Nigeria, polio vaccination campaigns faced resistance due to rumors that vaccines were a plot to sterilize Muslim populations. Similarly, in Japan, historical mandates and a preference for holistic health approaches have contributed to lower vaccination rates. These beliefs are deeply ingrained and often require sensitive, culturally tailored interventions to address. Public health strategies must respect these perspectives while providing accurate, localized information to bridge the gap.
Logistical barriers also play a significant role in vaccine hesitancy, particularly in low- and middle-income countries. Access to vaccines is not universal, and challenges like transportation, cost, and availability of healthcare workers can prevent individuals from getting vaccinated. For measles, which requires two doses (typically at 12–15 months and 4–6 years), incomplete vaccination is common. In rural areas of India, for instance, only 62% of children receive both doses due to poor infrastructure and lack of awareness. Even in high-income countries, marginalized communities face similar issues. Addressing these barriers requires investment in healthcare systems, mobile clinics, and public education campaigns to ensure vaccines are accessible and affordable for all.
Finally, individual risk perception shapes vaccine hesitancy. When measles is perceived as a mild childhood illness, the urgency to vaccinate diminishes. However, measles is highly contagious, with one infected person spreading it to 9 out of 10 unvaccinated individuals. Complications like pneumonia and encephalitis can be life-threatening, particularly for children under 5. Yet, in countries like the U.S., where measles was declared eliminated in 2000, younger generations have no firsthand experience of its severity, leading to complacency. Public health messaging must emphasize the real risks of measles and the collective benefit of herd immunity, which requires 95% vaccination coverage to protect vulnerable populations.
In summary, vaccine hesitancy for measles is a multifaceted issue requiring tailored solutions. Combating misinformation, respecting cultural beliefs, improving access, and raising awareness of measles’ dangers are all critical steps. By addressing these factors, global vaccination rates can rise, reducing outbreaks and protecting public health.
Step-by-Step Guide: Registering for Vaccines at Texas Motor Speedway
You may want to see also
Explore related products





![]()
Regional disparities in measles immunization
Measles immunization rates vary dramatically across regions, with some areas achieving near-universal coverage while others lag far behind. In high-income countries like the United States and the United Kingdom, vaccination rates typically exceed 90%, driven by robust healthcare infrastructure and public awareness campaigns. However, in low-income regions such as parts of sub-Saharan Africa and Southeast Asia, coverage often drops below 70%, leaving millions of children vulnerable to outbreaks. This disparity is not merely a statistic—it translates to real-world consequences, with over 90% of measles deaths occurring in low-resource settings where vaccine access is limited.
To address these gaps, understanding the root causes is essential. In some regions, logistical challenges dominate, such as inadequate cold chain storage for vaccines or poor transportation networks. For instance, in rural areas of Ethiopia, only 58% of children receive the recommended two doses of the measles vaccine by age 2, compared to 85% in urban centers. Other barriers include cultural misconceptions and distrust of vaccines, as seen in parts of Europe where anti-vaccine movements have taken hold, leading to localized outbreaks. In France, for example, vaccine hesitancy contributed to a 30% increase in measles cases between 2016 and 2019.
Practical solutions must be tailored to regional needs. In low-resource settings, strengthening healthcare systems through funding and training is critical. UNICEF’s outreach programs in Nigeria, which combine door-to-door vaccination drives with community education, have increased coverage by 15% in targeted areas. In regions where hesitancy is the primary barrier, public health campaigns must counter misinformation with evidence-based messaging. For instance, the World Health Organization’s *Vaccine Safety Net* initiative provides credible resources in multiple languages to combat myths.
Comparing successful models offers valuable insights. Rwanda, despite being a low-income country, achieves a 93% measles vaccination rate through its integrated health system, which includes routine immunization clinics and mobile outreach. Contrast this with Ukraine, where political instability and misinformation led to a vaccination rate of just 42% in 2016, triggering Europe’s largest measles outbreak in decades. These examples highlight the importance of political commitment and community engagement in overcoming regional disparities.
Ultimately, closing the immunization gap requires a multi-faceted approach. Policymakers must prioritize equitable vaccine distribution, while healthcare providers should focus on building trust and accessibility. Parents and caregivers can play a role by staying informed and adhering to vaccination schedules—typically, the first dose at 12 months and the second between ages 4 and 6. By addressing regional disparities head-on, we can move closer to the global goal of measles eradication, ensuring no child is left unprotected.
Understanding Rabies Vaccines: Live, Modified Live, or Killed?
You may want to see also
Explore related products


![]()
Impact of misinformation on vaccination rates
Misinformation has become a silent epidemic, eroding trust in vaccines and directly contributing to the rise in unvaccinated populations. For measles, a highly contagious disease preventable by a safe and effective vaccine, misinformation campaigns have led to a resurgence in outbreaks globally. The MMR (measles, mumps, rubella) vaccine, typically administered in two doses—the first at 12-15 months and the second at 4-6 years—has seen declining uptake in regions where false claims about its safety and efficacy spread unchecked. In the U.S., for instance, states with relaxed vaccine exemption policies have seen measles cases triple in recent years, with unvaccinated individuals accounting for over 90% of infections. This trend underscores how misinformation doesn’t just skew perceptions—it endangers lives.
Consider the mechanics of how misinformation spreads: a single viral post or video can reach millions, often bypassing fact-checking mechanisms. Anti-vaccine narratives frequently exploit parental fears, falsely linking vaccines to autism or other conditions, despite decades of research disproving such claims. For example, a debunked 1998 study by Andrew Wakefield continues to fuel skepticism, even though it was retracted and its author discredited. This persistence highlights the challenge: misinformation sticks because it preys on emotions, while corrections often fail to resonate with the same intensity. The result? In some communities, vaccination rates for measles have dropped below the 95% threshold needed for herd immunity, leaving vulnerable populations—infants, the immunocompromised, and those unable to receive the vaccine—at risk.
To combat this, public health strategies must evolve. First, healthcare providers should proactively address parental concerns during well-child visits, emphasizing the rigorous testing vaccines undergo and the negligible risks compared to the diseases they prevent. Second, social media platforms must prioritize algorithmic changes to amplify credible sources, such as the CDC or WHO, over misleading content. Third, community-based initiatives can play a role by engaging local leaders to dispel myths and share personal vaccination stories. For instance, in Samoa, a 2019 measles outbreak that killed 83 people was followed by a successful campaign that increased vaccination rates from 31% to 94% in months, demonstrating the power of targeted, culturally sensitive interventions.
The takeaway is clear: misinformation isn’t just a nuisance—it’s a public health crisis. Its impact on measles vaccination rates serves as a cautionary tale for other preventable diseases. By understanding how misinformation spreads and implementing multi-faceted solutions, we can rebuild trust and protect communities. The MMR vaccine remains one of the most studied medical products in history, with billions of doses administered safely. Let’s ensure that facts, not fear, guide decisions—because the cost of inaction is measured in outbreaks, hospitalizations, and lives lost.
Herpes Simplex 1 & 2: Current Vaccine Developments and Hope
You may want to see also
![]()
Unvaccinated populations by age group
The distribution of unvaccinated populations for measles varies significantly across age groups, reflecting differences in historical vaccination policies, access to healthcare, and societal attitudes. Among infants under 12 months, non-vaccination is nearly universal for measles, as the first dose of the MMR (Measles, Mumps, Rubella) vaccine is typically administered between 12 and 15 months of age. This age group relies on herd immunity for protection, making it critical that surrounding populations maintain high vaccination rates. In contrast, children aged 1–4 years show lower unvaccinated rates in countries with robust immunization programs, often below 5%, due to routine vaccination schedules. However, in regions with disrupted healthcare systems or vaccine hesitancy, this figure can spike to 20% or higher, leaving young children vulnerable to outbreaks.
For school-aged children (5–15 years), unvaccinated rates diverge sharply between high-income and low-income countries. In the U.S. and Europe, non-vaccination in this age group is often driven by parental choice, with rates ranging from 1–5% in some states or regions. In low-income nations, logistical challenges and vaccine shortages can push unvaccinated rates to 10–30%, despite school-entry vaccination requirements. Adolescents and young adults (16–29 years) represent a growing concern, particularly in high-income countries. Many in this group missed the second MMR dose, recommended between 4 and 6 years of age, due to gaps in healthcare access or misinformation. In the U.S., for example, approximately 8–10% of young adults lack full measles immunity, creating a reservoir for potential outbreaks in social or educational settings.
Among adults over 30, unvaccinated rates are influenced by birth cohort. Those born before 1957 are presumed immune due to likely measles exposure, while individuals aged 30–60 may have received only one dose of the vaccine, which is 95% effective but leaves a small gap in immunity. Adults under 30 are more likely to be unvaccinated or under-vaccinated due to shifting vaccination policies and rising hesitancy. Globally, older adults (65+) often have natural immunity, but those in regions with low historical measles circulation may remain susceptible, particularly if they avoided infection and never received the vaccine.
To address these disparities, targeted strategies are essential. For infants, strengthening herd immunity through community vaccination is paramount. School-based catch-up campaigns can reduce unvaccinated rates among children, while educational initiatives aimed at parents can combat hesitancy. Young adults benefit from workplace or university-based vaccination drives, and adults of all ages should be encouraged to verify their immunity status through antibody testing or receive a booster dose if needed. By tailoring interventions to the unique challenges of each age group, public health efforts can close immunity gaps and prevent measles resurgence.
Rabies Treatment: Can It Also Vaccinate You?
You may want to see also
Frequently asked questions
As of recent data, approximately 10-15% of the global population remains unvaccinated for measles, though this varies widely by region.
About 2-3% of children in the United States are not vaccinated for measles, primarily due to exemptions or lack of access to healthcare.
In low-income countries, up to 30-40% of the population may not be vaccinated for measles due to limited healthcare infrastructure and vaccine availability.
It is estimated that 20-25% of adults worldwide are not vaccinated for measles, either due to lack of childhood vaccination or waning immunity.
In Europe, approximately 5-10% of the population is not vaccinated for measles, with higher rates in certain countries due to vaccine hesitancy or gaps in immunization programs.