Japanese encephalitis (JE) vaccine is typically administered through an intramuscular injection, with the preferred site being the deltoid muscle in the upper arm for adults and older children. In infants and younger children, the anterolateral aspect of the thigh is often chosen due to the smaller muscle mass in the arm. This route ensures optimal absorption and immune response, as the vaccine is delivered directly into the muscle tissue. Proper injection technique is crucial to minimize discomfort and potential side effects, making it essential for healthcare providers to follow guidelines for the appropriate administration of the JE vaccine.
Explore related products

$11.93 $21.99





What You'll Learn
- Injection Site: Typically administered in the deltoid muscle of the upper arm
- Vaccine Administration: Given intramuscularly, not subcutaneously, for optimal immune response
- Age-Specific Sites: Children may receive it in the thigh muscle instead of the arm
- Pain Management: Applying ice or numbing cream can reduce injection site discomfort
- Post-Injection Care: Avoid heavy arm use for 24 hours to minimize soreness
![]()
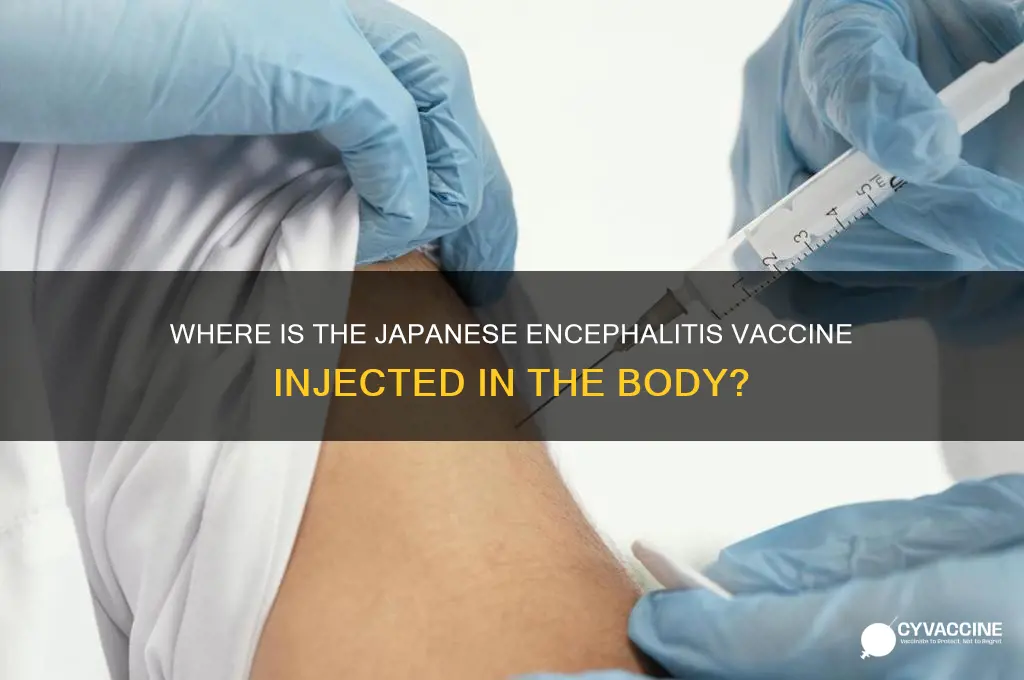
Injection Site: Typically administered in the deltoid muscle of the upper arm
The Japanese encephalitis (JE) vaccine is typically administered in the deltoid muscle of the upper arm, a site chosen for its accessibility and the muscle’s ability to facilitate robust immune response. This injection location aligns with global vaccination standards, ensuring consistency in vaccine delivery across healthcare settings. For adults and children aged 2 years and older, the deltoid muscle is the preferred site due to its size and ease of access, minimizing discomfort during administration. The vaccine, often given as a 0.5 mL dose, is delivered intramuscularly to ensure the antigen is absorbed efficiently, triggering a strong immune reaction. Healthcare providers are trained to identify the correct deltoid location, typically the thickest part of the arm, to avoid injury to nerves or blood vessels.
Administering the JE vaccine in the deltoid muscle follows a precise technique to maximize efficacy and minimize side effects. The injector should stretch the skin taut and insert the needle at a 90-degree angle, ensuring it penetrates the muscle tissue fully. For children aged 2 to 3 years, a smaller needle (e.g., 22–25 gauge) may be used to accommodate their smaller muscle mass. After injection, gentle pressure can be applied to the site, but rubbing is discouraged, as it may cause irritation. Common side effects, such as soreness or swelling, are generally mild and resolve within a few days. Proper technique not only enhances vaccine uptake but also reduces the risk of local adverse reactions.
Comparatively, the deltoid muscle is favored over other injection sites, such as the thigh or buttocks, for JE vaccination due to its lower risk of tissue damage and higher patient tolerance. The vastus lateralis muscle in the thigh is sometimes used for infants or individuals with insufficient deltoid mass, but this is less common for JE vaccines. The deltoid site also allows for easier self-care post-injection, as patients can apply cold compresses or move the arm to alleviate discomfort. In contrast, buttock injections carry a higher risk of sciatic nerve injury, making them less suitable for routine immunizations like JE vaccines. The deltoid’s prominence in vaccine administration underscores its reliability and safety profile.
Practical tips for patients receiving the JE vaccine in the deltoid muscle include wearing loose-fitting clothing to easily expose the upper arm and avoiding strenuous arm activity for 24 hours post-injection. Over-the-counter pain relievers, such as acetaminophen, can be taken if soreness persists, though aspirin should be avoided in children due to the risk of Reye’s syndrome. Keeping the arm active with gentle movements can help reduce stiffness, but heavy lifting or intense exercise should be postponed. For travelers receiving the vaccine, scheduling the injection at least 1–2 weeks before departure allows time for immunity to develop. Understanding these specifics ensures a smoother vaccination experience and optimal protection against Japanese encephalitis.
DTaP Vaccine: One Shot for Diphtheria, Tetanus, and Pertussis Protection?
You may want to see also
Explore related products

$13.98 $15.99

$13.98 $15.99

$8.48 $10.48



![]()
Vaccine Administration: Given intramuscularly, not subcutaneously, for optimal immune response
The Japanese encephalitis (JE) vaccine is administered intramuscularly, typically into the deltoid muscle of the upper arm for adults and older children, or the vastus lateralis muscle of the thigh for infants and younger children. This route of administration is critical for ensuring the vaccine reaches the muscle tissue, where it can elicit a robust immune response. Injecting the vaccine subcutaneously, or into the layer of fat beneath the skin, may result in reduced immunogenicity, as the vaccine’s antigens are not delivered to the optimal site for immune cell activation.
Intramuscular injection requires precision to avoid subcutaneous administration, which can occur if the needle is not inserted deeply enough. For the deltoid muscle, the injection site is the middle to upper outer aspect of the arm, approximately 2–3 finger widths below the acromion process. The needle should be inserted at a 90-degree angle, with a length appropriate for the patient’s age and size (typically 1 inch for adults and 5/8 inch for children). For the vastus lateralis, the injection site is the mid-thigh, roughly 2–3 finger widths above the superior lateral border of the patella, with the needle inserted at a 90-degree angle using a 5/8 inch needle for infants and young children.
The dosage and schedule of the JE vaccine vary by age and vaccine type. For example, the inactivated Vero cell culture-derived vaccine (IXIARO) is given in a 2-dose series, 28 days apart, with each dose being 0.5 mL for individuals aged 2 months and older. In contrast, the live-attenuated vaccine (SA14-14-2) is administered in a single 0.5 mL dose for adults and children over 1 year, or a 0.25 mL dose for infants aged 8 months to 1 year. Adhering to the correct dosage and administration technique is essential to maximize protection against Japanese encephalitis, a potentially severe mosquito-borne disease.
Practical tips for healthcare providers include ensuring the vaccine is at room temperature before administration to minimize discomfort and using proper needle size to avoid tissue damage. Patients should be informed to keep the injection site clean and monitor for mild side effects, such as soreness or redness, which typically resolve within a few days. In rare cases, more severe reactions may occur, warranting immediate medical attention. By following these guidelines, healthcare professionals can optimize the immune response to the JE vaccine and enhance its protective efficacy.
Comparatively, the intramuscular route for JE vaccination mirrors the administration of other vaccines, such as influenza or hepatitis A, but differs from subcutaneous vaccines like measles or mumps. This distinction underscores the importance of training healthcare providers to recognize and correctly administer vaccines based on their specific requirements. For travelers or individuals in endemic regions, ensuring proper JE vaccine administration is a critical step in disease prevention, particularly in areas where mosquito control measures are insufficient. Ultimately, the intramuscular delivery of the JE vaccine is a precise and purposeful method designed to harness the body’s immune system effectively.
Are Vaccine Antitoxins and Antitoxins the Same Thing?
You may want to see also
Explore related products






![]()
Age-Specific Sites: Children may receive it in the thigh muscle instead of the arm
The Japanese encephalitis (JE) vaccine is typically administered intramuscularly, but the injection site varies depending on the recipient’s age. For children, especially infants and toddlers, the thigh muscle (vastus lateralis) is often the preferred location. This choice is rooted in both anatomical and practical considerations. The thigh muscle in young children is more developed and accessible compared to the deltoid muscle in the arm, which is commonly used for adults. This ensures the vaccine is delivered effectively and minimizes discomfort.
From a procedural standpoint, administering the JE vaccine in the thigh follows specific guidelines. For infants and children under 3 years old, the injection is given in the anterolateral aspect of the thigh, approximately 2–3 cm above the knee. The needle length is adjusted based on age: a 5/8-inch needle is suitable for most children in this age group. Healthcare providers are instructed to stretch the skin slightly before inserting the needle at a 90-degree angle to ensure proper intramuscular delivery. This technique reduces the risk of hitting bone or causing unnecessary pain.
The rationale behind using the thigh for younger recipients is twofold. First, the deltoid muscle in infants and toddlers is underdeveloped, making it less ideal for intramuscular injections. Second, the thigh provides a larger, more stable area for injection, which is particularly important when administering vaccines to squirmy or uncooperative children. Parents and caregivers should be reassured that this site is safe and effective, with studies showing comparable immunogenicity to other injection sites.
Practical tips for parents include dressing children in loose-fitting clothing to easily access the thigh area during vaccination. After the injection, gentle massage or a cold compress can help alleviate any soreness. It’s also important to monitor the child for common side effects, such as mild fever or localized swelling, though these are typically transient. For children aged 3 and above, the healthcare provider may transition to the deltoid muscle, depending on the child’s size and muscle development.
In summary, the thigh muscle is the recommended injection site for the JE vaccine in young children, offering a safe and effective alternative to the arm. Adhering to age-specific guidelines ensures optimal vaccine delivery while minimizing discomfort. Parents and healthcare providers alike can benefit from understanding these nuances, ensuring a smoother vaccination experience for the child.
Bioinformatics Revolutionizes Vaccine Discovery: Accelerating Research and Development
You may want to see also
Explore related products




![]()
Pain Management: Applying ice or numbing cream can reduce injection site discomfort
The Japanese encephalitis vaccine is typically administered into the deltoid muscle of the upper arm for adults and older children, while infants and younger children may receive it in the vastus lateralis muscle of the thigh. Regardless of the injection site, discomfort is a common concern. Pain management strategies can significantly improve the vaccination experience, particularly for those who are needle-averse or have sensitive skin. Applying ice or numbing cream before the injection is a simple yet effective method to minimize pain and anxiety.
From an analytical perspective, the efficacy of ice and numbing cream lies in their ability to reduce nerve sensitivity at the injection site. Ice acts as a vasoconstrictor, narrowing blood vessels and decreasing blood flow to the area, which numbs the skin and reduces the perception of pain. Numbing creams, such as those containing lidocaine or prilocaine, work by blocking nerve signals, providing localized anesthesia. Studies show that these methods can reduce injection pain by up to 50%, making them valuable tools in pain management. For optimal results, apply ice for 10–15 minutes before the injection or use a numbing cream 30–60 minutes prior, following the product’s dosage instructions, typically 2–5 grams for adults.
Instructively, incorporating these techniques into the vaccination process is straightforward. For ice application, wrap a small ice pack or frozen gel pack in a thin cloth to prevent frostbite and hold it firmly against the deltoid or thigh muscle. Ensure the area is clean and dry before application. For numbing creams, clean the injection site with alcohol and allow it to dry, then apply a thin layer of the cream and cover it with an occlusive dressing to enhance absorption. Always follow the manufacturer’s guidelines, especially for children, as dosage and application times may vary. For instance, children under 12 may require half the adult dose of numbing cream.
Persuasively, the benefits of using ice or numbing cream extend beyond immediate pain relief. Reducing discomfort can make individuals, especially children or those with needle phobia, more willing to receive necessary vaccinations. This compliance is crucial for public health, particularly for vaccines like Japanese encephalitis, which protects against a potentially fatal disease. By making the experience less daunting, these methods contribute to higher vaccination rates and better community immunity. Additionally, they empower individuals to take an active role in their healthcare, fostering a positive attitude toward preventive measures.
Comparatively, while ice and numbing cream are effective, they are not the only pain management options. Distraction techniques, deep breathing, and topical heat are alternatives, but ice and numbing cream stand out for their simplicity and accessibility. Ice is readily available and cost-effective, while numbing creams are widely available over the counter. Unlike oral pain relievers, which may not target the injection site directly, these methods provide localized relief without systemic side effects. However, it’s essential to note that numbing creams should not be used on broken skin or by individuals with allergies to their components.
Descriptively, the experience of using ice or numbing cream can transform the vaccination process. Imagine arriving for your Japanese encephalitis vaccine, armed with a small ice pack or a tube of numbing cream. As you sit in the waiting area, you apply the ice or cream, feeling the coolness or tingling sensation spread across your skin. By the time the nurse prepares the injection, the area is numb, and the needle prick is barely noticeable. The procedure is quick, and you leave with minimal discomfort, grateful for the simple yet effective solution. This small step can make a significant difference, turning a potentially stressful event into a manageable one.
Understanding Vaccine Excipients: A Common Example Explained Simply
You may want to see also
![]()
Post-Injection Care: Avoid heavy arm use for 24 hours to minimize soreness
The Japanese encephalitis vaccine is typically administered into the deltoid muscle of the upper arm, a site chosen for its accessibility and robust muscle tissue, which aids in efficient vaccine absorption. After receiving this injection, the arm may experience soreness, swelling, or redness, common reactions to the body’s immune response. To mitigate these discomforts, healthcare providers often recommend minimizing strenuous arm activity for the first 24 hours post-vaccination. This precaution allows the muscle to recover without additional strain, reducing the likelihood of prolonged soreness.
From a practical standpoint, avoiding heavy arm use doesn’t mean immobilizing the limb entirely. Light activities like typing, writing, or lifting lightweight objects are generally safe. However, tasks requiring significant force—such as carrying groceries, intense exercise, or repetitive lifting—should be postponed. For children or adults with physically demanding jobs, planning the vaccination timing to allow for a day of reduced arm use can be beneficial. For instance, scheduling the vaccine on a Friday evening could provide the weekend for recovery.
The science behind this recommendation lies in the vaccine’s interaction with muscle tissue. When injected into the deltoid, the vaccine triggers an immune response, leading to temporary inflammation. Heavy arm use during this period can exacerbate inflammation, prolonging discomfort. Studies show that mild soreness typically resolves within 2–3 days, but excessive activity can extend this duration. For individuals receiving the vaccine in a two-dose series (common for brands like IXIARO or IMOJEV), adhering to this advice after each dose ensures optimal comfort and compliance.
Persuasively, consider this: ignoring post-injection care guidelines may not only increase personal discomfort but also deter others from vaccination. Sharing experiences of manageable side effects, thanks to proper care, can encourage vaccine uptake in communities where Japanese encephalitis is endemic. Simple measures like using the non-vaccinated arm for heavy tasks or applying a cold compress (not directly on the injection site) can further alleviate symptoms. By prioritizing this 24-hour window of care, individuals can ensure a smoother vaccination experience, focusing on protection rather than pain.
RSV Vaccine: Annual Booster or One-Time Protection?
You may want to see also
Frequently asked questions
The Japanese encephalitis vaccine is typically injected into the deltoid muscle of the upper arm for adults and older children, or the anterolateral aspect of the thigh for infants and young children.
No, the Japanese encephalitis vaccine is not recommended to be injected into the buttocks. It should be administered into the deltoid muscle or thigh, depending on the age of the recipient.
The Japanese encephalitis vaccine is administered intramuscularly, meaning it is injected directly into the muscle tissue.
Yes, the injection site varies by age. For adults and older children, it is given in the deltoid muscle of the upper arm, while for infants and young children, it is administered in the anterolateral thigh muscle.
After receiving the injection, it is advisable to avoid strenuous activity with the injected arm or leg for a short period. Applying a cold compress can help reduce any localized pain or swelling at the injection site.