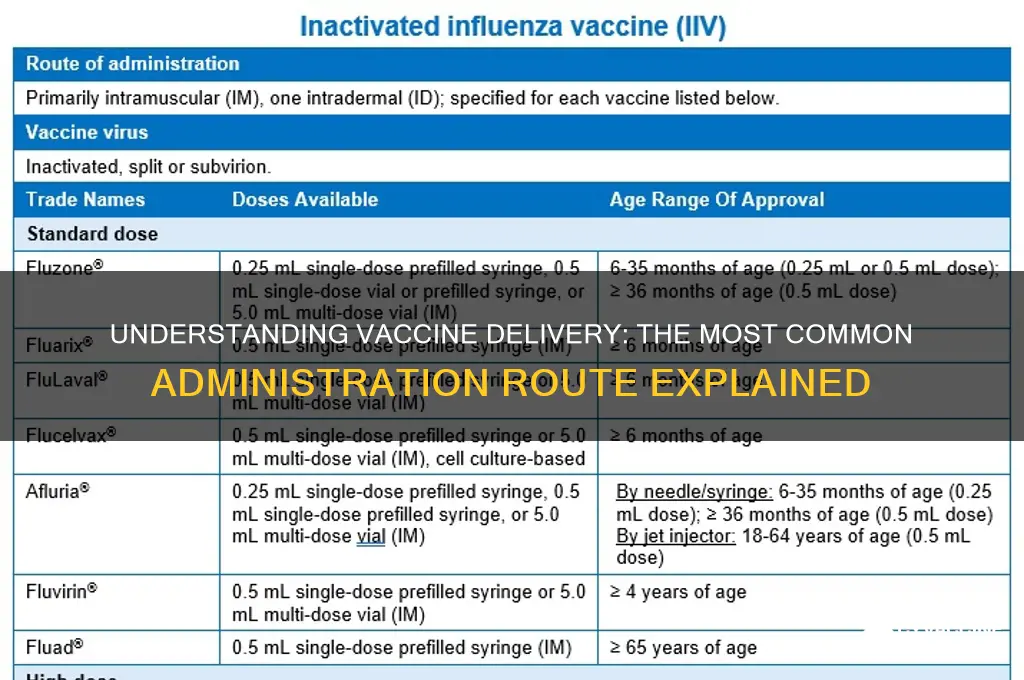
Vaccines are typically administered through various routes, but the most common and widely used method is the intramuscular (IM) injection, which involves delivering the vaccine directly into the muscle tissue, usually in the deltoid muscle of the upper arm for adults or the vastus lateralis muscle in the thigh for infants and young children. This route is preferred for many vaccines, including those for influenza, measles, mumps, rubella, and COVID-19, as it allows for efficient absorption and a robust immune response. Other routes, such as subcutaneous (under the skin) and oral administration, are also utilized depending on the specific vaccine and its formulation, but intramuscular injection remains the standard due to its effectiveness and ease of administration.
| Characteristics | Values |
|---|---|
| Most Common Route | Intramuscular (IM) injection |
| Primary Vaccines Administered IM | Influenza, COVID-19, Hepatitis A/B, MMR (Measles, Mumps, Rubella) |
| Injection Site | Deltoid muscle (arm) for adults, vastus lateralis (thigh) for infants |
| Needle Length | 1-1.5 inches (25-38 mm) for adults, shorter for children |
| Advantages | Efficient antigen delivery to muscle tissue, robust immune response |
| Disadvantages | Pain, local reactions (redness, swelling), requires trained personnel |
| Alternative Routes | Subcutaneous, Oral, Intranasal (less common for most vaccines) |
| Global Usage | Predominantly used in routine immunization programs worldwide |
| Recent Trends | Increasing use of IM for novel vaccines (e.g., mRNA vaccines) |
| WHO Recommendation | Preferred route for most inactivated and live attenuated vaccines |
Explore related products






What You'll Learn
- Intramuscular Injection: Most vaccines are administered via intramuscular injection for optimal immune response
- Subcutaneous Injection: Some vaccines, like MMR, are given just under the skin
- Oral Vaccines: Vaccines like polio can be administered orally for ease and safety
- Intranasal Vaccines: Flu vaccines are sometimes delivered intranasally to target respiratory immunity
- Transdermal Patches: Emerging methods use patches for needle-free vaccine delivery
![]()
Intramuscular Injection: Most vaccines are administered via intramuscular injection for optimal immune response
Intramuscular injection stands as the cornerstone of vaccine administration, favored for its ability to elicit robust immune responses. This method delivers the vaccine directly into the muscle tissue, typically in the deltoid muscle of the upper arm for adults or the vastus lateralis muscle of the thigh for infants and young children. The muscle’s rich blood supply ensures rapid absorption of the vaccine antigens, triggering a systemic immune reaction. For instance, the influenza vaccine, administered intramuscularly, achieves protective antibody levels in 90-100% of healthy adults within 2-4 weeks. This efficiency underscores why intramuscular injection remains the gold standard for vaccines like MMR, hepatitis B, and COVID-19.
The technique itself is precise and requires adherence to specific guidelines. Healthcare providers must use a needle length appropriate for the patient’s age and body mass—typically 1-1.5 inches for adults and 5/8 inch for infants. The injection site should be cleaned with an alcohol swab, and the needle inserted at a 90-degree angle to ensure the vaccine reaches the muscle tissue. Aspiration, or pulling back on the plunger to check for blood, is generally unnecessary for vaccine administration. Proper positioning of the patient—seated or lying down—minimizes discomfort and ensures accurate delivery. These steps, when followed meticulously, maximize the vaccine’s efficacy while minimizing adverse reactions.
Comparatively, intramuscular injection outshines other routes like subcutaneous or oral administration in terms of immune response potency. Subcutaneous injections, while effective for certain vaccines like measles, deliver antigens into the fatty layer beneath the skin, resulting in a slower and often less vigorous immune response. Oral vaccines, such as the polio vaccine, face challenges like degradation in the gastrointestinal tract and variable absorption rates. Intramuscular injection bypasses these limitations, making it ideal for vaccines requiring rapid and systemic immunity. This superiority is particularly critical for vaccines targeting highly contagious diseases or those requiring booster doses.
Practical considerations further cement the dominance of intramuscular injection in vaccine administration. The method is cost-effective, requiring minimal equipment and training compared to more complex delivery systems. It is also versatile, accommodating a wide range of vaccine formulations, from inactivated viruses to mRNA-based vaccines. For example, the COVID-19 mRNA vaccines, administered intramuscularly, have demonstrated efficacy rates exceeding 90% in preventing severe disease. However, patients should be advised to avoid massaging the injection site, as this can lead to localized pain or swelling. Applying a cold compress post-injection can alleviate discomfort, though this is rarely necessary.
In conclusion, intramuscular injection’s unparalleled ability to stimulate a strong and rapid immune response makes it the most common and effective route for vaccine administration. Its precision, efficiency, and adaptability across diverse vaccine types and patient populations solidify its role in global immunization efforts. Whether for routine childhood vaccinations or emergency pandemic responses, this method remains a reliable tool in the fight against infectious diseases. By understanding its mechanics and adhering to best practices, healthcare providers can ensure optimal outcomes for every vaccine dose delivered.
Pharmacists Vaccinating: Legal in Florida?
You may want to see also
Explore related products






![]()
Subcutaneous Injection: Some vaccines, like MMR, are given just under the skin
Subcutaneous injection, a method where vaccines are administered just beneath the skin, is a precise and effective route for delivering certain immunizations. Unlike intramuscular injections that target muscle tissue, this approach deposits the vaccine into the fatty layer between the skin and muscle, allowing for a slower release and absorption by the immune system. The measles, mumps, and rubella (MMR) vaccine is a prime example of a vaccine typically given via this method. This technique is particularly useful for vaccines that require a robust immune response from the body’s lymphatic system, as the subcutaneous tissue is rich in immune cells.
Administering a subcutaneous injection involves specific steps to ensure safety and efficacy. The recommended site for adults and children over 1 year is the fatty tissue over the deltoid muscle in the upper arm, while infants under 1 year are often injected in the fatty tissue of the anterolateral thigh. The needle should be inserted at a 45-degree angle, and the typical dosage for the MMR vaccine is 0.5 mL for both children and adults. It’s crucial to avoid injecting into muscle or blood vessels, as this can reduce the vaccine’s effectiveness or cause adverse reactions. Healthcare providers often use a short, fine-gauge needle (25–27 gauge) to minimize discomfort.
One of the advantages of subcutaneous injection is its ability to elicit a strong immune response with a smaller dose compared to other routes. For instance, the MMR vaccine, when given subcutaneously, provides long-lasting immunity against three highly contagious diseases with just two doses—the first at 12–15 months and the second at 4–6 years. This method also reduces the risk of systemic side effects, as the vaccine is absorbed more gradually. However, it’s important to note that the injection site may experience mild reactions, such as redness, swelling, or tenderness, which typically resolve within a few days.
Practical tips for patients and caregivers can enhance the experience of receiving a subcutaneous vaccine. Applying a cool compress to the injection site before and after can help reduce pain and swelling. Distraction techniques, such as deep breathing or engaging in conversation, can also ease anxiety, particularly in children. After the injection, avoiding strenuous activity with the vaccinated arm for 24 hours can prevent discomfort. If persistent pain or unusual symptoms occur, consulting a healthcare provider is essential to rule out complications.
In comparison to other routes like oral or intramuscular administration, subcutaneous injection strikes a balance between efficacy and patient comfort. While oral vaccines offer convenience, they can be less effective due to digestive breakdown. Intramuscular injections, though common, may cause more pain and require larger doses. Subcutaneous delivery, particularly for vaccines like MMR, leverages the body’s natural immune pathways efficiently, making it a preferred choice for specific immunizations. Understanding this method empowers individuals to approach vaccinations with confidence and clarity.
Pilot Vaccination Requirements: What You Need to Know
You may want to see also
Explore related products






![]()
Oral Vaccines: Vaccines like polio can be administered orally for ease and safety
The most common route of vaccine administration is intramuscular injection, but oral vaccines offer a compelling alternative, particularly for diseases like polio. This method eliminates the need for needles, making it ideal for mass immunization campaigns, especially in resource-limited settings. Oral polio vaccine (OPV), for instance, is administered as drops, typically 0.5 mL for infants and children, and can be given without specialized medical training. This simplicity has been pivotal in the global effort to eradicate polio, demonstrating the power of oral vaccines in reaching vulnerable populations.
One of the key advantages of oral vaccines is their ability to stimulate mucosal immunity, the body’s first line of defense against pathogens that enter through the mouth or nose. OPV, for example, replicates in the gut, producing antibodies that prevent the poliovirus from establishing infection. This localized immune response is particularly effective for diseases that primarily infect mucosal surfaces, such as rotavirus, another condition for which oral vaccines are available. Administering these vaccines to infants between 6 and 32 weeks of age ensures protection during the period of highest vulnerability.
However, oral vaccines are not without challenges. Their efficacy can be influenced by factors like gastric acidity, malnutrition, or concurrent gastrointestinal infections, which may reduce the vaccine’s ability to replicate effectively. For instance, studies have shown that OPV efficacy is lower in regions with high rates of malnutrition or diarrheal diseases. To mitigate this, it’s crucial to administer oral vaccines on an empty stomach or with minimal food intake, as recommended by the World Health Organization (WHO). Additionally, maintaining a cold chain for storage is essential, though oral vaccines generally have more flexible temperature requirements compared to injectable vaccines.
Despite these considerations, the benefits of oral vaccines in terms of ease of administration and safety are undeniable. They eliminate the risk of needle-related injuries and reduce the need for trained healthcare personnel, making them a practical choice for large-scale immunization programs. For parents, oral vaccines offer a less intimidating experience for children, who may fear injections. Practical tips include ensuring the vaccine is administered directly into the mouth and confirming the child swallows it, as spitting can reduce efficacy. As research advances, oral vaccines may become even more versatile, potentially addressing diseases beyond polio and rotavirus.
In conclusion, while intramuscular injections dominate vaccine administration, oral vaccines like OPV provide a unique and valuable alternative. Their ability to confer mucosal immunity, coupled with their ease of use, makes them indispensable tools in public health. By addressing challenges like efficacy in high-risk populations and adhering to best practices, oral vaccines can continue to play a critical role in preventing disease and saving lives globally.
Global Vaccination Rates: A Comprehensive Overview of Worldwide Immunization Trends
You may want to see also
Explore related products

$5 $32.99





![]()
Intranasal Vaccines: Flu vaccines are sometimes delivered intranasally to target respiratory immunity
Intranasal vaccines represent a targeted approach to immunization, particularly for respiratory infections like the flu. Unlike traditional injections that stimulate systemic immunity, intranasal delivery directly engages the mucosal immune system in the respiratory tract—the primary site of influenza virus entry. This method mimics the natural infection pathway, triggering the production of secretory IgA antibodies and resident memory T cells, which provide localized protection against viral invasion. For instance, FluMist Quadrivalent, a live attenuated influenza vaccine (LAIV), is administered as a 0.2 mL dose (0.1 mL per nostril) for individuals aged 2 to 49 years. This route is especially advantageous for children and needle-averse individuals, offering a painless alternative to intramuscular shots.
The efficacy of intranasal vaccines hinges on their ability to activate both systemic and mucosal immunity. While injected vaccines excel at generating circulating antibodies, intranasal formulations excel at preventing viral shedding and transmission by fortifying the respiratory mucosa. Studies show that LAIV can reduce flu symptoms in children by up to 50%, though its effectiveness varies by age and viral strain. However, this route is not without limitations: LAIV is contraindicated for pregnant individuals, immunocompromised patients, and those with severe asthma due to its live virus components. Proper administration is critical—the vaccine must be stored between 2°C and 8°C, and the spray should be delivered while the recipient is in an upright position to ensure even distribution in the nasal passages.
From a practical standpoint, intranasal vaccines streamline vaccination campaigns by eliminating the need for needles and reducing healthcare worker burden. Their ease of administration makes them ideal for mass immunization efforts, particularly in pediatric populations. However, their success depends on patient compliance; recipients must refrain from nose-blowing or sneezing immediately after vaccination to allow the vaccine to adhere to nasal tissues. Additionally, intranasal vaccines often require larger antigen doses compared to injections, as the nasal mucosa can degrade or expel foreign substances. Manufacturers address this challenge through formulations like chitosan-based nanoparticles, which enhance antigen stability and uptake.
Comparatively, intranasal vaccines occupy a niche in the broader vaccine landscape, complementing rather than replacing traditional routes. While intramuscular injections remain the gold standard for systemic immunity, intranasal delivery offers a specialized solution for respiratory pathogens. Ongoing research explores its potential for COVID-19 and other respiratory viruses, with candidates like the AstraZeneca intranasal vaccine showing promise in clinical trials. As the field advances, intranasal vaccines may become a cornerstone of mucosal immunology, bridging the gap between systemic protection and localized defense. For now, they serve as a testament to the versatility of vaccine administration routes, tailored to meet the unique challenges of respiratory infections.
Vaccine Shots: Building Immunity or Just a Myth?
You may want to see also
Explore related products






![]()
Transdermal Patches: Emerging methods use patches for needle-free vaccine delivery
The most common route of administration for vaccines is intramuscular injection, typically delivered via a needle into the deltoid muscle of the upper arm for adults or the vastus lateralis muscle of the thigh for infants and young children. This method ensures robust immune responses by directly introducing antigens into muscle tissue, where they can be efficiently processed by the immune system. However, needle-based delivery poses challenges, including pain, anxiety, and the need for trained healthcare personnel, particularly in resource-limited settings. These limitations have spurred innovation in alternative delivery methods, among which transdermal patches are emerging as a promising needle-free solution.
Transdermal patches leverage the skin’s permeability to deliver vaccines without piercing it, using microneedles or chemical enhancers to bypass the stratum corneum, the skin’s outermost barrier. Microneedle patches, for instance, consist of microscopic needles that dissolve upon application, releasing vaccine antigens into the epidermis or dermis, where antigen-presenting cells reside. A notable example is the influenza vaccine patch developed by researchers at the Georgia Institute of Technology, which demonstrated comparable immunogenicity to traditional injections in preclinical trials. This method not only eliminates needle-related pain but also simplifies storage and transportation, as patches can be stored at room temperature, unlike many liquid vaccines that require refrigeration.
One of the key advantages of transdermal patches is their potential for self-administration, empowering individuals to vaccinate themselves at home. This could significantly improve vaccination rates, particularly in remote or underserved areas where access to healthcare facilities is limited. For example, a study published in *Nature Biotechnology* highlighted that microneedle patches for COVID-19 vaccines could achieve similar immune responses to intramuscular injections while being more easily distributed and administered. However, challenges remain, such as ensuring consistent dosing and addressing variability in skin thickness and hydration across different age groups and populations.
Practical considerations for transdermal patch use include application time, typically ranging from 5 to 30 minutes, depending on the patch design and vaccine formulation. Users must apply firm, even pressure to ensure all microneedles penetrate the skin, and patches should be stored in a cool, dry place until use. While transdermal patches are generally safe, individuals with skin conditions such as eczema or psoriasis should consult a healthcare provider before use, as irritation may occur. As research advances, transdermal patches could revolutionize vaccine delivery, offering a painless, convenient, and scalable alternative to traditional injections.
RNA Vaccines: A Breakthrough in Medicine with Proven Success Stories
You may want to see also
Frequently asked questions
The most common route of administration for vaccines is intramuscular injection, where the vaccine is delivered into the muscle tissue, typically in the upper arm or thigh.
Yes, other routes include subcutaneous injection (into the layer of fat beneath the skin), oral (taken by mouth), intranasal (sprayed into the nose), and intradermal (into the skin’s top layer).
Intramuscular injection is preferred because it allows for rapid absorption of the vaccine, strong immune response, and ease of administration, making it effective for many types of vaccines.
Examples include the oral polio vaccine (oral), influenza nasal spray (intranasal), and tuberculosis vaccine (BCG) (intradermal).
Yes, the route of administration can significantly impact the vaccine’s effectiveness by influencing how the immune system responds. For example, intramuscular injections often elicit stronger systemic immunity, while intranasal vaccines may enhance mucosal immunity.