Vaccination rates vary significantly around the world, influenced by factors such as healthcare infrastructure, government policies, public awareness, and socioeconomic conditions. While some high-income countries like the United States, Canada, and those in Western Europe boast high vaccination coverage for diseases like measles, COVID-19, and influenza, many low- and middle-income nations in Africa, Asia, and parts of Latin America face challenges in achieving widespread immunization. Global initiatives like Gavi, the Vaccine Alliance, and COVAX have aimed to bridge this gap, but disparities persist, particularly in regions with limited access to vaccines, political instability, or vaccine hesitancy. Understanding these variations is crucial for addressing global health inequities and preventing the spread of preventable diseases.
Explore related products






What You'll Learn
![]()
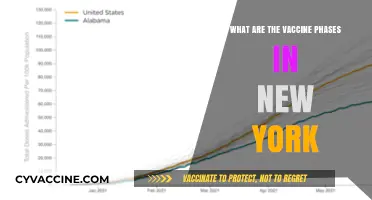
Global Vaccination Trends
Global vaccination rates reveal a stark divide, with high-income countries administering over 150 doses per 100 people compared to just 20 doses in low-income nations. This disparity underscores the inequity in vaccine access, exacerbated by factors like supply chain limitations, political instability, and vaccine hesitancy. For instance, while countries like Canada and the UAE have fully vaccinated over 80% of their populations, many African nations struggle to reach 20%. This gap not only prolongs the pandemic but also highlights the need for global cooperation in vaccine distribution.
Analyzing trends, COVID-19 vaccination campaigns have accelerated the adoption of mRNA technology, which now accounts for over 60% of doses administered globally. However, this innovation has yet to translate into equitable access. Wealthier nations have secured booster doses for their populations, while many low-income countries are still administering first doses. For example, the U.S. has administered over 100 million booster shots, whereas countries like Haiti have vaccinated less than 1% of their population. This imbalance demands a reevaluation of global vaccine allocation strategies.
Persuasively, the success of vaccination programs hinges on addressing hesitancy, which varies widely by region. In Europe, skepticism about vaccine safety has slowed uptake in countries like France and Germany, where only 75% of the population is fully vaccinated. Conversely, in Southeast Asia, cultural and religious beliefs have influenced acceptance rates in countries like Indonesia, where vaccination campaigns have been more successful due to targeted community engagement. Governments must invest in localized communication strategies to build trust and dispel misinformation.
Comparatively, childhood vaccination rates offer a contrasting picture, with global coverage for vaccines like measles and polio remaining relatively stable at around 85%. However, disruptions caused by the COVID-19 pandemic have led to backsliding in some regions, particularly in sub-Saharan Africa and South Asia. For instance, 23 million children missed out on basic vaccines in 2020, the highest number in over a decade. This regression underscores the importance of maintaining robust immunization systems even during health crises.
Practically, improving global vaccination rates requires a multi-faceted approach. High-income countries should fulfill their dose-sharing pledges, with initiatives like COVAX aiming to deliver 2 billion doses to low-income nations by 2022. Additionally, low-cost, easy-to-store vaccines like those developed by Novavax and Johnson & Johnson are critical for reaching remote areas. Finally, governments must prioritize health infrastructure, ensuring cold chain capabilities and trained personnel. By combining equitable distribution, innovation, and local engagement, the world can bridge the vaccination gap and protect global health.
Understanding Vaccine Lot Numbers: How Many Share the Same Identifier?
You may want to see also
Explore related products


![International Certificate of Vaccination with Vinyl Document Holder - World Health Organization Bilingual Version [cards] World Health Organization [Jan 01, 2007]](https://m.media-amazon.com/images/I/61SHjBP1VYL._AC_UY218_.jpg)



![]()
Regional Vaccination Disparities
Global vaccination rates reveal a stark divide, with high-income countries often achieving coverage above 80% for essential vaccines like measles and COVID-19, while low-income regions struggle to reach 50%. This disparity isn’t just a number—it translates to millions of preventable deaths annually, particularly among children under five. For instance, in sub-Saharan Africa, only 54% of children receive the full course of the diphtheria-tetanus-pertussis (DTP3) vaccine, compared to 94% in North America. Such gaps highlight systemic inequalities in healthcare infrastructure, funding, and access.
Consider the COVID-19 vaccine rollout, a recent case study in regional disparities. By late 2021, over 70% of the population in high-income countries had received at least one dose, while many African nations had vaccinated less than 10% of their populations. Wealthy nations hoarded doses, leaving COVAX, the global vaccine-sharing initiative, underfunded and overwhelmed. This imbalance wasn’t just unethical—it prolonged the pandemic, allowing variants like Delta and Omicron to emerge in unvaccinated regions and spread globally.
To address these disparities, a multi-pronged approach is essential. First, increase funding for global vaccine initiatives like Gavi, the Vaccine Alliance, which has immunized over 980 million children since 2000. Second, strengthen local healthcare systems in low-income regions by investing in cold chain infrastructure, training healthcare workers, and improving supply chain logistics. For example, solar-powered refrigerators can ensure vaccines remain viable in remote areas without reliable electricity. Third, high-income countries must commit to equitable vaccine distribution, sharing surplus doses and waiving intellectual property rights to enable local production.
Practical steps for individuals and organizations include advocating for policy changes, supporting NGOs focused on global health, and promoting vaccine literacy to combat misinformation. For instance, in South Asia, where vaccine hesitancy is fueled by rumors, community health workers have successfully used door-to-door education campaigns to increase uptake. Similarly, in Latin America, partnerships between governments and tech companies have utilized mobile apps to track vaccination schedules and remind parents of appointments.
Ultimately, regional vaccination disparities are not an insurmountable challenge but a call to action. By combining global cooperation, local innovation, and sustained investment, we can bridge the gap and ensure that every child, regardless of where they are born, has access to life-saving vaccines. The cost of inaction is measured in lives lost—the cost of action is a fraction of global healthcare spending. The choice is clear.
Pregnant and Vaccinated: Should You Still Wear a Mask?
You may want to see also
Explore related products





![]()
COVID-19 Vaccination Rates
As of recent data, COVID-19 vaccination rates vary dramatically across the globe, reflecting disparities in access, infrastructure, and public trust. High-income countries like Canada and Portugal have achieved over 80% full vaccination rates among their eligible populations, primarily due to robust healthcare systems and early procurement of doses. In contrast, many low-income nations in Africa, such as the Democratic Republic of Congo and South Sudan, report rates below 20%, hindered by supply chain challenges and vaccine hesitancy. This gap underscores the inequities in global health responses and the need for targeted interventions to bridge the divide.
Analyzing the factors behind these disparities reveals a complex interplay of logistics and societal attitudes. Wealthier nations often secured doses through advance purchase agreements, leaving poorer countries dependent on initiatives like COVAX, which faced delays and shortages. Additionally, misinformation campaigns and historical mistrust of medical systems have suppressed uptake in some regions. For instance, in parts of Eastern Europe, vaccination rates lag despite dose availability, influenced by widespread skepticism. Addressing these issues requires not just distributing vaccines but also building trust through community engagement and transparent communication.
From a practical standpoint, increasing COVID-19 vaccination rates demands tailored strategies. In urban areas, mobile clinics and workplace vaccination drives have proven effective, while rural regions benefit from integrating vaccine delivery with existing health services. For children aged 5–11, who often receive lower doses (typically 10 micrograms per shot compared to 30 micrograms for adults), schools can serve as vaccination hubs. Incentives, such as small rewards or public recognition, have also boosted participation in some communities. Policymakers must prioritize data-driven approaches, adapting methods to local contexts for maximum impact.
A comparative look at successful campaigns highlights the importance of leadership and innovation. Countries like Singapore and the United Arab Emirates achieved high vaccination rates through mandatory policies for certain activities and streamlined registration processes. Meanwhile, New Zealand’s emphasis on collective responsibility resonated culturally, driving voluntary participation. These examples illustrate that one-size-fits-all solutions are insufficient; instead, strategies must align with cultural values and societal norms. For instance, leveraging religious leaders or local influencers can counter hesitancy more effectively than generic messaging.
Ultimately, the global effort to raise COVID-19 vaccination rates is a test of equity and collaboration. While high-income nations focus on boosters and pediatric doses, low-income countries still struggle with first-dose coverage. International cooperation, including dose sharing and technology transfer, remains critical. Individuals can contribute by staying informed, advocating for equitable distribution, and supporting local vaccination drives. The pandemic has shown that no one is safe until everyone is safe—a principle that must guide ongoing efforts to protect global health.
DTap's Tetanus Vaccine: Understanding Its Unique Composition
You may want to see also
Explore related products






![]()
Childhood Immunization Coverage
Global childhood immunization coverage stands at a critical juncture, with approximately 83% of infants receiving the third dose of the diphtheria-tetanus-pertussis (DTP3) vaccine in 2022. This figure, reported by the World Health Organization (WHO), masks significant disparities. High-income countries often achieve over 95% coverage, while low-income nations struggle to reach 50% in some regions. The DTP3 vaccine serves as a benchmark for immunization systems, indicating access to essential vaccines like measles, polio, and hepatitis B. Despite progress, an estimated 25 million children worldwide missed out on basic vaccines in 2021, leaving them vulnerable to preventable diseases.
Analyzing these numbers reveals systemic challenges. In sub-Saharan Africa and parts of Southeast Asia, logistical hurdles, such as inadequate cold chain infrastructure and limited healthcare access, hinder vaccine delivery. For instance, the measles vaccine, requiring two doses by age 2, sees only 71% global coverage for the second dose, leaving millions susceptible to outbreaks. Conflict zones exacerbate the issue; in countries like Yemen and Syria, immunization rates plummet due to disrupted health services. Conversely, countries with robust health systems, like Rwanda and Cuba, demonstrate how political commitment and community engagement can achieve near-universal coverage.
To improve childhood immunization, a multi-pronged approach is essential. First, strengthen health systems by investing in trained personnel, reliable supply chains, and data monitoring. Second, address vaccine hesitancy through culturally sensitive education campaigns. For example, in India, the introduction of the rotavirus vaccine was accompanied by community workshops, increasing uptake by 40%. Third, leverage technology; mobile clinics and digital immunization records have proven effective in remote areas of Brazil and Kenya. Parents should ensure their children receive vaccines on schedule: BCG and hepatitis B at birth, DTP and polio at 6, 10, and 14 weeks, and measles at 9 and 15 months.
Comparatively, regions with high coverage offer lessons. Scandinavian countries achieve over 98% DTP3 coverage through mandatory school entry requirements and public trust in health authorities. In contrast, the United States, despite its resources, faces pockets of under-vaccination due to misinformation and policy gaps. A persuasive argument emerges: universal childhood immunization is not just a health issue but a socioeconomic imperative. Every $1 invested in vaccines yields $44 in economic benefits by preventing illness and reducing healthcare costs.
Practically, caregivers can take proactive steps. Keep a vaccination calendar, inquire about catch-up schedules for missed doses, and advocate for school-based immunization programs. Governments must prioritize equity, ensuring marginalized communities are not left behind. For instance, Nigeria’s partnership with Gavi, the Vaccine Alliance, has increased coverage by deploying solar-powered refrigerators for vaccine storage. Ultimately, closing the immunization gap requires global collaboration, local innovation, and unwavering commitment to protecting every child.
Puppy Diarrhea After Vaccinations: Normal or Cause for Concern?
You may want to see also
Explore related products






![]()
Vaccine Hesitancy Impact
Global vaccination rates reveal stark disparities, with some countries achieving near-universal coverage while others struggle to reach even half their populations. For instance, as of 2023, Portugal boasts a 95% vaccination rate for measles among children, whereas in the Democratic Republic of Congo, only 40% of children receive the same vaccine. These gaps are not merely statistical—they reflect deeper societal, economic, and cultural factors, with vaccine hesitancy emerging as a critical determinant of these differences. Understanding the impact of vaccine hesitancy is essential to addressing these inequities and improving global health outcomes.
Consider the resurgence of measles, a disease declared eliminated in many regions but now reappearing due to declining vaccination rates. In 2019, the World Health Organization reported a 300% increase in measles cases globally compared to 2018, largely driven by vaccine hesitancy in both high- and low-income countries. For example, in the United States, states with non-medical exemption policies have seen measles outbreaks among school-aged children, where vaccination rates drop below the 95% threshold required for herd immunity. This illustrates how localized hesitancy can undermine decades of progress, leaving entire communities vulnerable to preventable diseases.
The impact of vaccine hesitancy extends beyond individual health to strain healthcare systems and economies. During the COVID-19 pandemic, countries with high vaccine hesitancy experienced prolonged lockdowns, overwhelmed hospitals, and higher mortality rates. For instance, in countries like Bulgaria and Romania, where COVID-19 vaccine uptake was below 30%, healthcare systems collapsed under the weight of severe cases, leading to preventable deaths. Conversely, countries like Singapore and Canada, with vaccination rates above 80%, were able to reopen economies faster and minimize long-term health impacts. This highlights the economic and social costs of hesitancy, which ripple far beyond the unvaccinated.
Addressing vaccine hesitancy requires a multi-faceted approach tailored to local contexts. In France, for example, where skepticism toward vaccines is historically high, the government introduced mandatory vaccination for 11 diseases in 2018, coupled with public awareness campaigns. This led to a 5% increase in childhood vaccination rates within two years. Similarly, in Nigeria, community health workers were trained to engage with parents in rural areas, addressing misconceptions about polio vaccines and increasing coverage from 50% to 80% in targeted regions. These examples demonstrate that combining policy measures with culturally sensitive communication can effectively combat hesitancy.
Ultimately, the impact of vaccine hesitancy is a global challenge that demands urgent attention. It is not just about individual choices but about collective responsibility. By understanding the root causes of hesitancy—whether misinformation, historical mistrust, or systemic barriers—and implementing evidence-based strategies, we can bridge the vaccination gap. The goal is clear: to ensure that every person, regardless of where they live, has access to and confidence in life-saving vaccines. This is not just a public health imperative but a moral one.
Understanding Hepatitis B Vaccine: Doses, Schedule, and Protection
You may want to see also
Frequently asked questions
As of 2023, global COVID-19 vaccination rates vary widely. High-income countries have achieved over 80% full vaccination rates, while many low-income countries struggle to reach 20% due to limited access to vaccines and healthcare infrastructure.
Countries like Portugal, Singapore, and the United Arab Emirates have some of the highest COVID-19 vaccination rates, with over 90% of their populations fully vaccinated.
Differences in vaccination rates are primarily due to disparities in vaccine availability, healthcare infrastructure, government policies, public trust in vaccines, and socioeconomic factors.
Childhood vaccination rates for diseases like measles, polio, and diphtheria are generally higher than COVID-19 rates, with global coverage around 85%. However, disparities persist, with lower rates in Africa and parts of Asia.
Initiatives like COVAX aim to provide equitable access to vaccines, while organizations like WHO and UNICEF work to strengthen healthcare systems, address vaccine hesitancy, and improve distribution logistics.