The meningococcal vaccine is a crucial immunization designed to protect against meningococcal disease, a serious bacterial infection caused by the bacterium *Neisseria meningitidis*. This disease can lead to meningitis (inflammation of the brain and spinal cord membranes) and septicemia (blood poisoning), both of which can be life-threatening. There are several types of meningococcal vaccines available, each targeting specific strains of the bacteria. In the United States, the most commonly used vaccines are Menactra®, Menveo®, and Bexsero®, with Menactra® and Menveo® covering serogroups A, C, W, and Y, and Bexsero® primarily targeting serogroup B. Understanding which vaccine is appropriate depends on factors such as age, risk factors, and regional recommendations.
Explore related products

What You'll Learn
- Vaccine Names: Menactra, Menveo, Menomune, Bexsero, Trumenba
- Brand Variations: Different brands for specific strains and regions
- Common Terms: Meningitis vaccine, meningococcal conjugate vaccine
- Strain Coverage: A, C, W, Y, B strain-specific vaccines
- Usage Context: Routine immunization, outbreak control, travel requirements
![]()
Vaccine Names: Menactra, Menveo, Menomune, Bexsero, Trumenba
The meningococcal vaccine is known by several brand names, each with distinct characteristics and applications. Among the most recognized are Menactra, Menveo, Menomune, Bexsero, and Trumenba. These vaccines are designed to protect against different serogroups of the Neisseria meningitidis bacterium, which can cause severe infections like meningitis and septicemia. Understanding their differences is crucial for informed decision-making.
Menactra and Menveo are conjugate vaccines targeting serogroups A, C, W, and Y. Menactra is approved for individuals aged 9 months and older, while Menveo is licensed for those aged 2 months and older. Both require a single dose for most adolescents and adults, though certain high-risk groups may need boosters. Menactra is often preferred for its longer track record, while Menveo’s lower incidence of injection-site reactions makes it a favorable option for some. Menomune, in contrast, is a polysaccharide vaccine covering the same serogroups but is less commonly used due to its inferior immune response in young children. It is typically reserved for individuals aged 2 years and older in specific circumstances, such as during outbreaks or for travelers to high-risk areas.
Bexsero and Trumenba are unique as they target serogroup B, which is not covered by the A, C, W, and Y vaccines. Bexsero is approved for individuals aged 10 weeks to 25 years and requires a two-dose or three-dose series depending on age. Trumenba, licensed for ages 10 to 25, also follows a multi-dose schedule. These vaccines are particularly important for college students, military personnel, and those with compromised immune systems, as serogroup B is a common cause of meningococcal disease in these populations.
When choosing a meningococcal vaccine, consider age, risk factors, and serogroup prevalence in your region. For instance, adolescents typically receive Menactra or Menveo as part of routine immunization, while Bexsero or Trumenba may be recommended for additional protection against serogroup B. Always consult a healthcare provider to determine the most appropriate vaccine and dosing schedule. Proper vaccination not only safeguards individual health but also contributes to herd immunity, reducing disease transmission in communities.
New York Health Act: Forced Vaccination?
You may want to see also
![]()
Brand Variations: Different brands for specific strains and regions
The meningococcal vaccine is not a one-size-fits-all solution. Different brands target specific strains of the Neisseria meningitidis bacteria, which are categorized into serogroups (A, B, C, W, Y, and X). This specificity is crucial because the prevalence of these serogroups varies by region, age group, and even travel destination. For instance, Menactra and Menveo are conjugate vaccines that protect against serogroups A, C, W, and Y, making them suitable for regions where these strains are endemic. In contrast, Bexsero and Trumenba are designed specifically for serogroup B, which is more prevalent in certain countries like the UK and Canada.
When selecting a meningococcal vaccine, healthcare providers must consider the patient’s age, travel plans, and local epidemiological data. For example, infants and young children in the U.S. are typically vaccinated with Menactra or Menveo starting at 9 months of age, with a booster dose recommended at age 12–18. Travelers to the meningitis belt in sub-Saharan Africa, where serogroup A is common, may require a vaccine like MenAfriVac, which is tailored to this region. Dosage schedules also vary; Menactra is administered as a single dose for adolescents and adults, while Menveo may require two doses for optimal immunity in certain populations.
The brand of meningococcal vaccine chosen can also depend on availability and cost. In low-income countries, vaccines like MenAfriVac are often subsidized by global health organizations, making them more accessible. In contrast, serogroup B vaccines like Bexsero and Trumenba tend to be more expensive and may not be covered by insurance in all regions. This disparity highlights the importance of global vaccination programs in ensuring equitable access to life-saving vaccines.
Practical tips for patients include verifying which strains are prevalent in their area or travel destination before vaccination. For instance, students entering college dormitories in the U.S. are often advised to receive a serogroup B vaccine due to the increased risk of outbreaks in close-quarter settings. Additionally, travelers should consult a healthcare provider at least 4–6 weeks before departure to ensure adequate time for vaccination and immune response. Understanding these brand variations empowers individuals to make informed decisions about their health and protection against meningococcal disease.
RSV Vaccine: Live or Dead? Understanding Its Composition and Safety
You may want to see also
![]()
Common Terms: Meningitis vaccine, meningococcal conjugate vaccine
The meningococcal vaccine is often referred to by several names, which can cause confusion for those seeking information. Two of the most common terms are "meningitis vaccine" and "meningococcal conjugate vaccine." While both terms are related, they are not interchangeable, and understanding the distinction is crucial for informed decision-making.
Analytical Perspective: The term "meningitis vaccine" is a broad reference, as meningitis can be caused by various pathogens, including bacteria, viruses, and fungi. Meningococcal disease, specifically, is caused by the bacterium *Neisseria meningitidis*. Therefore, the "meningitis vaccine" could refer to vaccines targeting different pathogens, whereas the "meningococcal conjugate vaccine" specifically targets *N. meningitidis*. This vaccine is designed to protect against meningococcal groups A, C, W, and Y, with some formulations also covering group B. The conjugate vaccine is particularly effective because it prompts the immune system to produce a stronger, longer-lasting response by linking the meningococcal polysaccharides to a carrier protein.
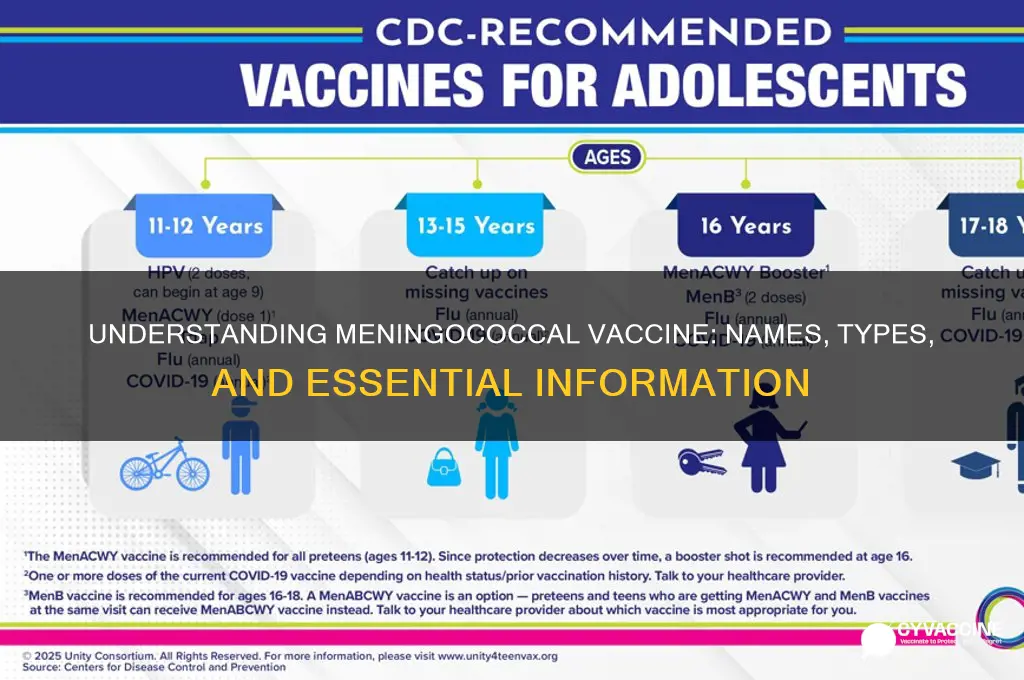
Instructive Approach: For parents and individuals, knowing which vaccine is appropriate is essential. The meningococcal conjugate vaccine (MenACWY) is typically recommended for adolescents aged 11–12 years, with a booster dose at age 16. Additionally, certain high-risk groups, such as college students living in dormitories, military recruits, and individuals with complement deficiencies or asplenia, may require earlier or additional doses. The MenB vaccine, which targets group B, is often recommended as a series of two or three doses for those at increased risk, such as individuals with specific medical conditions or during outbreaks. Always consult a healthcare provider to determine the appropriate vaccine and schedule based on age, risk factors, and regional guidelines.
Comparative Insight: While both terms are used, "meningococcal conjugate vaccine" is more precise and scientifically accurate. The "meningitis vaccine" could mistakenly imply coverage against all forms of meningitis, which is not the case. For instance, the pneumococcal conjugate vaccine (PCV) protects against *Streptococcus pneumoniae*, another cause of bacterial meningitis, but it is distinct from the meningococcal vaccine. Understanding these differences ensures that individuals receive the correct protection against specific pathogens. Moreover, the conjugate technology used in the meningococcal vaccine enhances its efficacy compared to older polysaccharide vaccines, making it a preferred choice for public health programs.
Practical Tips: When discussing vaccination with healthcare providers, use the specific term "meningococcal conjugate vaccine" to avoid ambiguity. Be aware of the different formulations available, such as MenACWY and MenB, and inquire about the recommended schedule for yourself or your child. Keep vaccination records updated, as some countries or institutions may require proof of meningococcal vaccination for activities like college enrollment or travel. Lastly, stay informed about local outbreaks or changes in vaccination guidelines, as these may influence the need for additional doses or specific types of meningococcal vaccines.
Takeaway: Clarity in terminology is key to ensuring proper vaccination against meningococcal disease. While "meningitis vaccine" is a common shorthand, "meningococcal conjugate vaccine" provides the precision needed to identify the correct immunization. By understanding these terms and their implications, individuals can make informed decisions to protect themselves and their loved ones from this potentially life-threatening infection.
Mastering Market Analysis: A Comprehensive Guide for Vaccine Development
You may want to see also
![]()
Strain Coverage: A, C, W, Y, B strain-specific vaccines
Meningococcal vaccines are tailored to combat specific strains of the Neisseria meningitidis bacterium, which is responsible for meningococcal disease. Among the most common strains are A, C, W, Y, and B, each requiring a distinct or combined vaccine approach. Understanding these strain-specific vaccines is crucial for effective prevention, especially in regions with varying disease prevalence.
Analytical Perspective:
The meningococcal vaccines targeting strains A, C, W, and Y are often combined into a single quadrivalent conjugate vaccine, commonly referred to as MenACWY. This vaccine is highly effective in preventing invasive meningococcal disease caused by these strains. For instance, the MenACWY-CRM (Menveo) and MenACWY-D (Menactra) vaccines are approved for individuals aged 2 years and older, with a standard dose of 0.5 mL administered intramuscularly. Adolescents and young adults, particularly those living in close quarters like college dormitories, are often prioritized for vaccination due to their higher risk of infection. In contrast, strain B requires a separate vaccine, such as MenB-FHbp (Trumenba) or MenB-4C (Bexsero), as it does not respond to the same antigens targeted by MenACWY vaccines.
Instructive Approach:
For optimal protection, healthcare providers recommend a two-dose series of MenACWY for adolescents, with the first dose administered at age 11–12 and a booster at age 16. In certain high-risk scenarios, such as outbreaks or travel to endemic areas like the meningitis belt in sub-Saharan Africa, a single dose may suffice for short-term protection. For strain B, Trumenba requires three doses over 6 months, while Bexsero follows a two-dose schedule. It’s essential to follow the specific dosing regimen for each vaccine, as deviations can compromise immunity. Parents and caregivers should consult healthcare providers to determine the appropriate vaccine and schedule based on age, risk factors, and local guidelines.
Comparative Insight:
While MenACWY vaccines offer broad protection against four strains, the MenB vaccines are more specialized and typically reserved for higher-risk populations. For example, MenB vaccines are often recommended for individuals with complement deficiencies, asplenia, or those exposed during an outbreak. The choice between Trumenba and Bexsero may depend on availability, cost, and provider preference, though both have demonstrated efficacy in clinical trials. Unlike MenACWY, which is often included in routine immunization schedules, MenB vaccines are usually administered on a case-by-case basis, highlighting the need for personalized vaccination strategies.
Practical Tips:
To ensure maximum benefit, individuals should be aware of potential side effects, such as soreness at the injection site, fatigue, or mild fever, which are generally short-lived. Scheduling vaccinations during periods of lower academic or work demands can minimize disruption. Additionally, keeping a record of vaccine doses and dates is crucial for tracking compliance and future boosters. For travelers to high-risk regions, verifying vaccination status and carrying documentation can expedite border crossings and ensure preparedness. Finally, staying informed about local disease trends and vaccine updates empowers individuals to make proactive health decisions.
Takeaway:
Strain-specific meningococcal vaccines are a cornerstone of disease prevention, with MenACWY and MenB vaccines addressing distinct serogroups. Tailoring vaccination plans to individual needs, following recommended schedules, and staying informed are key to maximizing protection against this potentially life-threatening disease.
Rabies Vaccine for South Africa: Essential Precaution or Optional Protection?
You may want to see also
![]()
Usage Context: Routine immunization, outbreak control, travel requirements
The meningococcal vaccine, commonly referred to as the MenACWY or MenB vaccine depending on the serogroups it covers, plays a critical role in preventing meningococcal disease, a severe bacterial infection that can lead to meningitis and sepsis. Its usage spans routine immunization, outbreak control, and travel requirements, each context demanding specific strategies and considerations.
Routine Immunization is the backbone of meningococcal disease prevention. In many countries, adolescents are the primary target group due to their heightened risk of infection. The MenACWY vaccine, which protects against serogroups A, C, W, and Y, is typically administered as a single dose at age 11–12, with a booster dose at age 16. For the MenB vaccine, a two-dose series is often recommended for infants and adolescents, depending on regional guidelines. Pregnant individuals and those with certain medical conditions, such as complement deficiencies or asplenia, may also require vaccination. Ensuring high coverage rates in these groups is essential to maintaining herd immunity and reducing disease transmission.
During outbreak control, the meningococcal vaccine becomes a rapid-response tool. Outbreaks often occur in crowded settings like college campuses or military barracks, where the disease spreads quickly. In such scenarios, public health officials may recommend mass vaccination campaigns with MenACWY or MenB vaccines, depending on the serogroup causing the outbreak. For example, during a serogroup B outbreak, the MenB vaccine (e.g., Bexsero or Trumenba) is prioritized. Vaccination efforts are often paired with antimicrobial prophylaxis for close contacts of infected individuals. Timely communication and accessibility of vaccines are critical to containing the outbreak and preventing further cases.
Travel requirements introduce another layer of complexity to meningococcal vaccine usage. Travelers to regions with high endemic rates, such as the meningitis belt in sub-Saharan Africa, are often required to receive the MenACWY vaccine. For instance, Saudi Arabia mandates proof of meningococcal vaccination for pilgrims participating in the Hajj or Umrah. Travelers should receive the vaccine at least 10–14 days before departure to ensure immunity. It’s also important to check specific country requirements, as some may demand additional documentation or specific vaccine brands. Consulting a travel health specialist can help ensure compliance and protection.
In all usage contexts, healthcare providers must balance vaccine availability, cost, and potential side effects. Common side effects, such as pain at the injection site or mild fever, are generally transient and manageable. However, rare but serious adverse events, like severe allergic reactions, require immediate medical attention. Public education campaigns can address hesitancy and emphasize the vaccine’s safety and efficacy. By tailoring vaccination strategies to the specific needs of routine immunization, outbreak control, and travel requirements, societies can effectively combat meningococcal disease and safeguard public health.
Patient-Supplied Vaccines: Billing Strategies for Healthcare Providers
You may want to see also
Frequently asked questions
The meningococcal vaccine is commonly referred to as MenACWY or MenB, depending on the specific type of vaccine.
Yes, there are two main types: MenACWY (protects against serogroups A, C, W, and Y) and MenB (protects against serogroup B).
Common brand names for the MenACWY vaccine include Menactra, Menveo, and MenQuadfi.
The meningococcal B vaccine is often referred to as Bexsero or Trumenba, depending on the manufacturer.
While the vaccines are known by their generic names (MenACWY and MenB), brand names may vary by country or region. Always check local health guidelines for specific names.