The MMR vaccine, which protects against measles, mumps, and rubella, is a crucial immunization typically administered in childhood. According to the Centers for Disease Control and Prevention (CDC), children should receive their first dose between 12 and 15 months of age, followed by a second dose between 4 and 6 years old. However, individuals who missed the vaccine during childhood or are unsure of their vaccination status can still receive it later in life. Adults born after 1956 who have no evidence of immunity or prior vaccination should consider getting the MMR vaccine, especially if they work in healthcare, education, or travel internationally. Additionally, women planning pregnancy should ensure they are immune to rubella, as it can cause severe complications in unborn babies. It’s essential to consult a healthcare provider to determine the appropriate timing and necessity of the MMR vaccine based on individual health history and risk factors.
| Characteristics | Values |
|---|---|
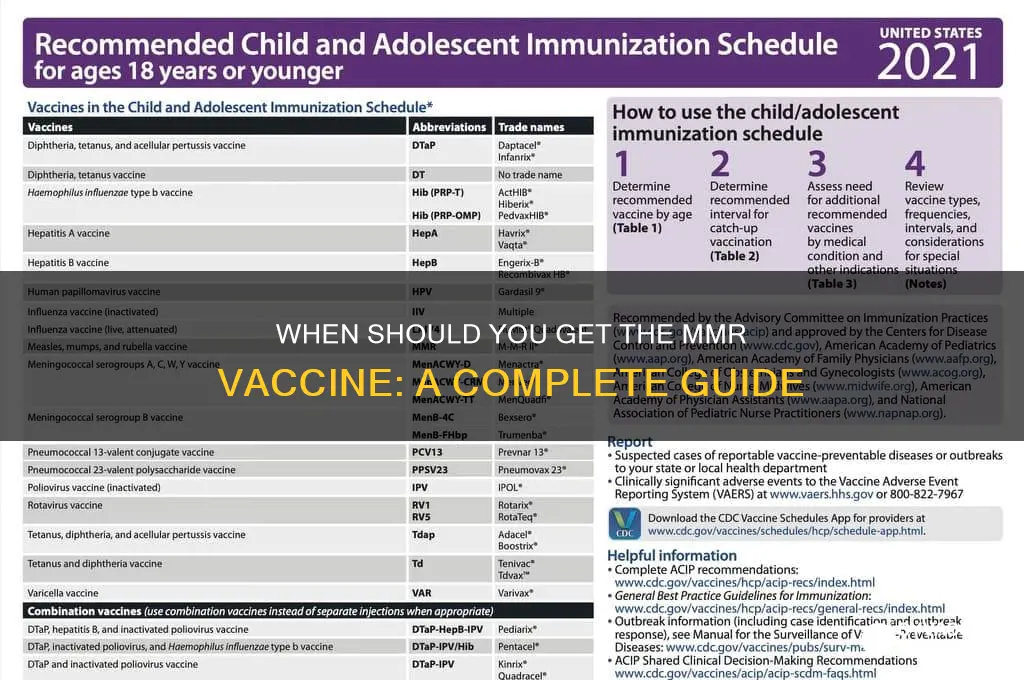
| Routine Vaccination Age | 12-15 months (first dose), 4-6 years (second dose) |
| Catch-Up Vaccination | Unvaccinated children and adults can receive the vaccine at any age |
| Adults Born After 1956 | Should receive at least one dose if not previously vaccinated |
| Healthcare Workers | Should have documented immunity or receive two doses |
| International Travelers | Ensure vaccination at least 2-3 weeks before travel |
| Pregnancy | Avoid MMR vaccine during pregnancy; defer until postpartum period |
| Breastfeeding | Safe to receive MMR vaccine while breastfeeding |
| Immunosuppressed Individuals | Consult healthcare provider; live vaccine may be contraindicated |
| HIV-Infected Individuals | Can receive MMR if CD4 count is sufficient; consult healthcare provider |
| Previous Severe Allergic Reaction | Avoid MMR if severe allergic reaction to neomycin or prior vaccine dose |
| Moderate or Severe Illness | Postpone vaccination until recovery |
| Interval Between Doses | Minimum 28 days between the first and second dose |
| Booster Doses | Generally not needed for most individuals; immunity is long-lasting |
| Vaccine Availability | MMR (measles, mumps, rubella) or MMRV (includes varicella) for children |
| Cost and Insurance Coverage | Covered by most insurance plans; available at low cost through programs |
| Side Effects | Mild fever, rash, or soreness at injection site (rare severe reactions) |
| Effectiveness | Over 97% effective after two doses |
Explore related products



$20.46 $21.95



What You'll Learn
- Infants: First dose at 12-15 months, second dose at 4-6 years
- Adults: Recommended if born after 1956 without evidence of immunity
- Travelers: Ensure vaccination before visiting regions with measles outbreaks
- Healthcare Workers: Mandatory MMR vaccination due to high exposure risk
- Outbreak Response: Accelerated vaccination schedules to control disease spread
![]()
Infants: First dose at 12-15 months, second dose at 4-6 years
The MMR vaccine schedule for infants is a carefully calibrated process, designed to provide optimal protection against measles, mumps, and rubella. At 12 to 15 months of age, a child's immune system is mature enough to respond effectively to the first dose of the vaccine. This initial dose triggers the production of antibodies, laying the foundation for long-term immunity. However, a single dose is not sufficient to guarantee full protection, which is why a second dose is recommended at 4 to 6 years of age. This booster shot reinforces the immune response, ensuring that the child is well-protected as they enter school and are exposed to a wider range of potential pathogens.
From a practical standpoint, parents should schedule the first MMR dose during the child's routine 12- to 15-month check-up. This appointment often includes other vaccinations, such as Hib and pneumococcal conjugate vaccines, streamlining the process. The second dose, given at 4 to 6 years, typically coincides with the child's pre-school or kindergarten enrollment. It’s essential to adhere to this timeline, as delays can leave the child vulnerable during critical developmental stages. If a dose is missed, consult a healthcare provider to determine the best catch-up schedule, as the MMR vaccine can be administered at any age after 12 months.
Comparatively, the MMR schedule for infants differs from that of adults or older children, who may receive the vaccine in a shorter timeframe if needed. For infants, the extended interval between doses is intentional, allowing the immune system to mature and respond more robustly. This approach maximizes efficacy while minimizing the risk of adverse reactions. Parents should also be aware that the MMR vaccine is often combined with the varicella (chickenpox) vaccine in some regions, creating a MMRV vaccine. While convenient, this combination may have slightly different dosing guidelines, so it’s crucial to follow the healthcare provider’s recommendations.
A persuasive argument for adhering to the 12-15 months and 4-6 years schedule lies in the vaccine’s proven track record. Since its introduction, the MMR vaccine has drastically reduced the incidence of measles, mumps, and rubella worldwide. For instance, measles cases have declined by over 99% in countries with high vaccination rates. By following this schedule, parents not only protect their child but also contribute to herd immunity, safeguarding vulnerable populations who cannot be vaccinated. Delaying or skipping doses undermines this collective effort, increasing the risk of outbreaks and severe complications, such as encephalitis or congenital rubella syndrome.
In conclusion, the MMR vaccine schedule for infants—first dose at 12-15 months and second dose at 4-6 years—is a scientifically backed strategy to ensure robust immunity against three highly contagious diseases. Parents play a pivotal role in adhering to this timeline, protecting not only their child but also the broader community. Practical steps, such as scheduling vaccinations during routine check-ups and staying informed about regional vaccine variations, can simplify the process. By prioritizing timely immunization, families can help maintain the progress made in eradicating these preventable diseases.
San Diego Vaccine Registration: A Step-by-Step Guide to Sign Up
You may want to see also
Explore related products






![]()
Adults: Recommended if born after 1956 without evidence of immunity
Adults born after 1956 face a unique health consideration: they may lack immunity to measles, mumps, and rubella (MMR). This isn't a generational quirk but a direct result of evolving vaccination practices. Before 1957, widespread MMR vaccination didn't exist, leaving many individuals susceptible. Unlike younger generations routinely immunized in childhood, this cohort often slipped through the cracks, relying on natural exposure for immunity. However, with declining disease prevalence due to vaccination, that natural immunity pathway has largely disappeared, leaving a gap in protection.
The recommendation is clear: adults born after 1956 without documented evidence of immunity should receive at least one dose of the MMR vaccine. "Evidence of immunity" includes written documentation of adequate vaccination, laboratory confirmation of immunity, or a history of laboratory-confirmed disease. Without this proof, a single dose of MMR vaccine is sufficient for most adults. This isn't just a precautionary measure; it's a critical step in preventing outbreaks and protecting both individual and community health.
For healthcare workers, international travelers, and students in post-secondary educational institutions, the stakes are even higher. These groups face increased exposure risks and are often required to have two doses of the MMR vaccine, spaced at least 28 days apart. This ensures a robust immune response, reducing the likelihood of infection and transmission. Pregnant women, however, should avoid the MMR vaccine, as it’s a live attenuated vaccine. Planning vaccination before pregnancy is ideal, as rubella infection during pregnancy can cause severe birth defects.
Practical considerations matter. The MMR vaccine is safe and effective, with minimal side effects such as fever, mild rash, or temporary joint pain. It’s typically administered as a subcutaneous injection, often in the upper arm. Adults can receive it at their primary care provider’s office, local health department, or pharmacy. Cost shouldn’t be a barrier; most insurance plans cover the vaccine, and programs like the Vaccines for Children (VFC) program offer assistance for eligible individuals.
In a world where vaccine-preventable diseases are reemerging, this recommendation isn’t just about personal health—it’s about collective responsibility. Adults born after 1956 without evidence of immunity play a pivotal role in maintaining herd immunity. By getting vaccinated, they not only protect themselves but also safeguard vulnerable populations, such as infants too young to be vaccinated and immunocompromised individuals. It’s a small step with a significant impact, ensuring a healthier future for all.
Is the Polio Vaccine FDA-Approved? Facts and Safety Explained
You may want to see also
Explore related products






![]()
Travelers: Ensure vaccination before visiting regions with measles outbreaks
Measles outbreaks in various regions pose a significant risk to unvaccinated travelers, turning dream vacations into potential health nightmares. The MMR (Measles, Mumps, Rubella) vaccine is your shield against this highly contagious disease, which can lead to severe complications like pneumonia and encephalitis. Before embarking on international travel, especially to areas with known measles activity, ensuring you're adequately protected is crucial.
Health organizations like the CDC recommend that all travelers aged 6 months and older receive the MMR vaccine. This is particularly vital for those visiting developing countries where measles remains endemic.
Dosage and Timing: The MMR vaccine is typically given in two doses. The first dose is administered at 12-15 months of age, followed by a second dose at 4-6 years. However, for travelers who haven't completed the series or are unsure of their vaccination status, catching up is essential. Adults born after 1956 who lack documented evidence of immunity should receive at least one dose of MMR. If traveling imminently, the second dose can be given as early as 4 weeks after the first.
Practical Tips: Check the measles outbreak situation in your destination countries through reliable sources like the WHO or CDC websites. Consult a healthcare professional well in advance of your trip (ideally 4-6 weeks) to discuss your vaccination needs and receive any necessary doses. Carry your vaccination record with you when traveling, as some countries may require proof of immunization.
Beyond the immediate health risks, traveling without adequate measles protection can have broader consequences. Outbreaks can spread rapidly within communities, affecting vulnerable populations like infants too young to be vaccinated and individuals with compromised immune systems. By ensuring your own vaccination, you contribute to herd immunity, protecting those who cannot be vaccinated themselves. Remember, responsible travel includes safeguarding not only your health but also the well-being of the communities you visit.
Parental Rights Act: Impact on Vaccination Decisions and Public Health
You may want to see also
Explore related products






![]()
Healthcare Workers: Mandatory MMR vaccination due to high exposure risk
Healthcare workers are on the front lines of disease prevention and treatment, yet they often face heightened exposure to infectious pathogens, including measles, mumps, and rubella (MMR). Given this risk, mandatory MMR vaccination for this group is not just a policy—it’s a critical safeguard for both providers and patients. The Centers for Disease Control and Prevention (CDC) recommends that all healthcare workers receive two doses of the MMR vaccine, with the first dose administered at least 28 days before the second. This regimen ensures robust immunity, reducing the likelihood of outbreaks in healthcare settings where vulnerable populations, such as immunocompromised patients, are at greater risk.
Consider the practical implications: a single unvaccinated healthcare worker exposed to measles could unknowingly transmit the virus to dozens of patients before symptoms appear. Measles, in particular, is one of the most contagious diseases, with a 90% transmission rate among unvaccinated individuals in close contact. Mumps and rubella, while less severe in most cases, can still lead to complications like meningitis or congenital rubella syndrome in pregnant women. Mandatory vaccination policies not only protect healthcare workers but also create a herd immunity effect within healthcare facilities, minimizing the spread of these diseases to the broader community.
Implementing such a policy requires clear guidelines and logistical planning. Healthcare employers should verify immunity status through documentation of prior vaccination or serologic testing for immunity. For those without immunity, the MMR vaccine should be administered as soon as possible, with the second dose following 4–8 weeks later. It’s essential to address concerns about vaccine safety, as the MMR vaccine has a well-established record of efficacy and minimal side effects, typically limited to mild fever or rash. Employers can further support compliance by offering on-site vaccination clinics and educational sessions to dispel myths and emphasize the collective benefits.
Critics might argue that mandatory vaccination infringes on personal autonomy, but the ethical imperative to protect patients outweighs individual preferences in this context. Healthcare workers have a professional duty to prioritize patient safety, and vaccination is a cornerstone of that responsibility. Moreover, exemptions should be limited to medical contraindications, such as severe allergies to vaccine components, and not extended to non-medical or philosophical objections. By framing mandatory MMR vaccination as a standard of care, healthcare institutions can foster a culture of accountability and trust.
In conclusion, mandatory MMR vaccination for healthcare workers is a proactive measure that addresses their unique exposure risks while safeguarding public health. It combines scientific evidence, practical implementation, and ethical considerations to create a safer healthcare environment. As infectious diseases continue to pose global threats, such policies serve as a model for how targeted interventions can yield widespread benefits. Healthcare workers, by leading the way in vaccination compliance, reinforce their role as stewards of community health.
Texas Duck Vaccine: Real Experiences and Outcomes Shared
You may want to see also
Explore related products



![]()
Outbreak Response: Accelerated vaccination schedules to control disease spread
During a disease outbreak, the standard vaccination schedule may not suffice to curb rapid transmission. Accelerated schedules, which shorten the interval between doses, become a critical tool in outbreak response. For the MMR vaccine, typically given as two doses 28 days apart, this interval can be reduced to a minimum of 3 days in emergency situations. This strategy, endorsed by the WHO, aims to rapidly increase population immunity, creating a firewall against further spread. However, this approach requires careful planning to ensure vaccine supply, trained personnel, and community trust, as deviations from standard schedules may raise concerns.
Implementing an accelerated MMR schedule demands precision. For instance, in a measles outbreak, children aged 6–11 months, who are usually vaccinated at 12 months, may receive an early dose. This dose, however, does not replace the routine 12-month shot, as immunity from early vaccination can wane. Adults without proof of immunity should receive two doses, with the second dose administered 4 weeks after the first, though the 3-day minimum interval applies in dire circumstances. Clear communication is essential to avoid confusion, such as emphasizing that accelerated doses are temporary measures, not permanent changes to the vaccination calendar.
The success of accelerated schedules hinges on logistical readiness and community engagement. Health systems must ensure sufficient vaccine stockpiles, cold chain maintenance, and rapid deployment capabilities. Mobile clinics, school-based campaigns, and community outreach can expedite coverage. Equally important is addressing hesitancy through transparent messaging about the safety and necessity of expedited dosing. For example, explaining that the MMR vaccine’s efficacy is not compromised by shorter intervals can reassure parents and caregivers. Without these dual pillars—logistics and trust—even the most aggressive schedule will fall short.
Comparing accelerated schedules to routine immunization highlights their trade-offs. While routine schedules optimize individual immunity with spaced doses, accelerated regimens prioritize collective protection during crises. For instance, a study during a 2017 measles outbreak in Minnesota demonstrated that rapid vaccination of 6,000 individuals within weeks significantly reduced case counts. However, such campaigns strain resources and risk overwhelming healthcare systems if not coordinated effectively. Thus, accelerated schedules are not a one-size-fits-all solution but a targeted intervention, reserved for scenarios where the threat of rapid disease spread outweighs the benefits of adhering to standard timelines.
In conclusion, accelerated MMR vaccination schedules are a powerful yet nuanced tool in outbreak response. They require meticulous planning, clear communication, and a balance between individual and community needs. When executed effectively, they can swiftly halt disease transmission, saving lives and preventing broader public health crises. However, their success depends on recognizing them as emergency measures, not substitutes for routine immunization programs. As outbreaks become more frequent in an interconnected world, mastering this strategy is essential for global health security.
Vaccine Without Adjuvant: Understanding Its Importance and Impact on Immunity
You may want to see also
Frequently asked questions
The first dose of the MMR vaccine is typically recommended between 12 and 15 months of age.
Yes, a second dose of the MMR vaccine is recommended to ensure full immunity. It should be given between 4 and 6 years of age, before a child enters school.
Yes, adults who have not been vaccinated or are unsure of their vaccination status can receive the MMR vaccine. It’s especially important for those at risk of exposure, such as healthcare workers or international travelers.
The MMR vaccine should be delayed or avoided in individuals with severe allergies to vaccine components, pregnant women, or those with a weakened immune system. Consult a healthcare provider for personalized advice.
Yes, the MMR vaccine can be administered at the same time as other childhood vaccines, such as those for chickenpox or hepatitis A, as long as there are no contraindications.