The current vaccination level in the United States is a critical public health metric, reflecting the nation's progress in protecting its population against preventable diseases, particularly COVID-19. As of recent data, approximately 68% of the eligible U.S. population has completed the primary COVID-19 vaccination series, with booster doses administered to about 30% of those fully vaccinated. However, vaccination rates vary significantly by state, age group, and demographic, with disparities influenced by factors such as access to healthcare, vaccine hesitancy, and socioeconomic conditions. Monitoring these levels is essential for understanding herd immunity, reducing hospitalizations, and guiding public health policies to address ongoing challenges like vaccine inequity and emerging variants.
Explore related products

$11.93 $21.99





What You'll Learn
![]()
Overall Vaccination Rates
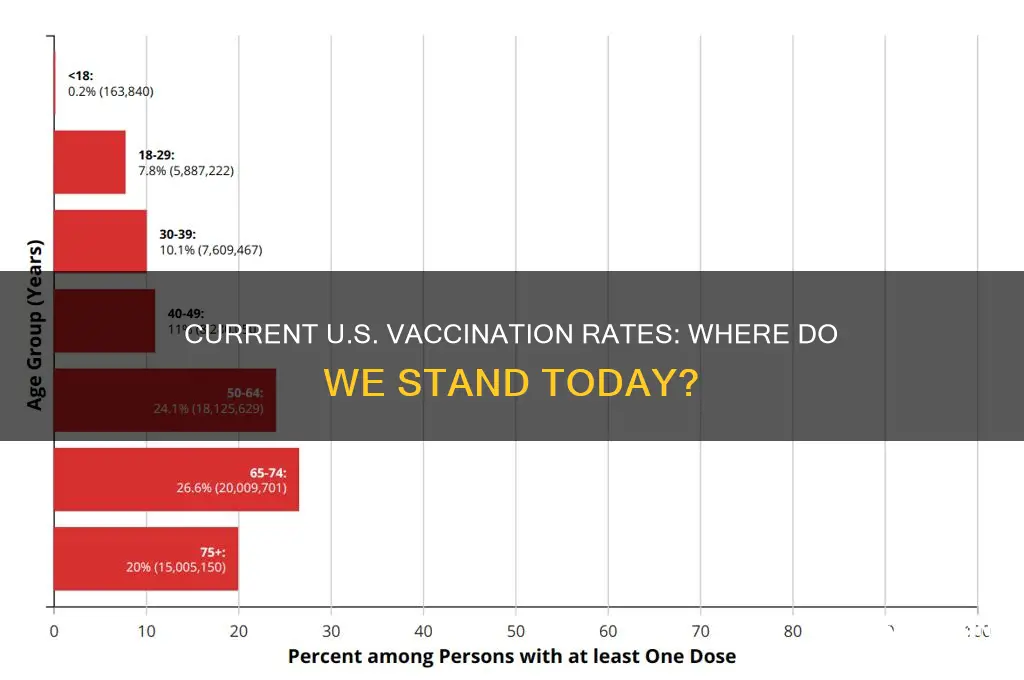
As of the latest data, the United States has administered over 670 million doses of COVID-19 vaccines, with approximately 79% of the eligible population (ages 5 and older) having received at least one dose. This figure highlights a significant public health achievement but also reveals disparities in vaccination rates across demographics and regions. For instance, while 93% of adults aged 65 and older have received at least one dose, only 60% of adolescents aged 12–17 are fully vaccinated, underscoring the need for targeted outreach in younger populations.
Analyzing these numbers reveals a complex landscape. Urban areas consistently report higher vaccination rates compared to rural regions, where access to healthcare and vaccine hesitancy remain barriers. For example, states like Vermont and Connecticut boast vaccination rates above 80%, while states like Mississippi and Alabama lag behind at around 55%. These disparities are further exacerbated by socioeconomic factors, with lower-income communities often facing challenges such as transportation and misinformation. Addressing these gaps requires localized strategies, such as mobile clinics and community-led education campaigns.
From a practical standpoint, understanding overall vaccination rates is crucial for public health planning. For parents, ensuring children receive their full series of COVID-19 vaccines (typically two doses for Pfizer-BioNTech, with a booster recommended for ages 12 and older) is essential. Employers can contribute by offering paid time off for vaccine appointments and hosting on-site vaccination clinics. Public health officials should prioritize data-driven approaches, such as mapping unvaccinated hotspots and deploying resources accordingly. For individuals, staying informed about booster recommendations—currently advised every 6 months for high-risk groups—is key to maintaining immunity.
Comparatively, the U.S. vaccination rate trails behind countries like Portugal (92% fully vaccinated) and Singapore (93%), but surpasses global averages, particularly in low-income nations where vaccine access remains limited. This global context underscores the importance of equitable distribution and international collaboration. Domestically, the U.S. can learn from successful campaigns in high-performing states by replicating their strategies, such as Vermont’s use of local pharmacies and community partnerships. By studying these examples, policymakers can refine efforts to increase overall vaccination rates and protect public health more effectively.
J&J Vaccine: Effective Against Indian Variants?
You may want to see also
Explore related products






![]()
Age Group Vaccination Coverage
As of the latest data, vaccination coverage in the United States varies significantly across age groups, reflecting both public health successes and ongoing challenges. For instance, among children aged 2, coverage for the measles, mumps, and rubella (MMR) vaccine stands at approximately 91%, a testament to decades of immunization campaigns. However, this rate drops to around 70% for adolescents aged 13–17 when considering the human papillomavirus (HPV) vaccine, highlighting disparities in vaccine uptake for newer immunizations. These variations underscore the need for targeted strategies to address age-specific barriers to vaccination.
Analyzing adult vaccination rates reveals further disparities. For adults aged 65 and older, influenza vaccination coverage hovers around 68%, while pneumococcal vaccine coverage is even lower, at roughly 60%. These figures are concerning, given that older adults are at higher risk for severe complications from these diseases. In contrast, younger adults aged 18–49 show lower overall vaccination rates, with only about 40% receiving the annual flu vaccine. This gap suggests that public health messaging and accessibility issues disproportionately affect this demographic, necessitating innovative outreach methods.
A comparative look at COVID-19 vaccination rates by age group provides additional insights. As of recent reports, over 90% of seniors aged 65 and older have received at least one dose, compared to approximately 75% of adults aged 18–64. While these numbers reflect the success of targeted campaigns for older populations, they also reveal a stagnation in uptake among younger adults. Booster dose coverage further amplifies this divide, with only about 40% of eligible adults aged 18–49 having received an updated booster, compared to 70% of those over 65. This trend highlights the importance of addressing vaccine hesitancy and logistical barriers in younger age groups.
To improve age group vaccination coverage, practical steps must be taken. For children and adolescents, integrating vaccine education into school curricula and offering on-site vaccination clinics can increase accessibility. Adults, particularly younger populations, may benefit from workplace vaccination programs and digital reminders. For seniors, partnering with community centers and healthcare providers to offer mobile clinics can bridge gaps in access. Additionally, addressing misinformation through trusted sources and culturally tailored messaging is critical across all age groups.
In conclusion, age group vaccination coverage in the United States is a mosaic of achievements and areas for improvement. By understanding the unique challenges each demographic faces—whether logistical, informational, or behavioral—public health initiatives can be tailored to maximize impact. Closing these gaps requires a combination of data-driven strategies, community engagement, and sustained investment in immunization infrastructure.
Understanding COVID-19 Vaccine Eligibility by Age Group: A Comprehensive Guide
You may want to see also
Explore related products






![]()
Regional Vaccination Disparities
As of the latest data, the United States has administered over 670 million COVID-19 vaccine doses, with approximately 79% of the population having received at least one dose. However, this national average masks significant regional disparities in vaccination rates, which are influenced by factors such as socioeconomic status, access to healthcare, and local attitudes toward vaccines. For instance, states in the Northeast, like Vermont and Connecticut, boast vaccination rates above 85%, while Southern states like Mississippi and Alabama lag behind, with rates below 60%. These disparities highlight the need for targeted interventions to address regional challenges.
Consider the rural-urban divide, a critical factor in vaccination disparities. Urban areas, with higher population densities and more healthcare facilities, often have higher vaccination rates. In contrast, rural regions face barriers such as limited access to vaccination sites, lower healthcare provider density, and higher rates of vaccine hesitancy. For example, in rural counties of states like Wyoming and Montana, vaccination rates can be as low as 40%, compared to urban centers like New York City, where rates exceed 90%. To bridge this gap, mobile vaccination clinics and community outreach programs have proven effective. These initiatives bring vaccines directly to underserved areas, offering convenience and addressing logistical hurdles.
Another layer of disparity emerges when examining racial and ethnic differences within regions. In the South, where Black and Hispanic populations are disproportionately represented, vaccination rates among these groups often trail those of white populations. Historical mistrust of the medical system, compounded by systemic inequities in healthcare access, contributes to this gap. For instance, in Georgia, only 45% of Black residents are fully vaccinated, compared to 55% of white residents. Tailored strategies, such as partnering with trusted community leaders and offering multilingual resources, can help mitigate these disparities. Additionally, addressing misinformation through culturally sensitive campaigns is crucial.
From a policy perspective, states with higher vaccination rates often share common strategies, such as robust public awareness campaigns and mandates for certain populations. For example, California and New York have implemented vaccine requirements for healthcare workers and students, contributing to their higher vaccination rates. In contrast, states without such mandates, like Florida and Texas, have seen slower uptake. Policymakers in regions with lower vaccination rates can learn from these examples by adopting evidence-based policies and leveraging federal resources, such as funding from the American Rescue Plan, to support vaccination efforts.
Finally, understanding regional disparities requires a focus on actionable solutions. For individuals in underserved areas, practical steps include locating nearby vaccination sites through tools like the CDC’s VaccineFinder and inquiring about transportation assistance programs. Employers can play a role by offering paid time off for vaccination and hosting on-site clinics. At the community level, local organizations can partner with health departments to organize vaccination drives and disseminate accurate information. By addressing regional disparities with tailored, collaborative efforts, the U.S. can move closer to achieving equitable vaccination coverage nationwide.
BCG Vaccine Availability in the United States: What You Need to Know
You may want to see also
Explore related products






![]()
Booster Shot Uptake Trends
As of the latest data, booster shot uptake in the United States has plateaued, with approximately 50% of eligible individuals having received an additional dose following their primary vaccination series. This trend highlights a significant gap between initial vaccination enthusiasm and ongoing commitment to maintaining immunity. While the initial rollout saw millions lining up for their first and second doses, the momentum has waned, leaving public health officials concerned about waning immunity and the rise of new variants.
Analyzing the demographics, older adults aged 65 and above lead in booster uptake, with over 70% having received an additional dose. This group, most vulnerable to severe COVID-19 outcomes, has shown a clear understanding of the benefits of maintaining robust immunity. In contrast, younger adults aged 18–49 lag behind, with only about 40% opting for a booster. This disparity underscores the need for targeted campaigns that address hesitancy and misinformation in younger populations, emphasizing the role of boosters in preventing long-term health complications and community spread.
From a practical standpoint, scheduling a booster shot is straightforward. Individuals are eligible for a booster 5 months after completing their Pfizer or Moderna primary series, or 2 months after a Johnson & Johnson dose. Most pharmacies and healthcare providers offer walk-in appointments, and the CDC’s VaccineFinder tool can help locate nearby sites. For those unsure about which booster to get, the CDC recommends an mRNA vaccine (Pfizer or Moderna) for optimal protection, regardless of the initial vaccine type.
Comparatively, booster uptake in the U.S. trails behind countries like Canada and the U.K., where aggressive public health campaigns and streamlined access have driven higher participation rates. For instance, Canada’s use of mobile clinics and workplace vaccination drives has made boosters more convenient, a strategy the U.S. could emulate to close its immunity gap. Additionally, incentivizing boosters through partnerships with local businesses or offering paid time off for vaccination could reignite interest.
In conclusion, while booster shot uptake in the U.S. has stagnated, there are clear pathways to reinvigorate participation. By focusing on underserved demographics, simplifying access, and learning from international successes, the nation can bolster its defenses against COVID-19. Staying up-to-date with vaccinations isn’t just a personal health decision—it’s a collective step toward ending the pandemic.
Vaccination Methods: A Global Comparison
You may want to see also
Explore related products






![]()
Vaccine Hesitancy Impact Analysis
As of the latest data, approximately 67% of the U.S. population is fully vaccinated against COVID-19, with significant disparities across age groups, regions, and socioeconomic demographics. While this figure reflects progress, it also highlights the persistent challenge of vaccine hesitancy, which continues to impede herd immunity and strain healthcare systems. Analyzing the impact of vaccine hesitancy reveals a complex interplay of public health, economic, and social consequences, underscoring the urgency of addressing this issue.
Understanding the Scope of Hesitancy
Vaccine hesitancy manifests in various forms, from outright refusal to delayed acceptance or selective uptake. For instance, while 90% of adults aged 65 and older are fully vaccinated, only 50% of adolescents aged 12–17 have completed their primary series. This disparity is not merely a numbers game; it translates to higher hospitalization rates among younger, unvaccinated populations, as evidenced by CDC data showing that unvaccinated individuals are 10 times more likely to be hospitalized with COVID-19. Such trends illustrate how hesitancy disproportionately affects specific age groups, amplifying risks within vulnerable communities.
Economic and Healthcare Burdens
The economic toll of vaccine hesitancy is staggering. Unvaccinated individuals account for a disproportionate share of COVID-19 hospitalizations, with a single hospitalization costing an average of $20,000. Multiply this by the thousands of preventable cases each month, and the financial strain on healthcare systems becomes clear. For example, Kaiser Family Foundation estimates that preventable COVID-19 hospitalizations among unvaccinated adults cost the U.S. healthcare system $13.8 billion between June 2021 and November 2022. Beyond direct costs, hesitancy perpetuates workforce disruptions, as outbreaks in unvaccinated populations lead to absenteeism and reduced productivity.
Strategies to Mitigate Hesitancy
Addressing vaccine hesitancy requires tailored, evidence-based approaches. Community-based initiatives, such as mobile vaccination clinics in underserved areas, have proven effective in increasing uptake. For instance, a program in rural Kentucky achieved a 20% increase in vaccination rates by partnering with local churches and offering on-site doses after services. Similarly, leveraging trusted messengers—such as primary care physicians or community leaders—can counteract misinformation. A study in *JAMA* found that personalized messages from healthcare providers increased vaccination intent by 15% among hesitant individuals. Practical tips include hosting Q&A sessions with experts, providing clear information about side effects (e.g., mild fatigue post-dose), and emphasizing the long-term benefits of vaccination, such as reduced risk of long COVID.
Long-Term Implications and Collective Responsibility
The impact of vaccine hesitancy extends beyond immediate health outcomes, shaping the trajectory of public health preparedness. As new variants emerge, lower vaccination rates create fertile ground for mutations, potentially rendering existing vaccines less effective. This underscores the need for a collective approach, where individuals, policymakers, and healthcare providers collaborate to build trust and disseminate accurate information. For example, incentivizing vaccination through workplace programs or school-based campaigns can normalize the behavior, while addressing systemic barriers like access to transportation or flexible appointment times ensures equity. Ultimately, reducing hesitancy is not just a medical imperative but a societal one, requiring sustained effort to protect both individual and community well-being.
Locate Your Vaccination Records Easily with CVS: A Quick Guide
You may want to see also
Frequently asked questions
As of 2023, approximately 68-70% of the U.S. population has received at least one dose of a COVID-19 vaccine, with about 65-67% fully vaccinated.
Vaccination rates vary significantly by state, with states like Vermont and Connecticut having rates above 80%, while states like Mississippi and Alabama have rates below 55%.
Approximately 30-35% of the U.S. population has received at least one COVID-19 booster shot as of 2023.
Yes, vaccination rates are highest among older adults, with over 90% of individuals aged 65 and older fully vaccinated, compared to about 60% of those aged 18-49.
The U.S. vaccination rate is higher than the global average, which stands at around 60% fully vaccinated, but lags behind some countries like Canada and several European nations.