The current vaccination rate in the United States is a critical metric for assessing public health efforts, particularly in the context of the ongoing COVID-19 pandemic. As of recent data, the Centers for Disease Control and Prevention (CDC) reports that approximately 68% of the eligible U.S. population has been fully vaccinated against COVID-19, with over 79% having received at least one dose. However, vaccination rates vary significantly by state, age group, and demographic, with higher rates among older adults and lower rates among younger populations and certain communities. Booster shot uptake has also been a focus, with about 48% of fully vaccinated individuals having received an additional dose. These figures highlight both the progress made and the challenges remaining in achieving widespread immunity and reducing the spread of the virus.
Explore related products




$12.79 $19.95


What You'll Learn
- State-by-State Vaccination Rates: Variations in vaccination coverage across different U.S. states
- Age Group Vaccination Trends: Breakdown of vaccination rates by age demographics in the U.S
- Vaccine Type Distribution: Percentage of U.S. population vaccinated with mRNA vs. other vaccines
- Booster Shot Uptake: Current rate of booster dose administration among eligible Americans
- Vaccination Disparities: Racial, ethnic, and socioeconomic gaps in U.S. vaccination rates
![]()
State-by-State Vaccination Rates: Variations in vaccination coverage across different U.S. states
As of the latest data, the United States exhibits significant disparities in vaccination rates across its states, reflecting a complex interplay of socioeconomic, cultural, and political factors. For instance, Vermont boasts one of the highest vaccination rates, with over 78% of its population fully vaccinated, while Mississippi lags behind at approximately 50%. These variations are not merely numbers; they represent real-world implications for public health, from outbreak susceptibility to healthcare system strain. Understanding these differences is crucial for policymakers and health advocates aiming to bridge the immunization gap.
Analyzing the data reveals distinct trends. Northeastern states like Vermont, Massachusetts, and Connecticut consistently lead in vaccination coverage, often attributed to higher education levels, robust public health infrastructure, and proactive local leadership. In contrast, Southern states such as Mississippi, Alabama, and Louisiana struggle with lower rates, influenced by factors like vaccine hesitancy, limited access to healthcare, and lower population density in rural areas. Age also plays a role; states with older populations, such as Maine and Florida, prioritize vaccinations for seniors, while younger demographics in states like Utah and Texas may skew overall rates downward.
To address these disparities, targeted strategies are essential. For states with low vaccination rates, mobile clinics and community-based initiatives can improve access, particularly in rural or underserved areas. Public awareness campaigns tailored to local cultures and languages can combat misinformation and build trust. For example, partnering with religious leaders or local influencers in hesitant communities has proven effective in states like West Virginia. Additionally, incentivizing vaccination through programs like lottery drawings or discounts has shown promise in states like Ohio.
A comparative analysis highlights the impact of policy decisions. States with strong mandates or incentives, such as California’s requirement for healthcare workers to be vaccinated, tend to have higher coverage. Conversely, states with political resistance to public health measures often face greater challenges. For instance, Florida’s inconsistent messaging and opposition to mandates correlate with its below-average vaccination rate. This underscores the need for bipartisan cooperation and evidence-based policies to drive equitable immunization efforts.
In practical terms, individuals can contribute by staying informed about local vaccination resources and encouraging peers to get vaccinated. Parents should ensure their children are up-to-date on routine immunizations, as pediatric vaccination rates have dipped in some states during the pandemic. Employers can play a role by offering paid time off for vaccine appointments or hosting on-site clinics. Ultimately, closing the state-by-state vaccination gap requires a multifaceted approach, combining data-driven strategies, community engagement, and policy support to protect public health nationwide.
Understanding Rabies Vaccine Lot Numbers: Character Count Explained
You may want to see also
Explore related products






![]()
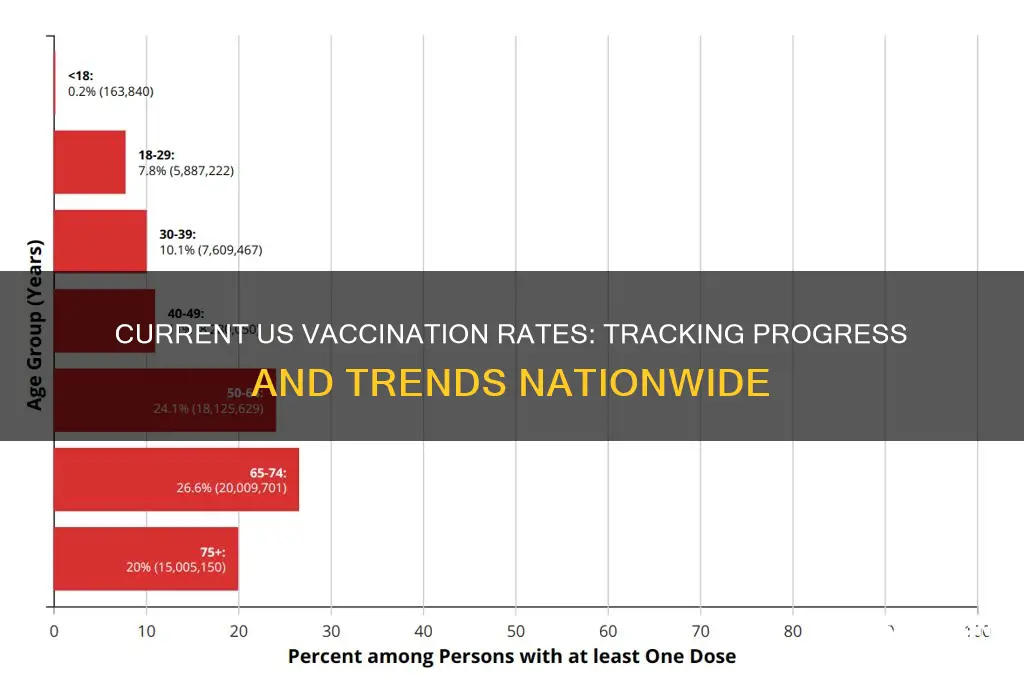
Age Group Vaccination Trends: Breakdown of vaccination rates by age demographics in the U.S
As of the latest data, vaccination rates in the U.S. vary significantly across age groups, reflecting both generational attitudes and access disparities. Adults aged 65 and older lead with a vaccination rate of approximately 90%, driven by heightened awareness of COVID-19 risks and targeted outreach efforts. In contrast, adolescents aged 12–17 lag behind at around 60%, influenced by parental hesitancy and lower perceived risk. This breakdown underscores the importance of age-specific strategies to address gaps and ensure equitable protection.
Analyzing these trends reveals a clear pattern: vaccination rates decline with decreasing age. Young adults aged 18–29, for instance, hover around 70%, while children under 12, who became eligible later, show a rate of roughly 40%. This gradient highlights the impact of eligibility timelines, misinformation, and varying levels of community engagement. For example, school-based vaccination drives have boosted rates among younger teens, while college campuses have struggled to reach consistent uptake due to transient student populations.
To bridge these gaps, tailored approaches are essential. For older adults, maintaining high rates involves addressing booster hesitancy through clear messaging about waning immunity. Among younger demographics, leveraging social media campaigns and peer influencers could combat misinformation. Parents of children under 12, often concerned about safety, benefit from pediatrician-led education emphasizing the vaccine’s rigorous testing and minimal side effects. Practical tips include scheduling family vaccination appointments together and using local health department resources for age-specific guidance.
Comparatively, the 30–49 age group, with a rate of around 75%, serves as a middle ground. This cohort, balancing work and family responsibilities, often cites time constraints as a barrier. Employers can play a pivotal role here by offering on-site vaccination clinics and paid time off for appointments. Meanwhile, addressing the 50–64 group (80% vaccinated) requires focusing on chronic conditions, as this demographic is more likely to have comorbidities that increase COVID-19 risks.
In conclusion, understanding age-specific vaccination trends is critical for refining public health strategies. From prioritizing booster campaigns for seniors to combating hesitancy in younger populations, each age group demands unique interventions. By dissecting these patterns and implementing targeted solutions, the U.S. can move closer to achieving comprehensive vaccine coverage and mitigating the pandemic’s impact across generations.
J&J Vaccine: Effective Shield Against Omicron?
You may want to see also
Explore related products






![]()
Vaccine Type Distribution: Percentage of U.S. population vaccinated with mRNA vs. other vaccines
As of the latest data, the U.S. vaccination landscape is dominated by mRNA vaccines, specifically Pfizer-BioNTech and Moderna, which account for over 90% of all administered doses. This overwhelming preference for mRNA technology raises questions about the distribution and uptake of other vaccine types, such as Johnson & Johnson’s viral vector vaccine. Understanding this breakdown is crucial for assessing public health strategies, addressing hesitancy, and ensuring equitable access to diverse vaccine options.
Analytically, the mRNA vaccines’ dominance can be attributed to their early availability, high efficacy rates (around 95% for Pfizer and Moderna in clinical trials), and the two-dose regimen that aligns with traditional vaccination schedules. In contrast, the Johnson & Johnson vaccine, a single-dose option, initially gained traction for its convenience but faced setbacks due to rare blood clot concerns and production issues. As a result, only about 7% of the U.S. vaccinated population received this vaccine. This disparity highlights the impact of public perception, regulatory actions, and logistical challenges on vaccine distribution.
From an instructive perspective, individuals seeking vaccination should consider their specific needs when choosing between mRNA and other vaccines. For instance, mRNA vaccines are recommended for most age groups, including adolescents as young as 12 (Pfizer) and 18 (Moderna), with a standard two-dose series spaced 3–4 weeks apart. The Johnson & Johnson vaccine, while less commonly used, remains a viable option for those seeking a single-dose solution or with mRNA contraindications. Practical tips include checking local availability, consulting healthcare providers for personalized advice, and staying updated on booster recommendations, as mRNA boosters are now widely encouraged for sustained immunity.
Comparatively, the mRNA vaccines’ near-monopoly in the U.S. contrasts sharply with global vaccine distribution, where viral vector and inactivated vaccines (e.g., AstraZeneca, Sinovac) play significant roles. This difference underscores the influence of national regulatory approvals, procurement strategies, and public trust in specific technologies. For example, while the U.S. prioritized mRNA vaccines, many European countries initially balanced their portfolios with AstraZeneca, reflecting varying risk assessments and supply chain priorities.
Persuasively, diversifying vaccine type distribution could strengthen the U.S. immunization strategy by addressing niche needs and building resilience against supply disruptions. Encouraging uptake of non-mRNA options, such as Novavax’s protein-based vaccine (recently approved for adults), could appeal to those hesitant about newer technologies. Policymakers should also consider targeted campaigns for underserved populations, where single-dose or non-mRNA options might be more accessible or culturally acceptable. By broadening the vaccine mix, the U.S. can enhance flexibility, equity, and public confidence in its vaccination efforts.
Italy's Vaccine Verification Process: How Officials Check Your Proof
You may want to see also
Explore related products

$14.95 $16.95





![]()
Booster Shot Uptake: Current rate of booster dose administration among eligible Americans
As of the latest data, approximately 48% of eligible Americans have received at least one booster dose of the COVID-19 vaccine. This figure highlights a significant gap between initial vaccination rates and booster uptake, raising questions about the factors driving this disparity. While over 80% of the U.S. population aged 5 and older have completed their primary vaccine series, booster rates lag, particularly among younger adults and certain demographic groups. This trend underscores the need for targeted strategies to encourage booster shots, which are critical for maintaining immunity against evolving variants.
Analyzing the data reveals stark differences in booster uptake across age groups. Among adults aged 65 and older, booster rates exceed 70%, reflecting a strong awareness of the heightened risk for severe illness in this population. In contrast, only about 30% of adults aged 18–49 have received a booster, despite this group comprising a significant portion of the eligible population. This disparity suggests that younger adults may perceive themselves as less vulnerable, even though boosters are essential for reducing transmission and preventing breakthrough infections. Public health campaigns must address these misconceptions and emphasize the collective benefits of widespread booster uptake.
Practical barriers also contribute to lower booster rates. Many Americans report confusion about eligibility, with frequent updates to guidelines creating uncertainty. For instance, the CDC recommends a second booster for individuals aged 50 and older and those with immunocompromising conditions, but awareness of these specifics remains low. To improve uptake, healthcare providers should proactively communicate personalized recommendations during routine visits. Additionally, expanding access to booster clinics in workplaces, schools, and community centers could remove logistical hurdles for busy individuals.
Persuasively, the case for boosters extends beyond individual protection. As immunity wanes over time, unvaccinated and under-vaccinated populations remain at risk, perpetuating the virus’s spread. Boosters not only reduce the likelihood of severe illness but also lower the viral load in breakthrough cases, decreasing transmission. This dual benefit makes boosters a cornerstone of public health strategy, particularly as new variants emerge. Policymakers and health advocates must reframe boosters as a civic responsibility, akin to the initial vaccine rollout, to shift public perception and drive higher uptake.
In conclusion, while the current booster shot uptake among eligible Americans is modest, targeted interventions can bridge the gap. By addressing age-based disparities, clarifying eligibility guidelines, and emphasizing the broader societal impact, public health efforts can encourage more individuals to receive their booster doses. Practical steps, such as streamlined communication and accessible vaccination sites, will be key to achieving this goal. As the pandemic evolves, boosters remain a vital tool in safeguarding both personal and community health.
Is the COVID-19 Vaccine Mandatory in the United States?
You may want to see also
Explore related products






![]()
Vaccination Disparities: Racial, ethnic, and socioeconomic gaps in U.S. vaccination rates
As of the latest data, the overall COVID-19 vaccination rate in the U.S. hovers around 68% for fully vaccinated individuals, with booster rates significantly lower. However, these numbers mask deep disparities that reveal a troubling reality: vaccination rates are not evenly distributed across racial, ethnic, and socioeconomic lines. For instance, while 73% of Asian Americans are fully vaccinated, only 56% of Black Americans and 62% of Hispanic Americans have received their full vaccine series. These gaps persist despite widespread vaccine availability, pointing to systemic barriers that extend beyond mere access.
Consider the socioeconomic factors at play. Low-income communities, often disproportionately composed of racial and ethnic minorities, face hurdles like limited transportation, inflexible work schedules, and a lack of nearby vaccination sites. For example, a single parent working multiple jobs may struggle to find time for a vaccine appointment, let alone deal with potential side effects that could mean missing a day of work. Practical solutions, such as mobile clinics in underserved neighborhoods or paid time off for vaccination, could help bridge this gap. Yet, these measures are inconsistently implemented, leaving many behind.
Racial and ethnic disparities also stem from historical and present-day mistrust in the healthcare system. Centuries of medical exploitation, from the Tuskegee Syphilis Study to forced sterilization, have left a legacy of skepticism among Black and Indigenous communities. Addressing this requires more than just providing information; it demands culturally sensitive outreach led by trusted community figures, such as local clergy or grassroots organizers. For instance, partnerships with Black churches during the COVID-19 vaccine rollout demonstrated how tailored approaches can increase uptake by 20% in some areas.
Language and technology barriers further exacerbate these disparities. Non-English speakers often struggle to navigate vaccine registration systems or understand health information, while older adults may lack digital literacy to schedule appointments online. A comparative analysis shows that states offering multilingual hotlines and in-person registration saw higher vaccination rates among immigrant populations. This highlights the need for inclusive strategies that meet people where they are, both linguistically and technologically.
Ultimately, closing these gaps requires a multifaceted approach that tackles systemic inequities head-on. Policymakers must invest in community-based initiatives, ensure equitable distribution of resources, and address the root causes of mistrust. For individuals, advocating for policies like paid vaccine leave or volunteering at local clinics can make a difference. The takeaway is clear: achieving true herd immunity means leaving no one behind, and that starts with confronting the disparities that persist in plain sight.
Vaccines and Agenda 21: Unraveling the Conspiracy Theory Connection
You may want to see also
Frequently asked questions
As of 2023, the vaccination rate in the USA varies by vaccine type. For COVID-19, approximately 68-70% of the eligible population has received at least one dose, while about 65-67% are fully vaccinated. Rates for other vaccines, like flu or childhood immunizations, differ and are typically reported by the CDC.
The USA's COVID-19 vaccination rate is comparable to many developed nations but lags behind countries like Canada, the UK, and several European nations. However, it is higher than many low- and middle-income countries.
Factors include vaccine accessibility, public health messaging, political and cultural beliefs, socioeconomic status, and geographic location. Hesitancy and misinformation also play significant roles.
Yes, vaccination rates vary widely by state. States with higher urbanization and stronger public health infrastructure tend to have higher rates, while rural or politically conservative states often have lower rates.
The CDC updates vaccination data regularly, often daily or weekly, for COVID-19. Data for other vaccines, such as childhood immunizations, is typically updated annually or quarterly.