At 15 months, infants typically receive a set of recommended vaccines as part of their routine immunization schedule, which is designed to protect them from serious and potentially life-threatening diseases. According to guidelines from organizations like the Centers for Disease Control and Prevention (CDC) and the World Health Organization (WHO), children at this age are advised to get vaccines such as the measles, mumps, and rubella (MMR) vaccine, the varicella (chickenpox) vaccine, and a booster dose of the diphtheria, tetanus, and acellular pertussis (DTaP) vaccine. Additionally, depending on regional recommendations and individual health needs, they may also receive vaccines for hepatitis A or influenza. These vaccinations are crucial for building immunity and ensuring long-term health, making the 15-month checkup a significant milestone in a child’s preventive care journey.
Explore related products






What You'll Learn
![]()
Recommended Vaccines at 15 Months
At 15 months, children are due for several critical vaccines that build on their earlier immunizations, ensuring continued protection against serious diseases. The Centers for Disease Control and Prevention (CDC) recommends a combination of booster shots and new vaccines at this age, tailored to strengthen a child’s immune system during a period of increased social interaction and exposure to pathogens. These vaccines include the fourth dose of DTaP (diphtheria, tetanus, and pertussis), the third or fourth dose of Hib (Haemophilus influenzae type b), and the final dose of the pneumococcal conjugate vaccine (PCV13). Each of these doses is crucial for maintaining immunity levels achieved in earlier months.
One standout vaccine at this stage is the measles, mumps, and rubella (MMR) vaccine, typically administered as a first dose at 12–15 months. This vaccine is a cornerstone of childhood immunization, preventing three highly contagious diseases that can lead to severe complications, including encephalitis, pneumonia, and lifelong disabilities. The MMR vaccine is given as a 0.5 mL intramuscular injection, often in the thigh for infants. Parents should be aware that mild side effects, such as fever or rash, may occur 7–12 days after vaccination, but these are normal immune responses and not cause for alarm.
Another critical vaccine at 15 months is the varicella (chickenpox) vaccine, which is often administered alongside MMR as the MMRV combination vaccine or as a standalone dose. Chickenpox, while often mild in children, can lead to serious complications like bacterial infections, dehydration, or, in rare cases, pneumonia. The varicella vaccine is 98% effective in preventing severe disease and is given as a 0.5 mL subcutaneous injection. Parents should ensure their child receives this vaccine, especially if they attend daycare or preschool, where the virus spreads easily.
Practical tips for parents include scheduling the 15-month vaccines during a well-child visit to minimize stress and ensure all doses are up to date. It’s also advisable to bring a favorite toy or snack to comfort the child during and after the appointment. While some children may experience soreness at the injection site or mild fever, these symptoms typically resolve within 24–48 hours. Over-the-counter pain relievers like acetaminophen can be used if needed, but aspirin should be avoided due to the risk of Reye’s syndrome.
In summary, the 15-month vaccine schedule is a vital phase in a child’s immunization journey, offering protection against diseases that were once common and often deadly. By adhering to the CDC’s recommendations—including DTaP, Hib, PCV13, MMR, and varicella vaccines—parents can safeguard their child’s health and contribute to community immunity. Staying informed and proactive ensures children receive the full benefits of these life-saving interventions.
Should You Stick to the Same Vaccine for Your Booster Shot?
You may want to see also
Explore related products






![]()
MMR and Varicella Vaccines
At 15 months, children typically receive a set of vaccines to protect against serious diseases, including the MMR (Measles, Mumps, and Rubella) and Varicella (Chickenpox) vaccines. These vaccines are often administered together in a single visit, streamlining the immunization process and ensuring timely protection. The MMR vaccine is given as a 0.5 mL dose, while the Varicella vaccine is administered as a 0.5 mL dose, both typically injected into the muscle of the thigh or upper arm. This combination approach not only reduces the number of injections but also aligns with the recommended immunization schedule, which emphasizes completing key vaccines by 18 months of age.
From an analytical perspective, the MMR and Varicella vaccines are crucial components of the 15-month immunization schedule due to the resurgence of vaccine-preventable diseases in recent years. Measles, for instance, has seen outbreaks in communities with low vaccination rates, highlighting the importance of maintaining herd immunity. The MMR vaccine is 97% effective after two doses, while the Varicella vaccine provides 90% protection against chickenpox and significantly reduces the risk of severe complications. Administering these vaccines together at 15 months ensures that children are shielded from these highly contagious diseases during their early, vulnerable years.
Instructively, parents should prepare for the 15-month vaccination appointment by scheduling it well in advance and ensuring their child is healthy on the day of the visit. Mild side effects, such as fever, fussiness, or soreness at the injection site, are common and can be managed with acetaminophen or a cool compress. It’s essential to follow the healthcare provider’s post-vaccination instructions and monitor the child for any unusual reactions. Keeping a record of the vaccines received is also critical for future medical reference and school enrollment requirements.
Persuasively, combining the MMR and Varicella vaccines at 15 months is not just a matter of convenience but a strategic public health measure. By protecting children against measles, mumps, rubella, and chickenpox simultaneously, this approach minimizes the risk of outbreaks and reduces the burden on healthcare systems. Parents play a pivotal role in this process by adhering to the recommended schedule and advocating for timely immunizations. Delaying or skipping these vaccines leaves children susceptible to diseases that can have severe, lifelong consequences, such as encephalitis from measles or pneumonia from chickenpox.
Comparatively, the 15-month MMR and Varicella vaccines differ from earlier immunizations in their focus on preventing highly contagious, airborne diseases. While vaccines like DTaP (Diphtheria, Tetanus, and Pertussis) target bacterial infections, MMR and Varicella address viral illnesses that spread rapidly in unvaccinated populations. This distinction underscores the importance of these vaccines in community-wide disease prevention. Additionally, the 15-month milestone marks a transition from infant to toddler immunizations, setting the stage for booster doses later in childhood.
Practically, parents can make the 15-month vaccination experience smoother by bringing a favorite toy or snack to comfort their child during the appointment. Dressing the child in loose-fitting clothing allows easy access to the injection site, and scheduling the visit earlier in the day can help manage potential side effects. After the vaccines, engaging in gentle activities and offering plenty of fluids can aid in recovery. By approaching this milestone with preparation and understanding, parents can ensure their child receives the full benefits of the MMR and Varicella vaccines.
Exploring the Global mRNA Vaccine Market: Trends, Growth, and Opportunities
You may want to see also
Explore related products






![]()
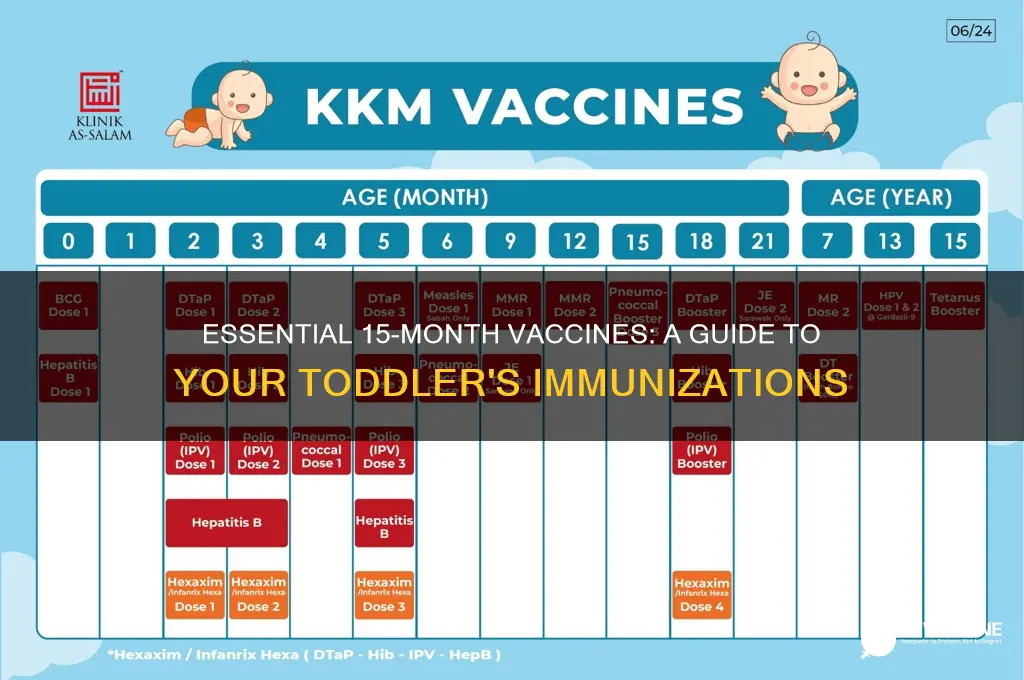
Booster Shots for Infants
By 15 months, infants have already received a series of primary vaccinations to protect against serious diseases like measles, mumps, rubella, and whooping cough. However, the immune response generated by these initial doses can wane over time, leaving children vulnerable. This is where booster shots come in—they reinforce immunity, ensuring continued protection during critical developmental stages. For instance, the MMR (Measles, Mumps, Rubella) vaccine typically requires a first dose around 12 months, with a booster administered between 15 and 18 months. Similarly, the DTaP (Diphtheria, Tetanus, Pertussis) vaccine follows a schedule that includes a fourth dose around 15 months to solidify immunity.
Administering booster shots at 15 months is a strategic decision based on immunological science. At this age, a child’s immune system is mature enough to mount a robust response to vaccines, yet young enough to benefit from early protection. For example, the Hib (Haemophilus influenzae type b) vaccine, which prevents meningitis and pneumonia, often requires a booster at 12–15 months to maintain antibody levels. Parents should consult their pediatrician to confirm the exact timing, as schedules may vary based on regional guidelines or individual health needs.
One common concern is the number of vaccines given at this visit, which can include boosters for DTaP, Hib, PCV13 (Pneumococcal), and MMR. While multiple shots in one visit may seem overwhelming, it’s important to note that this approach minimizes the number of clinic visits and ensures timely protection. To ease the process, parents can use distraction techniques, such as singing or bringing a favorite toy, and ask about numbing creams to reduce injection discomfort. After the appointment, mild fever or fussiness is normal and can be managed with acetaminophen as directed by a healthcare provider.
Comparing booster schedules across countries highlights the adaptability of vaccination programs. In the U.S., the CDC recommends a DTaP booster at 15 months, while some European countries may delay it slightly. These variations reflect differences in disease prevalence and healthcare infrastructure. Regardless of location, the core principle remains the same: boosters are essential to bridge immunity gaps and prevent outbreaks. For families traveling internationally, verifying that their child’s vaccinations align with destination requirements is crucial.
In conclusion, booster shots at 15 months are a cornerstone of pediatric immunization, ensuring sustained protection against preventable diseases. By understanding the science behind these doses, preparing for the appointment, and staying informed about regional guidelines, parents can confidently support their child’s health. While the process may seem daunting, the long-term benefits far outweigh the temporary discomfort, making boosters a vital step in a child’s developmental journey.
Medicare-Covered Vaccines: Essential Immunizations for Adult Health Protection
You may want to see also
Explore related products






![]()
Hepatitis A Vaccine Timing
At 15 months, a child’s vaccination schedule often includes the first dose of the hepatitis A vaccine, though timing can vary based on regional guidelines and risk factors. The Centers for Disease Control and Prevention (CDC) recommends this vaccine between 12 and 23 months of age, with a second dose administered 6 to 18 months later. This two-dose series provides long-term protection against hepatitis A, a liver infection caused by the hepatitis A virus, often spread through contaminated food or water. For parents, understanding this timing ensures their child is shielded during peak exposure risks, such as when starting daycare or traveling to endemic areas.
The decision to administer the hepatitis A vaccine at 15 months is both strategic and practical. By this age, infants have completed their initial series of routine vaccines, and their immune systems are robust enough to respond effectively. The 0.5 mL dose (for children aged 12 months to 2 years) is well-tolerated, with mild side effects like soreness at the injection site or low-grade fever being rare. Delaying the vaccine beyond 23 months is not ideal, as it leaves the child vulnerable during a critical developmental period. However, if missed, the vaccine can still be given later, though adherence to the recommended schedule is strongly encouraged.
Comparatively, the hepatitis A vaccine’s timing contrasts with other vaccines given at 15 months, such as the MMR (measles, mumps, rubella) or varicella (chickenpox) vaccines, which are part of a standardized schedule. Hepatitis A vaccination, however, is often influenced by individual risk assessments. For instance, children living in areas with high disease prevalence or those with chronic liver conditions may receive the vaccine earlier. This flexibility underscores the importance of consulting a pediatrician to tailor the vaccination plan to a child’s specific needs.
A persuasive argument for timely hepatitis A vaccination lies in its preventive efficacy. Hepatitis A outbreaks can occur in childcare settings, schools, or communities with poor sanitation, and the disease can lead to severe complications, especially in young children. Vaccination not only protects the individual but also contributes to herd immunity, reducing community transmission. Practical tips for parents include scheduling the vaccine during a routine 15-month checkup to minimize additional clinic visits and keeping a record of the vaccination date to ensure the second dose is administered on time.
In conclusion, the hepatitis A vaccine’s timing at 15 months is a critical component of a child’s immunization schedule, balancing developmental readiness with disease prevention. By adhering to the recommended timeline and dosage, parents can safeguard their child’s health against a preventable yet potentially serious infection. This proactive approach aligns with broader public health goals, making it a cornerstone of pediatric care.
When Do Chickenpox Vaccinations End? Age Limits Explained
You may want to see also
Explore related products






![]()
Vaccine Schedule Adjustments
At 15 months, a child’s vaccine schedule typically includes boosters for critical immunizations like MMR (measles, mumps, rubella), varicella (chickenpox), and DTaP (diphtheria, tetanus, pertussis). However, individual circumstances—such as travel plans, health conditions, or missed earlier doses—may require adjustments. For instance, a child traveling to a region with high measles prevalence might need an accelerated MMR dose before the standard 4-year booster. Pediatricians often assess these factors to tailor the schedule, ensuring protection without overloading the immune system.
Adjustments aren’t arbitrary; they follow evidence-based guidelines from organizations like the CDC or WHO. For example, if a child missed the 12-month hepatitis A vaccine, it can be administered at 15 months alongside other scheduled doses. However, spacing is crucial—some vaccines, like MMR and varicella, can be given simultaneously, while others, such as inactivated and live vaccines, may require a 4-week interval unless administered on the same day. Parents should communicate gaps or delays to their healthcare provider to ensure proper catch-up scheduling.
Health conditions also play a role in adjustments. Immunocompromised children might need alternative vaccine types or timing. For instance, the MMR vaccine is live-attenuated and may pose risks for severely immunocompromised individuals, requiring a delay or alternative approach. Similarly, preterm infants often follow a modified schedule, with some vaccines administered based on chronological age rather than corrected age. Always consult a pediatrician to balance protection with safety in these cases.
Practical tips can ease the process. Keep a detailed immunization record to track doses and due dates, especially if switching providers or traveling. Use appointment reminders to avoid missed doses, as delays can leave children vulnerable during critical developmental stages. For children with vaccine anxiety, discuss strategies like distraction techniques or numbing creams with your pediatrician. Finally, stay informed about regional outbreaks or new vaccine recommendations, as these may prompt earlier or additional doses.
In summary, vaccine schedule adjustments at 15 months are not one-size-fits-all. They depend on factors like missed doses, travel, health status, and regional risks. By working closely with healthcare providers and staying proactive, parents can ensure their child’s immunization plan remains effective and safe, adapting to unique needs without compromising protection.
Denmark's Vaccination Progress: Tracking the Number of Vaccinated Individuals
You may want to see also
Frequently asked questions
At 15 months, children usually receive 3-4 vaccines, including the MMR (Measles, Mumps, Rubella), Varicella (Chickenpox), Hib (Haemophilus influenzae type b), and Pneumococcal conjugate vaccine (PCV13), depending on the schedule and previous doses.
Yes, it is safe. The CDC and pediatricians confirm that receiving multiple vaccines at once does not overwhelm a child’s immune system and is an effective way to ensure timely protection against diseases.
Delaying or skipping vaccines increases the risk of preventable diseases. It’s best to follow the recommended schedule, but discuss any concerns with your pediatrician to make an informed decision.
Common side effects include mild fever, fussiness, tiredness, and soreness at the injection site. These are normal and usually resolve within a day or two. Contact your doctor if symptoms persist or worsen.